 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Penile ectopic testis: experience of an adolescent P.A. Ongom, Department
of Surgery, School of Medicine, Makerere College of Health Sciences, Makerere
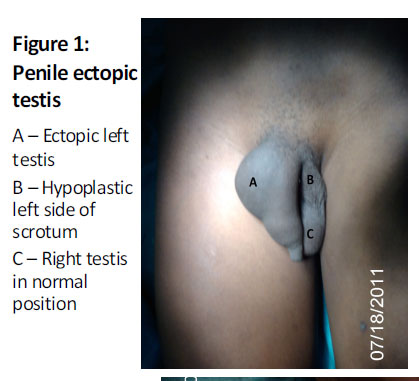
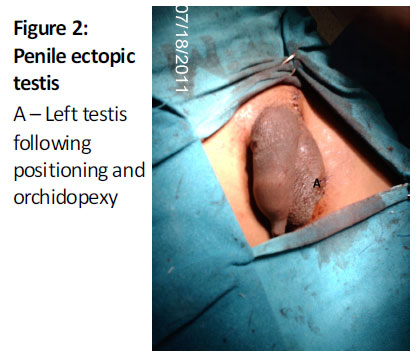
University Fax: +256-414-532591, Code Number: js11063 This report describes a case of a penile ectopic testis a 14 years old. The condition had been present since birth. Social reasons hampered earlier referral for appropriate medical care. There had been progressive penile development, in association with a swelling, and normal secondary sexual characteristics. The scrotum was well developed on the right side. The right testis and spermatic cord were normal in size and position. The left scrotum was empty. There was an ovoid mass (the left testis) at the right (contralateral), dorsal, proximal half of the penile shaft. It was normal in size with a palpable spermatic cord. An ultrasound scan confirmed these findings. Surgical exploration and mobilization of the ectopic testis was done through a left inguinal incision. A gubernaculum was present. Colle’s fascia of the left scrotum was dissected. A left scrotal incision was used to anchor (orchidopexy) the left testis in a sub-Dartos pouch. Postoperative recovery was normal. It was concluded that a penile ectopic testis, normal in size, may present during adolescence. The condition is correctible though there is need for screening and early detection in children through national Health Policy interventions. Introduction Testicular maldescent or crytorchidism is the most common anomaly of the genitalia with an incidence of approximately 1% in male newborns. It is commoner on the right side, and in premature neonates1,2. It is reported that 5 % of maldescended testes are ectopic3. Ectopic testis (Testicular ectopia) specifically describes inguinoscrotal descent outside the normal boundaries. The major sites of ectopic testes are the superficial inguinal pouch, femoral, suprapubic, penile, transverse (contralateral hemiscrotum), and perineal. Penile ectopic testis is a rare congenital anomaly in which the testis is abnormally situated along the penile shaft or around its root. These conditions present at birth or within the 1st two years of childhood2. Definitive treatment of this condition is thus usually done in childhood. In this case, the condition was present at birth but presented to hospital during adolescence. A similar case was reported in India, with the patient presenting at the age of 19 years4. Penile ectopic testis cases are well documented. Of relevance are cases described by Albin R et al in 1972 and Concodorra JA et al in 1976, and more recently several other authors5,6,7,8. The emphasis is generally the description of the presentation, evaluation, management and possible aetiological factors. Theories based on embryological development attempt to explain the occurrence of ectopic testes2. During intra-embryonic life, an intra-abdominal gubernaculum develops and terminates in the inguinal region. It guides the testis in transabdominal descent to this area. Later, an extra-abdominal gubernaculum part forms and grows from the inguinal region to the scrotal fundus, guiding the inguino-scrotal descent. Ectopic testes may arise out of failure of proper positioning of the extraabdominal gubernaculums or its failure to form9,10. If the testis deviates from its course through obstruction (obstructive theory), an ectopic also arises. Increased intrabdominal pressure is involved in testis descent up to the inguinal region. It is worth noting that other ectopic forms have been documented. Perineal ectopic testis is particularly well described9,10,11,12. Their aetiology is best described by a failure of proper positioning of the extraabdominal gubernaculums. Reported cases have presented in infancy and early childhood. Very rare forms of ectopic testis include a subumbilical location13 and an anterior abdominal wall location14. It was postulated that the subumbilical ectopic testis was due the failure of formation of the extraabdominal gubernaculums leaving the testis to wander. Case Report A 14 year old adolescent, presented with an abnormal swelling of the penis since birth. His mother reported that the child had a normal birth from a local Health Centre, following an uneventful pregnancy, for which she had attended antenatal care. On subsequent health visits to the health unit, she was advised to get the child to a hospital where he could be seen by a Doctor. His father declined any intervention, citing it as a new found “clan identification birthmark”. It is only when the child was the age of 13 that she was able to get the child to have a doctor’s opinion. One year later she presented to the national referral hospital. There was no history of trauma to the perineum and no pain or swelling of the inguinal region. He was in a good general condition with normal male features for his age. He had normally developing male secondary sexual characteristics. The perineo-inguinal examination revealed a swelling on the right side of the penis, proximal half, and dorsal (Figure 1). The rest of the penile shaft was normal and he still had a phimosis. It measured approximately 2.6 by 2.4 cm, was regular, smooth, soft and mobile. The right testis was normally positioned in the right scrotal pouch. The left scrotal pouch was empty, and was smaller in size than the right. Its lower-most point also hung higher than the right. The penile swelling had a spermatic cord felt disappearing into the left superficial inguinal ring, having crossed the midline. This gave an provisional diagnosis of a penile, ectopic left testis. An ultrasound scan of the perineo-inguinal region and abdomen was done. It revealed a maldescent of the left testis to the contralateral side, with a normal positioning of the right testis. Surgery was done through 2 incisions. The first was a left medial inguinal incision. Through it, the ectopic testis was mobilized easily with blunt dissection. A gubernaculum, found attached to Buck’s fascia, was divided. The second incision was a left, low scrotal incision. Through this was found a hypoplastic Colle’s fascial pouch, which was dissected. The testis and its appendages, all normal, were positioned in the left side of the scrotum, in a sub-Darto’s pouch and orchidepexy performed (Figure 2). There was no associated hernia. Circumcision was not done. Post-operative recovery was uneventful. He is currently being followed up for one year. This is to monitor complete healing and attainment of normal penile and scrotal srtucture. Histological report showed normal adult testicular tissue. Discussion This case describes a left penile ectopic testis, with contralateral (right) positioning. The patient presented in early adolescence. A similar case was reported in India, of a 19 year old male who had had the condition since birth4. The presenting features were similar to ours. He had a left penile ectopic testis, positioned to the right side. Cord structures were palpable on the left side and extended up to the proximal end of the swelling, which was on right pre-pubic area. The scrotum was well developed bilaterally, but was empty on the left side. The right testis and cord were normal. Secondary sexual characters were well developed. Routine investigations and the semen analysis were within normal limits. In the case under review, semen analysis was not done. Ultrasound scan is a highly effective radiological investigation. There was no relevance of computerized tomography, which however is useful for cryptorchidism with an intra-abdominal location of the testis15. The gubernacular tail theory provides a simple and valid explanation of the aetiology of the penile ectopic testis13. The presence of a gubernaculum attached to the penile fascia of Buck indicates an anomalous growth and termination of its extraabdominal portion. Though there have been quite a number of reported cases of penile ectopic testis, the uniqueness in this case is a presentation at adolescence, after the onset of puberty. This was mainly attributed to social factors. These included: a father who was against medical assessment and possible intervention from early childhood; and a poor socioeconomic setup, not giving a willing mother decision making powers. It took a separation between the boy’s parents for the mother to access some help from a sister in order to get the required medical attention. Other possible surgical intervention that he could have benefitted from during the operation, was circumcision. Maternal consent was not given for this, feeling that we had to overcome one hurdle at a time. In conclusion, we have a patient who presented with a left penile ectopic testis in adolescent life. The lesson to learn is that patients may present later than early childhood (over 5 years) and even up to adolescence and adulthood. The condition is correctible even at these later stages. Possible intervention by Health policy custodians, like the Ministry of Health, can be geared at notification of urogenital-inguinal anomalies at birth and at times of child health visits to health facilities. This can go hand in hand with anorectal malformation notification. Anorectal anomalies are reported early more frequently because of their intestinal obstructive effect. Testicular maldescent, occurring in every 1 in 100 births, deserves a place in the child health card. Social workers in communities can provide remedies to other social challenges as seen in this case. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11063f2.jpg] [js11063f1.jpg] |
| |||||||||

{kind=link}
{kind=link}