 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 3, Nov/Dec, 2011, pp. 86-93 Blood and body fluid exposures among surgeons in Mulago hospital T. Kimuli1, Denise Meya1, David Meya2, J. Tulsky3,W. Schecter4 1Dept of
Surgery, College of Health Sciences, Makerere
University Code Number: js11056 Background: It is now recognized that
health workers are at risk of acquiring infection with hepatitis B virus (HBV),
hepatitis C virus (HCV), HIV and other blood borne pathogens through contact
with infected blood and other body fluids. This study was aimed at determining
the frequency and circumstances of blood borne pathogen exposures among
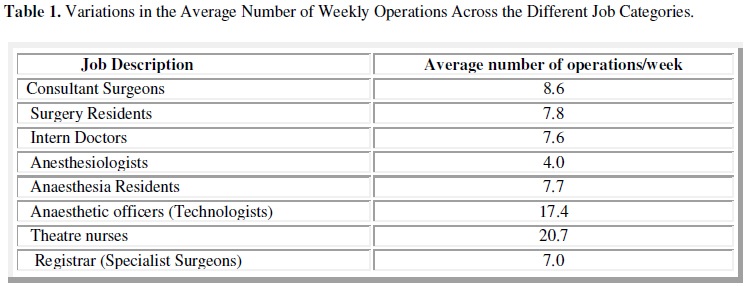
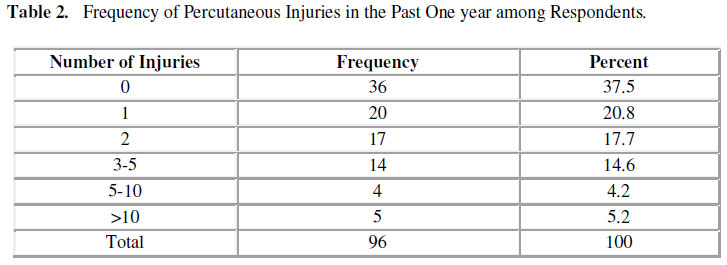
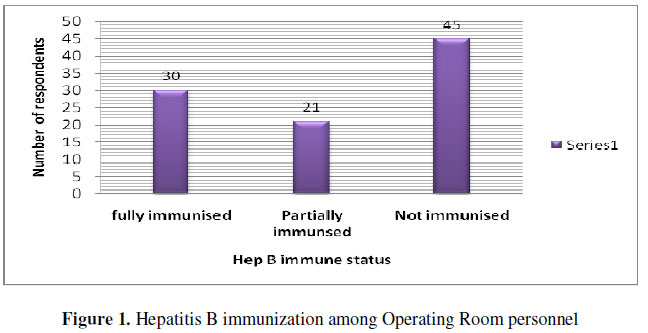
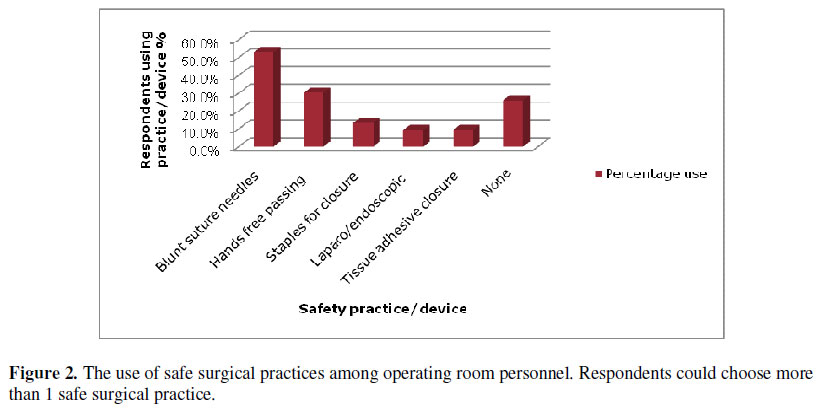
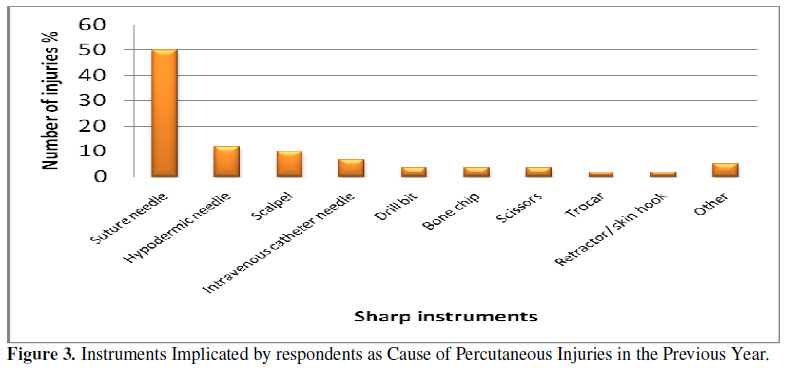
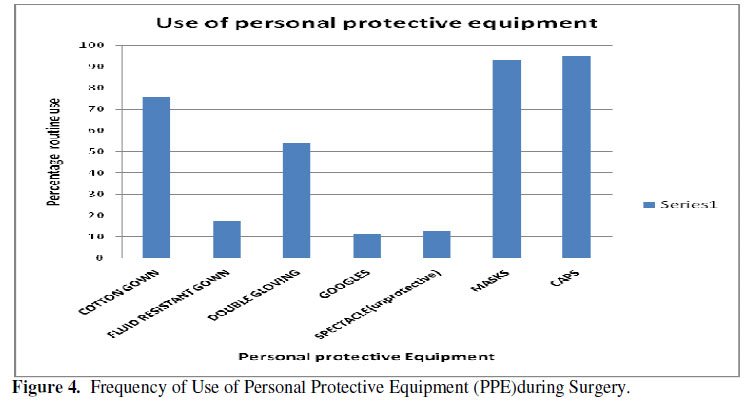
operating theatre personnel in Mulago Hospital. Introduction Recent global focus on the AIDS epidemic has resulted in increased recognition of the morbidity and mortality of occupationally acquired infections for health care workers (HCWs). Surgeons and other operating room personnel are at higher risks of infection with hepatitis B virus (HBV), hepatitis C virus (HCV), HIV and other blood borne pathogens through contact with blood and other body fluids1. In many Sub-Saharan African (SSA) countries with higher prevalence of these infections, occupationally acquired infections can shorten the careers of HCWs, especially surgeons. Half of all premature deaths in HCWs are projected over the next years to be due to occupationally acquired infections in sub-Saharan Africa2. Worldwide, of 35 million total HCWs, 3 million experience a needle stick every year; 70,000 of these will acquire hepatitis B, 15,000 hepatitis C, and 1,000 will acquire HIV. Of HCV, HBV, and HIV among HCWs, an estimated 40%, 37%, and 4% are occupationally acquired. The WHO also estimates that overall, 90% of needle-stick injuries occur in low and middle-income countries3. These projections, however, are based on very limited primary data from Africa. Nonetheless, the protection of HCWs is largely neglected, and these risks are a deterrent to recruiting, training, and retaining health workers--especially surgeons. Occupational risks are one of many causes of the global crisis in human resources in health, most pronounced in Africa, which is short of an estimated one million health workers and has only 2% of the world’s health workforce to cope with 25% of the global burden of disease4-6. In the United States, prospective observational studies of intraoperative exposure have shown that practices like double gloving, use of waterproof garments, face shields, and blunt suture needles reduced blood and body fluid contacts7-8. In developing countries, with no systematic study of occupational exposures to blood or body fluids among operating theatre personnel there is an overall need to determine the epidemiology of blood and body fluid contact among operating theatre and ascertain circumstances of exposure. This is compounded by the high rates of blood borne pathogens among the surgical patients hence high exposure rate9,10. The Centre for Disease Control and Prevention (CDC) recommendations for infection prevention against blood-borne pathogens during invasive procedures emphasize the prevention of needle-sticks and use of barriers to prevent muco-cutaneous exposures11. In sub-Saharan Africa, most health facilities lack basic protective equipment for their employees and operations are completed under extreme resource constraints that may increase risk of exposure, such as unreliable or marginally functional equipment, limited lighting and exposure, limited nursing assistance, and short anesthetic time that requires faster operations. Our findings in this study will be critical in supplying much needed preliminary data to support studies that aim at testing relevant interventions to reduce blood and body fluid exposures in the operating theatre. While occupational safety interventions worked in developed countries, it is not clear that these same solutions are either acceptable or affordable in low-income high HIV-prevalence countries. Research by academics who are passionate about their programs and the need to sustain the creative efforts of country personnel will help to answer questions about occupational safety. Preliminary Studies A recent retrospective study on needle stick injuries in Mbarara hospital (western Uganda) reported that 55% of health care workers had a needle stick injury (NSI) in the previous year, and there was an incidence of 1.86 NSI/HCW/year and an associated risk of 0.08% for HIV and 0.135% for HBV (per single NSI)12. Sero prevalence of HIV and HBV were 26% and 2.8% respectively. Interns had the highest risk of experiencing a NSI (mean 4.8 incidents/year). In addition, a cross-sectional study among obstetric nurses and midwives in Mulago Hospital, found a similar rate of exposure: Over 55% had a percutaneous injury over the last year, and the rate of NSIs was 4.3/person/year13. Only 18% reported not having any such injury in their entire career. This study identified lack of training as the most important risk factor for a NSI, followed by working > 40 hours/week, recapping needles most of the time, not using gloves when handling needles, and short professional experience, and other work-related factors (such working on surgical disciplines). A recent survey by Jagger et al17 in 2007 of 106 surgeons in East, Central, and Southern Africa which included 15 surgeons in Uganda, done at the annual regional surgical conference, showed that the operating room ranks very high as a setting for percutaneous injuries and blood exposures to HCWs. This study reported 3.1 percutaneous injuries per surgeon per year. Average experience of the surgeons was nearly 17 years; this is important as larger studies in the USA confirm that trainees (residents) have the highest rates of exposure, however, they were under-represented in this study11,15. Circumstances of percutaneous injuries were mainly during suturing, especially of skin and fascia. Inadequate use of preventive measures was notably associated with a high rate of risky exposures in the study. Other significant findings of this study were the very low rate of hepatitis B vaccination among surgeons, and the lack of personal protective equipment (PPE) for surgeons in Africa, especially eye goggles sealed above the eyes. A onetime surveillance of occupational exposures undertaken by surgical personnel in 2005 at Makerere University documented that 82.9% had ever been exposed, 70% of these had percutaneous exposure, 77% had knowledge of post exposure prophylaxis as an option to prevent HIV transmission (personal communication, KT2008). However, none of these studies included other theatre staff. While surgeons have been shown to have the highest exposure rate in observational studies in the USA, nurses also have a high exposure rate, and while exposure rates for anesthesia personnel are lower, they are often at higher risk due to injuries with hollow bore needles (i.e. while placing IV lines)11. Our study sought to address this important yet often overlooked group by documenting the frequency and circumstances of blood exposures in a group of African surgeons and theater personnel, and collecting data regarding their access to and use of protective equipment and preventive strategies for reducing occupational blood exposure. Subjects and Methods Survey forms were distributed to operating room personnel at their various stations in July 2008 in Mulago Hospital. Information relating to the study was provided at departmental meetings (in surgery, orthopedic and obstetrics and gynecology) that encouraged operating room personnel to complete and return the survey forms. The forms were collected after completion. Approval for the study was obtained from the University of San Francisco, California, Makerere University and the Uganda National Council of Science and Technology Research and Ethics Committees. Written consent was also obtained and responses were anonymous. The questionnaire solicited descriptive information from respondents including years in practice, weekly number of surgical procedures performed, and surgical specialty, as well as information about the use of PPE and injury-reducing practices and devices; hepatitis B vaccination status; and access/use of post exposure prophylaxis for HIV. Respondents described in detail their most recent sharp-device injury sustained during surgery, including the procedure being performed, the device that caused the injury, circumstances of the exposure, and extent of blood contamination of the device. They also described their most recent blood or body fluid exposure, including the procedure being performed, type of body fluid involved, location of fluid contact and PPE worn at time of exposure. Results Of 120 operating room personnel who were given survey forms 96 returned completed surveys giving a 78% response rate. Respondents included surgeons, surgical trainees, anaesthesia staff and nurses. Overall, the mean number of years in practice of respondents was 6.6 (SD 7.3). The most common job categories among respondents were general surgery residents (30%), registrars (17%) and interns (17%) Table 1 shows the variations in the average number of weekly operations across the different job categories. The respondents reported doing an average of 10.5 (SD 9.6) procedures per week. Forty seven percent of respondents had been fully vaccinated against hepatitis B virus. Of the remaining 53%, a total of 31% had completed part of the 3-dose vaccination series, and 22% had not begun. Figure 1 shows Hepatitis B immunization status among operating room personnel. Most (79%) of the respondents indicated that they had access to HIV post exposure prophylaxis (PEP). However, only 11.3% of the 62 respondents who had injuries reported utilizing the HIV post exposure prophylaxis service. Only 24% of 50 injured respondents (with access to PEP) reported utilizing the post exposure prophylaxis services. Figure 2 shows the use of safe surgical practices among operating room personnel. Respondents could choose more than 1 safe surgical practice. Sixty nine (71.9%) of 96 respondents used one and 27 of 96 (28.5%) respondents used at least two of the safe surgical techniques. Almost one-half (53%) of surgeons reported having used blunt suture needles, 30% used the hands-free technique for passing sharp instruments (Figure 2). The use of tissue adhesive—an alternative to using regular suturing that requires no sharp device—was reported by fewer (5) respondents. Respondents estimated the number of percutaneous injuries, other sharp-device injuries, and/or cuts sustained during the previous year. A total of 64% reported 1 or more percutaneous injuries (range, 0 to more than 10) in the past one year, and there was a mean (SD) of 3.2 (3.3) percutaneous injuries per operating theatre personnel per year CI 95% 2.5-3.9. Injuries were reported to be above average among consultants 5 (SD 4.5) and senior house officers 3.6 (SD 3.8). At least one injury in the past one year was reported by all Consultants, 75% of anaesthetic officers, 66.7% of theatre nurses, 62.5% of all interns and 60.7% of surgery residents (SHOs). In 66% of the incidents, the surgeons’ hands were in contact with the operative site when the injury occurred, a circumstance under which there is potential for both surgeon-to-patient blood contact and vice versa. However, in 59% of all incidents, the sharp instrument was visibly contaminated with blood before injuring the surgeon, hence patient- to-surgeon blood contact. In 68% of incidents there was actual bleeding post injury. The device most frequently responsible for the injury was a suture needle (accounting for 50% of percutaneous injuries). All injuries involved fingers. Pre-operative routine counseling and testing (RCT) for HIV as a policy was supported by 87.5% of respondents. Figure 3 shows instruments implicated by respondents as cause of percutaneous injuries incurred in the previous year. Suture needles were the commonest cause of injuries. Support for pre-operative RCT in 74 % of respondents was based on grounds that if the patient was HIV positive, the surgical team would take extra precautions during surgery and would be more apt to using personal protective gear. 4% of respondents said they would refuse to operate on HIV positive patients. Respondents estimated the number of BBF exposures to skin or mucous membranes that they sustained during the previous year; 68.75% reported 1 or more BBF exposures (range, 0-17), with a mean (SD) of 4.2(4.6) exposures per surgeon per year. The body site most frequently exposed was the eyes (38%), hands (27.3%), arm (12.6%),foot/leg (11.5%), nose/mouth (4%) and face (6%). In 59% of incidents, the surgeon was exposed to blood, and in another 16% the surgeon was exposed to blood-tainted body fluid. BBF exposures typically involved fluid making contact with an exposed area that was not protected by a barrier garment. Figure 4 Shows the frequency at which the respondents used personal protective equipment during surgical procedures in theatre. In reporting the PPE typically worn during surgery, 70 % of respondents indicated that they typically wore a gown for all surgical procedures. Cotton gowns were worn all the time in 86% and 14% reported using fluid resistant gowns sometimes. Significantly the routine use of eye protective equipment was abysmal. Only 24% of surgeons reported wearing some kind of eye protection all the time that is goggles (11.5%) and non-protective eye glasses (12.5%). Bearing in mind that all injuries involved hands, at time of injury 43 of 69 (62.3%) were wearing double pair of gloves, 21of 69 (30.4%) single pair and 5 of 69 (7.3%) none at time of injury Limitation of study Recall bias since respondents had to recall events over the past year which is quite a long period. Discussion A total of 64% reported 1 or more percutaneous injuries in the past one year, and there was a mean (SD) of 3.2 (3.3) percutaneous injuries per operating theatre personnel per year. CI 95% 2.5-3.9. This rate of exposure is not any different from that found in a similar survey done among African surgeons by Jagger14. Unlike in other studies, injuries were reported to be higher among the more experienced group namely the consultants 5 (SD 4.5) and surgery residents 3.6 (SD 3.8) as well as anaesthetic officers. This could partly be explained by pressure exerted by quite larger number of operations per week handled by these categories of personnel. Also noncompliance to accepted protective measures could also develop overtime.Just like in other similar studies suture needles were a leading cause of injuries. Therefore use of blunt suture needles as a safety practice could markedly lower this high injury rate. The rate of hepatitis B vaccination was alarmingly low. This finding was not surprising, because there is/has been no standardized Hepatitis B vaccination program for health workers in Uganda let alone for medical trainees which correlates well with what was reported previously in sub-Saharan Africa14. In addition to the importance of protecting surgeons, countries have an economic interest in protecting the resources invested while training the surgeons. Hepatitis B vaccination should be mandatory for all HCWs and medical trainees who have direct contact with patients. Vaccination should take place during their training to achieve high levels of immunity early in their careers. Knowledge of availability of HIV post-exposure prophylaxis was good. However, for unknown reasons, this service was underutilized. This was probably because those who had injury didn’t want to check their status due to the stigma attached to HIV. One of the most surprising findings was that 50% of respondents reported using blunt suture needles - a higher percentage than reported in some industrialized countries; for example, in the United States16, indicating a high level of awareness in a majority of African surgeons though they remain at unnecessarily high risk of injury. Just like other surveys in Africa14, results also indicate that fluid-resistant barrier garments are less frequently worn than cotton garments which soak body fluids and hold them next to the skin particularly around the sleeves. Cotton gowns which absorb fluid and hold it next to the skin may be more harmful, especially if the skin is not intact15. If worn in combination with a cotton gown a fluid-proof barrier, such as a plastic apron, provides inexpensive frontal protection. Fluid-resistant gowns would be even more protective. Just like in other studies in Africa14, the most exposed part of the body to splashes were the eyes coupled with significantly underutilized eye protection gear, despite the known possibility for the transmission of blood-borne pathogens through the eyes16-18. Standard eyeglasses though used more frequently than goggles provide inadequate protection, since they lack a seal above the eye19. The scarcity of adequate and safe surgical supplies is a major obstacle to African surgeons’ safety. Purchasing safety engineered devices and protective products may create additional expenses, and developing these items at cost-affordable prices should be a goal of manufacturers. Respondents’ frequent use of the hands-free passing technique, using a “neutral zone,”14 reflects the fact that they are motivated to minimize risk. This is a no-cost practice that, if widely adopted, could reduce the risk of injury for all surgical personnel, not just surgeons. Opportunities to educate African surgical personnel about the use of this technique should be actively pursued. One possible way of achieving this goal would be to offer an open-access, Internet-based training program. Surgeons in sub-Saharan Africa are keenly aware of the infection risks they face, and this survey identifies simple yet high-yield opportunities to improve their protection against occupation exposures. HCWs are not a scarce and valuable commodity, and they have a basic right to protection from preventable occupational diseases. Hospital administrators, national and international policy-makers, and HCWs must work collaboratively to realize this right. Acknowledgments We acknowledge the assistance received from Dr. Doruk Odzgez, Sudha Jayaraman and Infectious Disease Institute, Prof Jackline Tulsky and Prof Schecter. We extend special thanks to the operating theatre personnel who shared their experiences through this survey.. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11056f4.jpg] [js11056f3.jpg] [js11056t1.jpg] [js11056f2.jpg] [js11056f1.jpg] [js11056t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}