 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 3, Nov/Dec, 2011, pp. 94-101 Vascular Lesions Seen among Patients Treated at Muhimbili National Hospital in Dar es Salaam, Tanzania J. Moshy1, S. Owibingire1, S. Shaban2 1Dept. of Oral Surgery and Oral Pathology, Muhimbili
University of Health and Allied Sciences, Code Number: js11057 Background: Birthmarks
sometimes represent significant vascular anomalies that require diagnosis and
treatment. This study was aimed at determining the demographic and clinical pattern
of vascular lesions seen among patients attending The Oral and Maxillofacial Surgical
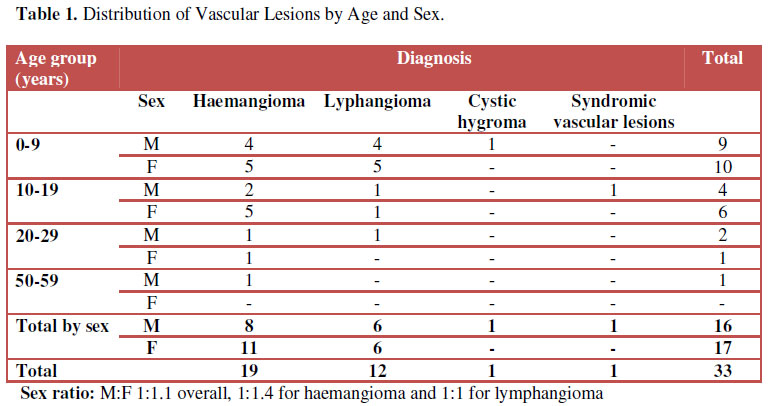
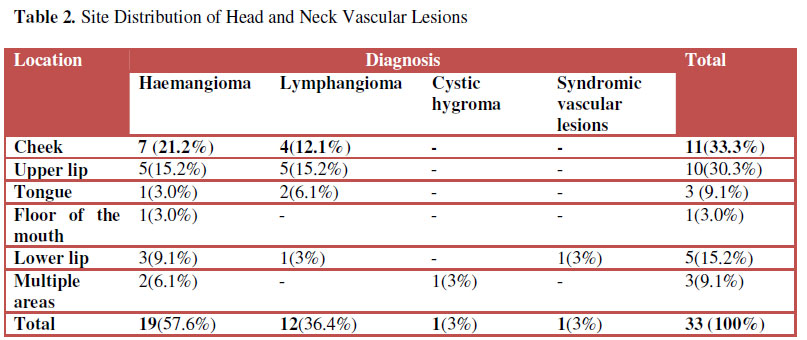
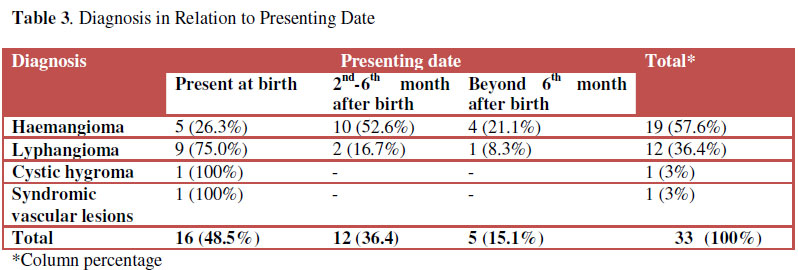
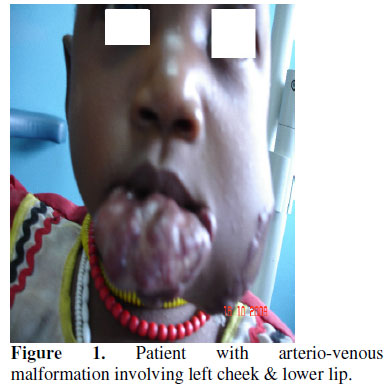
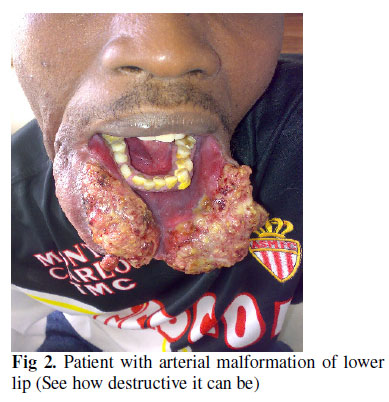
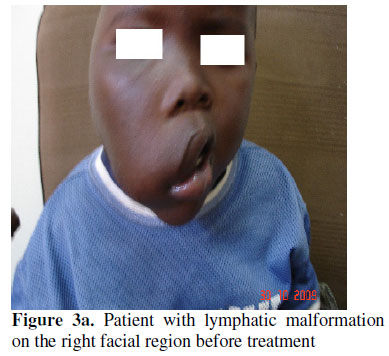
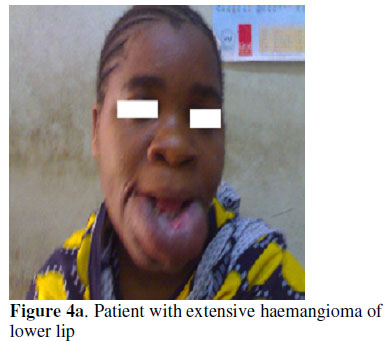
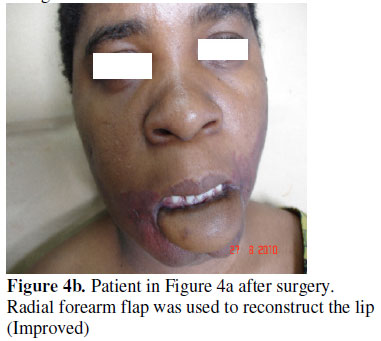
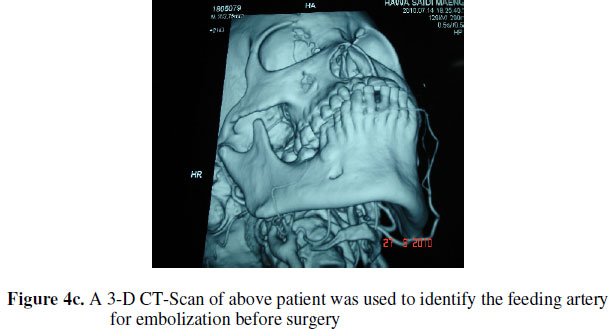
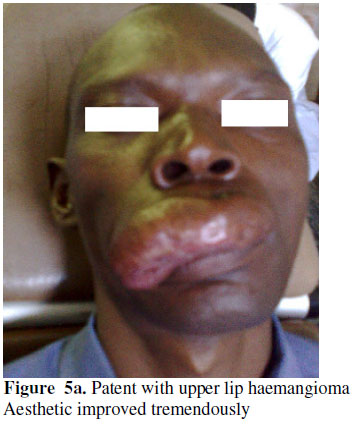
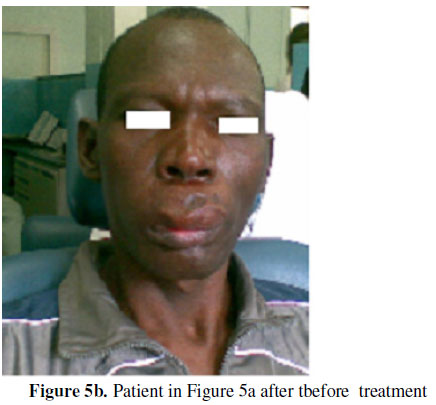
Clinic at Muhimbili National Hospital. Introduction Vascular lesions are among the most common congenital and neonatal abnmalities1. Mulliken and Glowacki2 classify vascular lesions into haemangiomas and vascular malformations. Vascular malformations occur as the results of aberrant vessels angiogenesis during embryogenesis (i.e. arterial, venous, capillary, lymphatic or mixed)3. They are classified clinically by their blood flow characteristics and can be described as “high flow” or “low flow” lesions4,5. Low flow lesions are more prevalent and consist of capillary, venous, lymphatic and venous-lymphatic varieties4,6 .Venous malformations are usually present at birth and grow proportionately with patient7. Lymphatic malformation is the most common lesion in the head and neck area8. They can be localized or may be associated with generalized abnormality of the lymphatic system. Usually enlarge slowly over time, but abrupt enlargement may occur in about 0.3% newborns and typically located in the head and neck region7. Venous malformations represent more than 50% of patients referred to centre for vascular anomalies7. Unlike haemangiomas, the histology of vascular malformation is composed of cells with normal endothelial and mast cell activity. Haemangioma is very common vascular lesion of infancy that usually appears 2-4 weeks after birth, grows rapidly until the age of 6-8 months and then slowly and predictably involutes by the age of 5-8 years8,9. On a cellular level, hamangiomas are characterized by increased endothelial turnover and increased numbers of mast cells during their rapid post natal growth phase10. Involuted haemangiomas have diminished cellularity with fibrous tissues, and have low mast cell counts10. Haemangiomas occur in about 10-12% of 1 year old children7,8. They are common in Caucasians and occur more frequently in females than males, in ration of 3:18. Usually 80% of all haemangiomas are single lesions, but 20%of the affected infants develop multiple lesions11. There is a wide range of therapies used in different units and different specialties indicating that there is no true consensus regarding the best treatment for each type of vascular anomalies especially for those that are extensive and involve several anatomical areas12. Haemangiomas because of their tendency to involute spontaneously are generally managed conservatively using wait and see attitude unless they bleed, ulcerate or interfere with functions8,13. In infants and children, such threatening haemangioma and vascular malformations of orofacial areas have been treated by surgical excision with blade or laser, cryosurgery, steroid therapy or radiotherapy9. Many studies on craniofacial vascular lesions have been conducted worldwide but none in our country and especially at our centre. The present study aimed at the documentation of clinico-demographic pattern of craniofacial vascular lesions seen among patients attending oral and maxillofacial unit at Muhimbili National Hospital. Patients and Methods This was a prospective study involving patients with histological/cytological diagnosis of vascular lesions of orofacial region seen within the period of 3 years (February 2008 to Jan 2011) at the Maxillofacial Centre Muhimbili National Hospital, Tanzania. Clinico-demographic data (age, sex, diagnosis, location, clinical behavior and treatment information) of the patients were documented, entered into the computer and analyzed using SPSS programme version 13 and presented in the form of tables. Results The study consisted of 33 patients of whom 16 were males and 17 were females. The sex ratio (M: F) was 1:1.1 and the mean age was 9.36 years. The age ranged from I month to 56 years. The age group 0-9 years was the most affected 19(57.6%). Age groups 20-29 and 50-59 were least affected. Haemangioma was the commonest vascular lesion found 19 (57.6%) followed by lymphangioma 12 (36.4%). Cystic hygroma and syndromic vascular lesions were found less frequently. Females were slightly more affected with haemangioma (M: F 1:1.4) compared to male while lymphangioma affected both sexes equally (M: F 1:1) [Table 1 and 2]. Clinically the lesions presented as painless swellings with no colour change of the skin and mucosa for lymphangiomas and cystic hygroma and with colour change for haemangioma and syndromic vascular lesions. Most of haemangiomas 14 (73.7%) presented after birth while most of lymphangiomas 9 (75%) presented at birth. Cystic hygroma and syndromic vascular lesions presented at birth (Table 3). Cheek and upper lip was the commonest site affected disregarding of type of lesions in 11 (33.3%) and 10 (30.3%) respectively. The commonest location for haemangiomas were the cheek 7(21.2), upper lip 5(15.2%). The lower lip 3(9.1%), tongue 1(3%) and floor of the mouth were less affected. Lymphangiomas were commonly located on the upper lip 5(15.2%) followed by the cheek 4(12.1 %), tongue 2(6.1%) and the lower lip 1(3%) (Table 2). Of the total patients attended at our centre, only 5 patients received active treatment of whom 4 patients had haemangioma and 1 patient had lymphangioma. Mode of treatment was surgery preceded by injections of sclerosing agent (alcohol 70%). Eight patients had very extensive lesions and were referred to specialized centre for vascular lesions abroad. The remaining 20 (60%) were still being followed up at our clinic including those who had been operated. Discussion Birthmarks sometimes represent significant vascular anomalies that require diagnosis and treatment. Knowing the vascular anomalies underlying the birthmarks helps to avoid missed or incorrect diagnosis or extensive, unnecessary workup. Milliken and Glowack2 classify vascular lesions into haemangioma and vascular malformations. Separation of vascular lesions into one of these two groups can be of considerable significance relative to the treatment of patients. Unfortunately, in actual practice, some difficulties may be encountered in classifying lesion in this way because of overlapping clinical and histologic features 14,15. The current study showed haemangioma was the commonest group of vascular lesion of head and neck and followed by lymphatic malformations. This is in contrary to what others have reported in the literature that the head and neck is the most common site of lymphatic malformations8,16. The probable reasons for this difference are that clinically the lymphangioma may occasionally appear similar to haemangioma when it has a significant capillary component. Also many atrio-venous malformations (AVM) are misdiagnosed as haemangiomas during infancy only to later cause progressive soft tissue destruction, ulceration, bleeding and disfigurement17. The finding of the present study that most haemangiomas presented after birth while vascular malformations presented at birth concurred with other studies in the world literature 18. However, vascular malformations may not be seen at birth. These lesions may not be evident until additional growth or vascular engorgement is seen as response of thrombosis, trauma, infection or endocrine fluctuation19. As a result these lesions are commonly misdiagnosed as haemangioma. Such misdiagnoses in patients with vascular anomalies often receive inadequate treatment. Depending upon the anomaly, such inappropriate management can risk potential long-term functional and cosmetic sequelae. Previous reports indicated that haemangiomas occur more frequently in females than males (M: F = 1:3) while vascular malformations occur equally in both sexes (M:F-1:1)8. This was confirmed in the current study. Also the study showed that Haemangioma and lymphatic malformations were nearly equally distributed in the oral and maxillofacial region with the upper lip and check being the most preferred sites. Jochen et al8 stated that the head and neck area is the most common site of lymphatic malformations and also 75% of all lymphatic malformations (LMS) occur in the head and neck region16. It seems therefore, the pattern of occurrences of vascular lesions in this population is different from what has been reported in the literature since the present study reported haemangioma as the commonest malformation in this region. The probable reason for this difference is that the settings for these studies were different. Some were done in an institution which deals with vascular anomalies only while others like the present one was done in an institution which deals with oral & maxillofacial surgery. Also there could be geographical variation in the pattern of occurrence of vascular lesions in different part of the world. Furthermore, as many arteriovenous malformations are mis-diagnosed as haemangioma there could be misdiagnosis between vascular malformations and haemangioma14. Whether haemangoma or malformation, these vascular lesions represent the most common growth of infancy and child hood (57.6% of child & infancy affected in the age group 0-9 in the current study) in the head and neck region, and may vary from a small innocuous mark to a disfiguring process22. Separation of vascular lesions into haemangioma and vascular malformations can be of considerable significance relative to treatment. Unfortunately, in actual practice, some difficulties may be encountered in classifying lesions in this way because of overlapping clinical and histological features. In any event haemangiomas has been subdivided into two microscopic types (capillary and cavernous) that essentially reflect differences in vessel diameter. Vascular malformations may exhibit similar features but show vascular channels that represent arteries and veins. Lymphatic malformations are one type of vascular malformations. The head and neck surgeon play a central role in the management of these patients. These lesions occasionally affect vital functions and frequently cause disfigurement (Figures 1, 2, 3a, 3b, 4a, 4b, 4c and 5a, 5b). The principal goal of lymphatic management is restoration or preservation of function and aesthetic integrity. Standard LM treatment is ablative and variably successful, necessitating multiple treatments and long-term management14,15,16. All treatments are based on thorough initial assessment to detect the degree of functional impairment and/or disfigurement. Severe life-threatening functional impairment necessitates early treatment. When there is significant functional deficit, treatment can be delayed well past infancy and may consist of surgery, sclerotherapy, or observation. In the oral and maxillofacial regions, diagnosis of vascular malformation may be easy, but their management remains difficult. Previous reports indicate that the likelihood of cure may be improved in lesions treated at an earlier stage of development22. Early diagnosis is best established with MRI, arteriogram, and CT-angiography illustrating high flow lesions with flow voids and supplemental vasculature. Surgical resection, endovascular embolization or combination of these modalities has been attempted in the management of AVM23. Some evidence suggests that surgery with preoperative embolization and complete removal of the nidus offers the best chance for cure25. Generally, treatment of vascular lesions continues to centre on a careful surgical approach. Adjuncts include selective embolization and sclerosant therapy, Laser therapy is now a valid form of primary treatment of selected vascular lesions. The range of therapies in different units and by different specialties indicates that there is no true consensus regarding the best treatment for each type of vascular anomaly, especially those that are extensive and involve several anatomic areas. In the current study only few cases received treatment at our centre. Majority were referred abroad especially those with huge and devastating lesions. Our centre is still elementary in terms of management of vascular lesions as it lacks experts and equipments. The management of these lesions is complex and requires an intergraded team approach including surgeons, interventional radiologists, and critical care intensivists. Therefore, referral to the treatment centers familiar with the endovascular or surgical management of these lesions is strongly advocated. Although many of these lesions were referred outside of the country for treatment, the success of some of those malformations treated were discouraging and especially the lymphatic malformations (Figures. 3a and 3b).Some of those treatment offered did not restore function and aesthetics(Figures 3a and 3b).Therefore, careful choice of referral vascular center is very important before referring the patient. As the cost of referring & treating these lesion cost the country a lot of money which may otherwise injected into health care services, efforts should be put forward to train our own experts and to establish our own vascular centre for treating these lesions. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11057f4c.jpg] [js11057f3b.jpg] [js11057t2.jpg] [js11057f4b.jpg] [js11057f5a.jpg] [js11057f2.jpg] [js11057f1.jpg] [js11057f3a.jpg] [js11057t3.jpg] [js11057f4a.jpg] [js11057f5b.jpg] [js11057t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}