|
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 3, Nov/Dec, 2011, pp. 102-114 Prostate Cancer: Evidence Based Management Guidelines for Uganda J.B. Kigula Mugambe1, S. Watya2, S. Kaggwa2, I. Luutu1, D.M. Kanyike1, A. Luwaga1, J. Fualal2, J. Jombwe2, M.Galukande2, Leng3, A. Gakwaya2 1Radiotherapy Department, Mulago Hospital, Makerere
University College of Health Sciences Code Number: js11058 Introduction Cancer of the prostate is now the commonest malignancy in the male in Uganda1 while Kaposi’s sarcoma was the commonest in the 1990’s2. The incidence rate is 39.2:100,000 males in Kyaddondo County and it has been rising in Uganda since 19603. It is a challenging tumour to treat with most of the patients presenting with metastatic disease. Members of the Uganda cancer working group (Appendix I) compiled the currently accepted, most appropriate approach to the management of prostate cancer which was deemed available and accessible. All recommendations were category 2 A unless otherwise stated (Appendix II). Epidemiology The incidence rises with age e.g. at 40 years it is 1: 10,000 while at 40-59 years it is 1:103 and by 60-79 years it is 1:8. The median age at presentation is 72 years (comparable to the median age in African Americans)2. There is an increased incidence of cancer of the prostate in blacks. It has been noted that the genetically related prostatic cancer starts at an earlier age e.g. at 40 years and tends to be more aggressive4. Aetiology The aetiology of prostatic cancer is not known but the following are the risk factors. Risk Factors
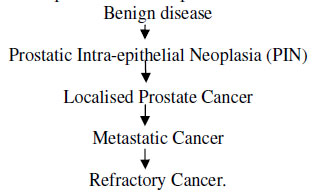
Pathology A genetic model has been proposed to explain the clinical presentation from:
Latent disease (PIN): Here malignant cells are shown histo-pathologically in the epithelial lining but without invasion of the basement membrane. Microscopic lesions have been found in 20% of men in the fifth decade, increasing to 60 % in the eighth decade12. The main histological type is an Adenocarcinoma (95%) – of which 85% are multifocal. The rest are due to small cell carcinomas, transitional cell carcinomas , lymphomas, neuro-endocrine and sarcomas. The spread is by local extension to the base of the bladder, seminal vesicles and lower ureters, by lymphatics to the regional LNs and by haematogenous spread via pelvic veins to the lower spine, other bones, lungs, brain and liver12. The UICC TNM Staging, group staging and Grading of Cancer of the Prostate are used13. Early Detection Any man who is over 40 years with a positive family history (Especially one with HPC-1 gene) warrants a high index of suspicion and should have annual screening PSA tests, digital rectal examination (DRE) and a Trans-rectal ultrasound scanning. At 50 years all men should have annual screening against prostatic cancer14,15. Clinical Presentation Early Disease Early prostatic cancer is usually asymptomatic and is diagnosed on screening PSA tests or on investigations of an accompanying benign prostatic hyperplasia. Men over 50 years should have regular screening tests as above. Those with a positive familial history should start as early as 40 years11,14,15. Late Disease The symptoms and signs of prostate cancer include urinary obstruction, haematuria (rare) haemospermia, and perineal pain and pain from osseous metastatic deposits. Other features may arise as a result of complications of the disease e.g. ureteric involvement/obstruction with uremia, spinal cord compression, anemia, cachexia, weight loss and others11. Diagnosis Digital Rectal Examination (DRE): The findings of a hard irregular gland on DRE suggests a diagnosis of prostate cancer. It has a 21-50% positive predictive value and only 40% of patients diagnosed by DRE will have local prostatic disease. It is a subjective examination with 60% of patients being under or over diagnosed if used in isolation. The diagnosis of malignancy on DRE depends upon its size, location and consistency as well as the skill of the examiner11. It should be combined with PSA determination and TRUS whenever possible. DRE should be done after the blood for PSA determination has been taken off. Investigations Prostatic Specific Antigen (PSA): This is produced by epithelial cells and secreted into the lumen and is the most sensitive and specific tumour marker for prostatic cancer. PSA determination leads to detection of earlier, organ confined disease and provides a lead time of 5-10 years compared with DRE4,11,15,16. False elevations occur after urethral instrumentations, DRE, prostatic biopsy, urinary retention, prostatitis and acute prostatic infarction. PSA is prostate specific but not disease specific. Combination with DRE and Trans-rectal ultrasound improves the sensitivity and disease specificity11.BPH causes an average rise of PSA of 0.75ng/ml per year. A rise above this rate therefore calls for more evaluation. The risk of finding prostatic cancer on biopsy is related to the PSA level: About 5-25% for PSA <4, 15-25% for PSA 4-10, and up to 50-67% for PSA level > 1017. PSA is also useful in prognosis and follow-up of patients to assess response to treatment18. Ultrasound Scan (US)19,20,21 This can either be done Trans-abdominally (3.5-5 MHz probe) or transrectally ± biopsy (TRUS) or transperineally (7-9 MHz Probe). TRUS is superior to transabdominal US because it provides more anatomical details of the gland symmetry, the seminal vesicles and the zonal anatomy. The majority of lesions are hypoechoic. TRUS can detect non-palpable malignancies. It cannot however detect microscopic spread of malignancy. The Sensitivity of transrectal ultrasound (TRUS) varies from 52-91% and the Specificity for cancer is between 41-97%. Colour Doppler addition may help by demonstrating malignant vascularisation. Abdominal extension of the disease and hydronephrosis are shown by tans-abdominal scans. TRUS and Biopsy Needle core biopsy underestimates tumour grade in 33 - 45% of cases and it overestimates it in 4-32% of cases. Complications: Haematuria (20-25% of patient for 2 days), Infection (1-6%), haemospermia (9%), Haemoatochezia (blood in stool in 9%). At least 3-5 core biopsies should be taken from each lobe. Plain X-Rays Bone metastases are seen as osteoblastic lesions (commonest cause of such lesions). The X-rays are done as indicated by the patient’s complaint. Usually shown as osteoblastic lesions with or without pathological fractures. CXRs may also be done as indicated. CT Scan CT scan is useful in ascertaining the local spread especially where T3/T4 are suspected. It can also detect involved nodes which are larger than 1cm in diameter. The accuracy in identifying metastatic involvement of nodes is 40-50%21. MRI Scan Overall accuracy is 69% for staging prostate cancer (local and advanced). It is better than CT for detecting local extension, but has no advantage for lymph node metastases. A PET-CT Scan is preferable where available19,20. It is also more sensitive in detecting bone metastases than radioisotope bone scans which may have up to 11% false negatives11. Bone Scan This is required in all cases of advanced disease. It is also indicated for early cancers with PSA levels higher than 10ng/ml. 24% of all prostate cancer patients have bone metastases by the time of diagnosis, 11% are however false-negatives11. The indications include bone pain with any PSA value; PSA > 10ng/ml prior to any intervention and Gleason score of or greater than 8; PSA >2.0ng/ml after prostatectomy. 43% with positive bone scans are asymptomatic); T3/T4 tumours and Elevated alkaline phosphatase. PS: SPECT and PET-CT are more accurate than the traditional bone scans. Histo-Pathology This is required to confirm the diagnosis and for tumour grading, Gleason score and staging. Laboratory Tests PSA, Alkaline Phosphatase, Haemogram, and Kidney function tests are required. The risk of progression depends on the tumour grade, age, serum PSA levels and the clinical stage and these should be assessed at diagnosis and a “risk classification / stratification” done. Treatment of Prostatic Cancer The treatment of cancer of the prostate depends on risk stratification, age, life expectancy of the patient and patient preference. The options include surgery and radiotherapy (which may be curative or palliative), hormonal manipulation (androgen depletion therapy – ADT), or a combination of the above or just watchful waiting11,15,20. Fox Chase prognostic index for cancer of prostate17.
Key: PSA= prostate specific antigen, FF =Favorable features, UF= Unfavorable features, Pn= Perineural invasion, FF refers to: Stage T1/T2a, G/Score 2-6, Perineural invasion –ve, UF refers to: Stage T2b, or T3, Gleason score 7-10, Perineural invasion +ve, Prognostic Factors The most important predictors of disease in organ confined prostate cancer are:
Other factors which predict survival are peri-neural invasion and number of positive cores. There are several risk stratification schemes in use17. In these guidelines, we recommend the Fox Chase risk stratification system as we find it is user friendly. Management of Organ Confined Disease Surgery (i) Watchful Waiting This is applicable in patients who are 70 years or older, and life expectancies of less than 10 years. This is done in low risk patients and involves careful observation and PSA monitoring at regular intervals (every 3 months). Treatment is initiated when cancer causes symptoms or PSA values start to rise. The rationale is that only 10-25% of these cancers progress within 10 years, and they rarely advance significantly within 5 years11,22,23.If the patient is sexually active, watchful waiting should also be considered22,24,25,26. ii) Curative Surgery27,28,29,30 Radical prostatectomy is indicated in organ confined disease (T1, T2, N0,M0) in a patient with a life expectancy of greater than 10 years. The aim is to cure. There is however a 1% peri-operative mortality (going up to 4% depending on age), 30% erectile dysfunction, 2-18% incontinence, and in 14 - 41% there are positive surgical margins29. iii) Palliative Surgery This is indicated in metastatic disease which is often the stage at presentation30. The following may be done: a.
Bilateral Orchidectomy (surgical
castration): The lowest levels of testosterone (Nadir levels) are reached
within 9-10 hours. Radiotherapy Controversies in the management of prostate cancer make treatment selection one of the most challenging areas in contemporary oncology23,31,32,20. External beam radiotherapy (EBRT) is the one treatment modality that has applications at every stage in the natural history of prostate cancer. Low risk Patients: – organ confined11,15,17,25,27,31,33,35 For patients with life expectancy of more than 10 years, RT alone using either EBRT or with brachytherapy (BCT) gives similar results with radical surgery. A four field box technique using an 8x8 cm field size is employed to a total dose of 60-64 Gy in 30-32 fractions in 6-6.4 weeks17. Where possible, dose escalation using 3D-CRT or IMRT to 75-80 Gy may be done33. Adjuvant RT is also indicated for patients with positive margins and positive lymph nodes after prostatectomy. For a patient to be considered for BCT the prostatic volume should not exceed 50 cm3 with no urinary obstruction, no previous TURP and no prostatitis. BCT can be given by permanent implants e.g. iodine 125 / Palladium 103 or high dose rate insertions using iridium 192 27,34. Intermediate Risk patients – Organ Confined11,15,17,25,27,31,33,35 For patients with life expectancy less than 10 years, definitive RT with short term hormonal therapy (HT) is advisable whenever possible or Expectant management as an option. For life expectancy of 10 years or more, whole pelvic RT + short term HT (4-6 months) is given. The options are high dose RT alone, or radical prostatectomy (RP) ± pelvic LN dissection. If prostatectomy was done and the margins are positive, adjuvant RT ± short term HT is given. If radical prostatectomy was done and the LNs were positive androgen ablation ± RT or expectant management can be done35,11. High Risk Patients11,15,17,25,27,31,33,35 Whole pelvic RT ± BCT boost where possible is done + long term AD ≥ 2 years. If the patient is node positive, Whole pelvic RT + long term AD ≥ 2 years can be considered or androgen ablation alone can be done. In metastatic disease, Androgen ablation ± palliative RT ± bisphosphonates are given. For hormone refractory disease docetaxel + prednisone is advisable. If a patient has residual disease or recurs after radical prostatectomy, RT ± AD (especially if there is high risk of metastases) or observation. If patient recurs after RT without high risk of metastases, then salvage RP or salvage brachytherapy is given. If the patient is metastatic or not candidate for local therapy then, androgen ablation or observation is done. 3D conformal treatment is the ideal modality as it allows safe escalation of the radiation dose with an improved disease control. Intensity modulated radiotherapy (IMRT) which is an advanced form of three-dimensional planning, holds promise to further improve dose distribution. Another area of intense investigation has been the use of interstitial radioactive implants, alone or in combination with EBRT. In locally advanced prostate cancer (tumor with extension beyond the confines of the glandular capsule, into the seminal vesicles, or into regional structures), EBRT combined with androgen deprivation has become the standard of care. For those patients who have undergone surgical resection as the primary form of management, retrospective studies have identified a role for adjuvant EBRT. It provides extra safety for tumors with poor pathologic features (e.g. positive margins, high grade, and advanced pathologic tumor stage). EBRT also has a role in salvage therapy for patients with late local recurrences following surgery (whether detected on biochemical studies or by physical examination). Finally, EBRT has a well-established role in the management of symptomatic osseous metastases, and it generally provides quick and effective pain control. Radiotherapy Treatment11,15,17,25,27,28,29,30,31,33,35 Brachytherapy (BCT) Inclusion criteria for BCT are: life expectancy greater than ten years, biopsy confirmed adenocarcinoma of prostate, disease confined within prostate capsule, bone scan negative, CT or MRI showing no pelvic or abdominal lymph node enlargement, no prior transurethral resection of the prostate (TURP) and PSA less than 20ng/ml and a prostatic volume of less than 50 ml. External Beam Radiation Therapy (EBRT) The target volume includes the tumor and any local extension e.g. seminal vesicles with safety margins of 1.0 cm. The field is 8 x 8 cm with the center of the volume 1 cm below the top of the pubic symphysis in the midline. A dose of 64 Gy in 32 fractions in 6.4 weeks is recommended. Conformal therapy can be given with dose escalation (where available). Post Operative RT is not routinely given because of the potential risks of complications from both surgery and radiotherapy. Palliative Radiotherapy Radiotherapy has a useful role in relieving pain from bone metastases. It can also shrink advanced local disease causing symptoms of urinary obstruction and pelvic nodes causing lymph oedema and nerve compression. The dose is : Prostate 30 Gy in 10 daily fractions over 2 weeks. Bone Metastases For the metastases confined to a limited area (e.g. lumbar spine) a single fraction of 8.0 Gy is preferred but 20 Gy in 4/5 daily fractions or 30 Gy in 10 fractions may be given. The single fractions offers similar palliation of bone pain compared with the more fractionated treatments28,29. For wide spread bone metastases, hemi-body irradiation is utilized depending on the site. The patient is given intravenous fluids and steroids, and fasted before treatment. If both halves of the body are treated, an interval of at least 6 weeks is allowed before the other half is treated. The dose for lower half of the body is 8 Gy mid-plane in a single fraction. For the upper half, it is 6 Gy mid-plane in a single fraction. Regular anti-emetics are given before and after treatment11. Breast Prophylaxis To prevent gynecomastia which is a common side effect of hormonal therapy, prophylactic breast irradiation is given. 10Gy is delivered as a single dose to each entire breast through tangential fields. This must be done before hormonal treatment because once glandular hyperplasia is initiated the process is irreversible. Complications The complications of EBRT include: Erectile dysfunction (48-59%): patients who have had previous TURP or pelvic surgery are at greater risk of developing severe complications; Cystitis (8%); Urethral strictures (4%); Enteritis (3%); Proctitis (2%) and Risk of second malignancy11,17,27,28. The complications of BCT include: Urinary voiding symptoms (incontinence) (12%), erectile dysfunction (10%), rectal discomfort (3%) and oedema (3%). Management of Radiotherapy complications Acute Cystitis can be managed by anticholinergics. e.g. probantheline bromide and oxybutynin. Citrosoda (bicarbonate) reduces cystitis by changing pH to alkaline. Proctitis is managed by local steroids administration, antispasmodics e.g. atropine 0.6-1.2mg at night, or probantheline 15 mg 8 hourly. NSAIDs, oral codeine phosphate or morphine help in reducing associated pains. Late reactions Chronic cystitis, urethral strictures or incontinence and loss of sexual potency are difficult to treat. Bowel complications include rectal ulceration or stricture and small bowel obstruction. The symptoms are tenesmus, rectal bleeding and incontinence. Proctitis may respond to local steroid administration. A rectal pack of gauze soaked in formalin can be used if rectal bleeding persists. Side effects of hemi body irradiation include nausea, vomiting, hair loss, altered taste, pneumonitis and pancytopenia. These can be minimized by pre-medication using steroids, anti-emetics and iv rehydration. Antibiotics should only be given when there is an established bacterial infection11,17. Metastatic Prostate Cancer (MPC) Hormonal Manipulation11,15,17,27,28,30,38,2 By definition, MPC is incurable. MPC includes metastases to non-regional lymph nodes, bones and other distant sites like lungs and liver. In Uganda, almost 100% of our patients present with MPC while it is only 60% in UK and between 20-40% in USA and Canada. Presentation with MPC is decreasing rapidly in these countries with the increasing use of screening PSA. MPC usually responds to hormonal treatment aimed at androgen deprivation therapy (ADT). 80% of patients with MPC will respond to hormonal manipulation. This maybe by surgical orchidectomy or medical AD (includes LHRH agonist’s therapy, oestrogens and other anti-androgens therapy). i) Bilateral Orchidectomy: Achieves reduced testosterone levels within 9 hours of the operation. There was no agreement on the timing of orchidectomy - whether it should be taken as a first line option in resource limited setting and whether the findings of a hard, irregular prostate on DRE, raised PSA and radiological findings suggestive of metastatic bone metastases would be enough for a decision of orchidectomy in a centre where prostate biopsy cannot be done. These were therefore category 3 recommendations (see appendix 2. ii) Diethylstilboestrol (stilboesterol): This should be used with caution because of its potential side-effects of fluid retention, venous & arterial thrombosis, cardiac toxicity, stroke. It is however cheap and effective and is recommended for those patients who cannot afford the LHRH agonists. The dose is 1-3 mg daily24,31. In emergencies (e.g. impending spinal cord compression) high dose stilboesterol can be given tapering down over one week till a maintenance dose of 1 - 2.5 gm daily is reached24,31. This was a category 2B recommendation (see appendix 2).
This “Tumour flare” may worsen features of spinal cord compression, urinary obstruction or increased bone pain. Orchidectomy or concomitant use of an anti-androgen e.g. Bicalutamide (casodex) or flutamide is advisable. It should be started 3 days before the gonadorelin analogue and it should be continued for 3 weeks. Low levels of 0.2-0.5µmol/l (nadir) are reached in 3 weeks.
The side effects include urticaria at site of injection, hot flushes, hypertension, hypotension, gynecomastia and erectile dysfunction etc. Possble Combinations in Medical Hormonal Manipulation11,15,17,28,29,31,38 A. Monotherapy with antiandrogens: can use
B. Early androgen deprivation therapy Early therapy offers a survival advantage over delayed treatment, especially when the tumour burden is minimal. Early treatment may also delay complications of late prostate cancer23. C. Intermitent androgen suppression (IAS): Involves initiation of anti- androgen therapy and then halting therapy upon a predefined clinical response (usually based on PSA level). It aims to delay progression but does not prevent androgen-independent state. Maximum androgen blockade (MAB) is given for 6 months until PSA nadir is reached. Consider IAS if PSA level is stable at <4ng/ml. Therapy is then withdrawn until PSA reaches pre-treatment levels and then restart. Patients are off therapy for mean of 41% - 45% of the time. The mean time to progression is 128 weeks. Mean overall survival is 52 months D. Maximum androgen blockade (MAB): The rationale is that 20-25% of patients who relapse after orchidectomy are found to have high levels of serum DHY. MAB involves use of orchidectomy or LHRH agonist with an anti-androgen to block peripheral androgen action. It is not clear that combined therapy offers improved overall survival and the survival benefit must be weighed against the additional cost and inconvenience. There is no compelling evidence that this method of castration offers any advantage over the other medical/surgical methods12. Five-year actuarial rates comparing radiation with and without Luteinising Hormone Releasing (LHRH) agonists.
Hormonal Refractory Cancer The majority of patients who develop hormonal refractory cancers die within 12 months and HRC remains a major dilemma40,32,20,11. The options are: i. Withdraw anti- androgen therapy. 21% have serum PSA response, mean duration of response is 5 months. ii. Corticosteroids: a 50% decrease in PSA levels has been seen in 20% of patients. Anti-oestrogen therapy has been tied but with a poor response to tamoxifen (0-10%). There is however a 43% overall response to diethylstilboestrol (2nd line). iii. Bisphosphonates: Bone metastases occur in 80% of prostate cancers worldwide and in almost 100% of prostate cancer patients in Uganda. Long term use of androgen blockade also results in osteoporosis. Bisphosphonates have been shown to decrease the level of pain experienced and reduce the risk of skeletal events (e.g. pathologic fractures, hypercalcemia and the need for radiotherapy or surgery). The drugs include zoledronic acid (zometa) given at a dose of 4mg iv, alendronate (70 mg p.o. weekly), etidronate (didronel) and pamidronate (aredia). Supplement of vitamin D and calcium may be required in patients with renal insufficiency to prevent hypocalcemia41. iv. Chemotherapy: A wide range of chemotherapeutic agents have been shown to be effective in prostate cancer including Docetaxel and Prednisolone, Etoposide, (Nitrogen Mustard) Estromustine and Mitoxantrone. 3 weekly docetaxel with prednisolone has been shown to lead to improved survival in “castration-recurrent prostate cancer” and chemotherapy should be reserved for such men. The other combinations should only be used in clinical trial settings. Future direction is towards developing angiogenesis inhibitors, growth factor inhibitors and immunotherapy.42,43,44,20 Adrenal Androgen Inhibitors: 3rd Line options40,41,42,43,44,20 Ketaconazole: The dose ranges from 200 – 400mg three times daily. It should be given with caution and regular liver function tests are required as it is hepatotoxicity. Aminoglutethimide: Blockade is at suprarenal level. The start dose is 250 mg tds for three weeks and it is then stepped up to 250 mg qid. It should be given in combination with hydrocortisone 30 mg daily (20 mg in the morning and 10 mg in the evening). Low dose steroids: These inhibit ACTH (adrenal cortical tropic hormone) secretion through a negative feedback loop. Dose of Hydrocortisone as when given with aminoglutethimide. Megesterol acetate: Given at a dose of 40 mg qid. Complications of Late Prostate 11,17,20,27,28,30 Spinal Cord Compression - This mostly occurs in the thoracic and lumbar regions of the spine. It is managed with irradiation or surgery and or hormonal manipulation. Bladder Obstruction - Occurs in up to two thirds of patients on androgen deprivation therapy. It is treated with insertion of an indwelling catheter or intermittent catheterization for up to 3 months. The patient is re-evaluated for a possible TURP and palliative EBRT. Anaemia - The cause of this is multifactorial. The patient may benefit from iron, folic acid, vitamin supplements and erythropoietin. Blood transfusion may improve strength and performance status. Palliative Care11,15,17,20,25,27,28 A multidisciplinary team approach is very important in the care of these patients and should be patient and family centered. Managing Physical signs and Symptoms Pain This is managed according to the WHO 3-step analgesic ladder (see appendix VII). Somatic Pain - Paracetamol and non-steroidal anti-inflammatory drugs (NSAIDs) may be needed for bone pain, which is very common in prostate cancer. If the pain is not controlled a weak opioid (like codeine) should be added. Strong opioids like morphine are required in severe pain. Luxatives should be added whenever the opioids are given. Severe Bone Pain - It is crucial to control for maintaining quality of life. Irradiation can provide relief in 80% of patients for up to 6 months. Bisphosphonates help by inhibiting the activity of osteoclasts (prostaglandins). Neuropathic Pain - Prostatic cancer may invade nerve tissues manifesting with neuropathic pain. Amitriptylline, anticonvulsants (like phenytoin and carbemazepine) or both may be beneficial in treating this complication. Hypercalcemia This is managed depending on the degree of severity. The management includes intravenous fluids, loop diuretics, bisphophonates and calcitonin. Social, Emotional and Spiritual Issues Family stress - It is important to support and discuss salient issues with the patient, wife, children and close family friends. Sexual Problems - It is important to discuss with the couple. This may make them understand what is happening and helps them decide what is better for them. Open and honest discussions for the patient and partner including alternatives to penetrative sexual intercourse should be availed. Spiritual Issues - Spiritual beliefs can be comforting when death is approaching; patients have questions about what is to happen. He may need to make peace with God so that his soul is safe after death. A spiritual advisor will play a role but it is important to respect people’s spiritual beliefs. Patients may need someone to talk to or pray with like religious leaders or someone else they respect. Prognosis20,28, 17,11,45 Important prognostic factors include T-stage, the degree of tumour differentiation and genetic factors i.e. Patients with T1 / T2a disease have a 53% survival rate at 15 years. Well differentiated T3 tumours have a 10 year survival rate of 50% while poorly differentiated tumours have a 10-year adjusted survival rate of less than 20%. The median survival for metastatic cancer is 3 years. There is a very large survival advantage of African American male compared with Ugandan men but the 5 year relative survival rate of Uganda men at 46.9% is comparable to the rates in other developing countries.2 Appendix I: List of Uganda Prostate Cancer Working Group. Dr
Gakwaya Antony Senior Consultant Surgeon (Chairman) Appendix: Categories of Evidence and Consensus of the UCWG Category 1: The recommendation is based on high level evidence (e.g. randomized
controlled trial) and there was UCWG consensus All recommendations are category 2 A unless otherwise stated. References
Copyright 2011 - East and Central African Journal of Surgery |
| |||||||||