 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 1, No. 1, Oct, 2004, pp. 1-5 Health and Nutritional Status of Children in Western Kenya in Relation to Vitamin A Deficiency Esther C Nabakwe1, Duncan K. Ngare2 Dept. of Child Health & Paediatrics1,
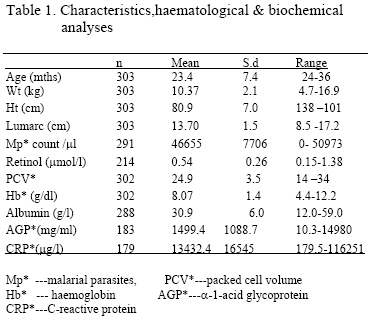
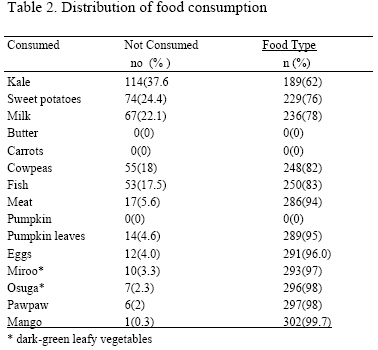
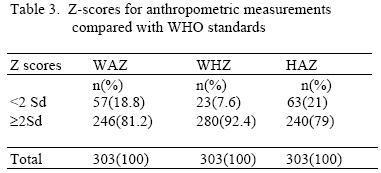
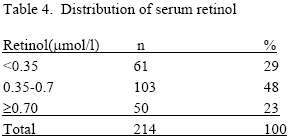
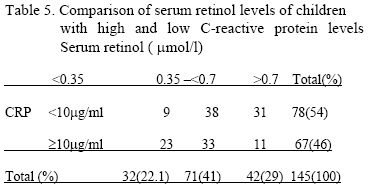
Behavioral Sciences2 Abstract A cross-sectional study was conducted from September to December 1998 among 300 children aged 1-3 years in Bungoma district of western Kenya. This is an area endemic for malaria with a high prevalence of vitamin A deficiency. In 1993 the prevalence of vitamin A deficiency was 37.8%. In the present study effects of vitamin A deficiency on health and growth of children were studied. Twenty-nine percent (29%) of the children had severe vitamin A deficiency 92% had anaemia, 76% had malaria parasitaemia and 21% were stunted. Anthropometric measures significantly correlated with haemoglobin concentration (P value <0.0001). There was significant difference in the retinol levels of the stunted and normal children (P value = 0.02). Retinol concentration differed significantly among children with high and low C-reactive protein (P = 0.0004). Vitamin A deficiency and anaemia are a public health problem among the children studied. High prevalence of vitamin A deficiency and anaemia was associated with impaired growth. Key words: Vitamin A, anaemia, malaria parasitaemia, acute phase proteins, young children Introduction Worldwide, malnutrition is one of the leading causes of childhood morbidity and mortality. In the developing countries, 15% or more of children born each year die before they reach 5 years of age. This is mainly due to malnutrition, parasitic infections and low birth weight. Malnutrition is aggravated further by diarrhea, infections (parasitic infections, measles, TB and pertusis). These infections whether acute or chronic, induce anorexia and divert nutrient energy from growth and development (1). Malaria has been shown to impair growth of younger but not older children (2). Mortality is high among these children and the survivors have stunted growth, impaired psychological and emotional development. Vitamin A deficiency is associated with poor immune function (3), increased risk of growth faltering, common childhood diseases and higher risk for childhood mortality (4). The importance of vitamin A to the health and visual acuity in children has been known since the 1920s (5). Children aged 1-3 years are affected more due to faster growth and higher physiological requirements of vitamin A (6). A study done in Papua New Guinea where children aged 6-60 months were supplemented with vitamin A showed that it had most effect on P.falciparum in the 12-36 month age group, in which morbidity rates are highest and immunity is actively developing. Lesser effects were seen in the 37-60 months age group in which some degree of protection might have already developed (7). Cross-sectional studies in young children and in adults have shown that low plasma retinol concentrations are associated with increased malarial parasite counts, which trigger an acute phase response that transiently depresses the circulating vitamin A levels (8). Alpha-1 acid glycoprotein (AGP) and C-reactive protein (CRP) rise during acute infection and then fall as the infection is controlled. The fall in AGP follows a slower time course similar to the fall in serum retinol after infection (9). The diagnosis of malnutrition is based on dietary history and anthropometric measurements (weight, height and mid arm circumference). Nutrient deficiencies may be revealed by measurement of the blood levels and consumption history. A survey was carried out in Sitikho sublocation of Webuye division in western Kenya to assess the health and nutritional status of children aged 1-3 years in relation to vitamin A deficiency. This was done by assay of serum retinol, examination of blood slides for malarial parasites, stool examination for ova and cysts, measurement of acute phase proteins (C-reactive protein and α -1 acid glycoprotein), documentation of history of illness and measurement of anthropometry. Study population and Methods The study was conducted in Sitikho sub-location of Webuye division in Bungoma district - western Kenya. This is an area endemic for malaria and in 1993 it was among areas where the prevalence of vitamin A deficiency was high – 37.8% (10). The highest registered rainfall is usually during the months of April to September- a time when malaria transmission is highest. Sugarcane is the main cash crop maize being the staple food. Animal sources of vitamin A and fruits are occasional in their diet. There is only one dispensary serving a population of about 10,000 people. The nearest sub-district hospital is 34 km away and bicycles are the only means of transport. Three hundred and three children aged 1-3 years were recruited in the study between the months of August and December 1998. Those with the following characteristics were excluded: - regular multivitamin supplementation or cod liver oil, sickle cell disease, and anti-malarial prophylaxis Moi University Research and Ethics Committee in collaboration with Maastricht University approved the study. Informed and written consent was sought from the mothers. Children with xerophthalmia, positive blood slides for malarial parasites, anemia and intestinal parasite infestation received appropriate standard treatment. WHO multistage cluster sampling technique was applied with the administrative division forming the sampling frame. Webuye division was randomly selected from a list of divisions in Bungoma district. From these divisions, Sitikho sublocation was randomly selected. The children were consecutively recruited from 8 villages where the households were visited daily from Monday to Friday by the investigator and a field assistant. Information on the child’s age was derived from the birthday. Growth monitoring cards and the mothers’ recall were used to determine the birthday and immunisation status. The mother’s age, level of education and occupation was recorded. The type and frequency of food eaten over the previous 24 hours was used to have an impression of dietary intake of vitamin A and protein-containing foods. History of illnesses such as malaria, measles, diarrhea, upper respiratory tract infections, otitis media and skin infections which occurred within a period of 2 weeks before survey were asked for and recorded. General examination of the children was done to detect anemia, xerophthalmia and splenomegaly. Axillary body temperature was measured using a clinical thermometer. Weight, height and mid-arm circumference were measured using a Salter scale, a height meter scale and a tape measure to the nearest 100g and 0.5cm respectively. Presence of edema was looked for and recorded. A sample of 3-5 mls venous blood was obtained from the children; 0.5-1 ml was placed in an EDTA-coated evacuated tubes (Becton Dickson, Cowley UK) and 3-4 mls was placed in a plain tube for hematological and biochemical studies respectively. These were transported to the laboratory at Webuye sub-district hospital in a cool box. Stool samples of the children were obtained for examination of ova and cysts. Those who were not able to produce a stool specimen were left with the polypots and asked to collect the stool within the following 24 hours. Laboratory Tests Samples in the plain tubes were immediately centrifuged at 1500-x g for 15 minutes at ambient temperature. Serum was separated and stored in tubes dried with liquid nitrogen. It was frozen at -20°C for one week and then transferred to a -80 °C refrigerator where they were stored until transported to Maastricht on dry ice where analysis was done. High performance liquid chromatography (HPLC) (11) was used to analyse serum retinol. Levels < 0.35 μmol/l were classified as severe vitamin A deficiency while levels between 0.35- <0.7μmol/l were marginally deficient. Serum alpha 1-acid acid glycoprotein (AGP) and C-reactive protein were measured to determine the degree of acute-phase response by ELISA technique. Values of AGP and CRP > 1 g/l and >10μg/ml were regarded as abnormal. Albumin was assayed by the Bromocresol green method (12). Serum albumin <35g/l was regarded as low. Haemoglobin was estimated using haemoglobincyanide method. Hemoglobin levels <6g/dl, 6-8g/dl and >8-10g/dl were classified as severe, moderate and mild anemia respectively. Thick blood smears were stained with Giemsa stain and examined for malarial parasites by a laboratory technologist. If after 200 leukocytes had been counted and 10 or more parasites were identified, these were recorded as parasites/200 leukocytes. If after 200 leukocytes had been counted, 9 or fewer parasites were identified, counting was continued until 500 leukocytes were counted. The number of parasites/500 leukocytes would be recorded. The number of malarial parasites per µl of blood was computed on the basis of total WBC count (13). Thus the number of parasites /200 WBC would be multiplied by 40 or 16 if 500 WBC were counted based on the fact that there are 8000 WBC / µl of blood. Malarial parasite counts of > 5000/ µ/l were regarded as high parasitaemia associated with clinical malaria. Direct examination and concentration techniques were used to examine the stool for ova and cysts (WHO 1991). Serum alpha 1-acid acid glycoprotein (AGP) and C-reactive protein were measured to determine the degree of acute-phase response by ELISA technique. Values of AGP and CRP > 1 g/l and >10μg/ml were regarded as abnormal. Data Analysis Data was entered into an IBM compatible microcomputer and analysed using the SPSS/PC + (Statistical Package for Social Sciences) package- 1989-1993. Cases with missing values were excluded from the various analyses. Weight for height (ZWH), (ZWA) and height for age (ZHA) were calculated according to WHO guidelines (14,15) thus: Normal ZWH 2SD ZHA > -2SD Underweight ZWA -2SD Those with left upper mid-arm circumference of: <12.5, >12.5 -13.5 and >13.5cm were regarded as malnourished, at risk of malnutrition and of normal nutritional status respectively. Correlation analysis was used to determine the relationship between vitamin A and anaemia with measures of anthropometry. Chi-square test was used to test the significance of the differences among children with and without vitamin A deficiency. Results Three hundred and three children aged 1-3 years were studied. One hundred and fifty (49.5%) were female while 153(50.5% ) were male.; most mothers 192(63%) had attained primary education; 277(91.4%)were unemployed. The characteristics, and biochemical analyses are shown in table 1. Nutrition The 24 -hour recall of the intake of vitamin A and protein-containing foods was as shown in table 2. None of the children consumed carrots, butter and pumpkins. All the 303 children had anthropometric measurements taken and compared with WHO standards using Z scores. Fifty-seven (18.8%) were underweight 23(8%) were wasted and 63(21%) were stunted. Forty one (14%) children were both stunted and underweight. Using the mid arm cicumference, 66(22%) were malnourished ( <12.5cm), 70(23%) were at risk of getting malnutrition (12.5-13.5cm) while 167(55%) were well nourished (>13.5cm). The distribution of nutritional status was as shown in table 3.. Two hundred and twenty seven (79%) children had serum albumin levels less than 35g/l while 61(21%) had normal albumin levels.Twenty-one (7%) had oedema. No significant difference was found in the retinol levels of the hypoalbuminimic and normal children (Chi-square p value = 0.55). Two hundred and eighty six children underwent ophthalmological examination. Conjunctival xerosis was detected in 168(59%), 5(2%) had Bitot’s spots while 113(39%) were normal (see table 4). Of the 214 samples on which biochemical analysis was done, 61(29%) had severe vitamin A deficiency deficiency (serum retinol <0.35mmol/l, 103(48%) had mirginal vitamin A deficiency while 50(23%) were normal (see table 4). Three hundred and three children were examined for clinical anaemia. Two hundred and thirty one(76%) were anaemic on clinical examination, 72(24%) were not anaemic. Haemoglobin estimation and packed cell volume was estimated on 301 samples. Two hundred and seventy six (92%) were anaemic; 25(8%)were not anaemic . The weight, height and left mid upper arm circumferance of the children significantly correlated with haemoglobin levels ( r values 0.3055,0.3033 and 0.3337 respectively with P values <0.0001). There was a statistically significant difference in the retinol levels of the stunted and normal children ( Chi-square Pvalue = 0.02). No significant difference was found between the retinol levels of wasted,undeweight and normal children (Chi-square P value = 0.47 and 0.93 rspectively). Health Status History of illness over the previous 2 weeks prior to recruitment into the study was reported among 267(88%) of the children. Thirty six (12%) were well. One hundred and thirty four (44%) had malaria, 58(19%) had dirrhoea, 56(19%) had upper respiratory tract infection, 12(4%) had skin diseases while 3(1%) had chronic otitis media. Thirty seven (12%) had unspecified illnesses. Information regarding the immunization status of one child was unavailable. Twelve(4%) had not been immunized, 64(21%) had incomplete immunizations while 226(75%) had completed their immunizations. Of the 301 blood slides which were examined for malarial parasites, two hundred and twenty nine (76%) were positive. Two hundred and ninety-one (291) had malaria parasitaemia quantified out of which 216 (74%) had malaria parasite counts less than 5000/μl of blood while 75 (26%) had counts ≥ 5000 /μl. The mere presence of malarial parasites was not correlated with temperatures equal or greater than 37.5oC (r = 0.0427, p = 0.46). One hundred and ninety (63%) had splenomegaly. E.histolytica was the commonest intestinal infestation accounting for 35(12%) of the cases. This was followed by A.lumbricoides 19(6%), hookworm 15(5%) and G.lamblia 11(4%) other intestinol parasites accounted for 22(8%) There was a negative correlation between worm infestation and serum retinol (r = -0.1514, p = 0.029); using Chi-square test ( p = 0.06), there was no significant difference in the retinol levels of children with and without worm infestation. Correlation with haemoglobin levels was not significant (r = 0.0691, p = 0.24). Acute Phase Response Ninety eight (55%) had serum C-reactive protein levels < 10μg/ml, while 81(45%) had raised serum levels >10μg/ml; 78(43%) had serum α-1-acid glycoprotein levels < 1g/l while 105(57%) had levels ≥ 1g/l (see table 9).There was significant negative correlation between serum retinol and C-reactive protein and α-1-acid glycoprotein ( r = -0.2642, p value = 0.001; r = -0.1780, p value = 0.03 and –0.1414 respectively. Using the Chi-square test, there was a high significant difference in the retinol levels of the children who had low and high serum C-reactive protein ( p value = 0.0004 see table 5). Discussion An association between low vitamin A status and impaired growth has been reported in several observational studies (16). In the present study 19% of the children were underweight 8% were wasted and 21% were stunted. There was a significant difference in the retinol levels of the stunted and normal children. These results are similar to the the findings of a National Survey done in 1993 which showed that the prevalence of stunting, wasting, and underweight among children aged 6 months to 6 years was 33%, 6% and 23% respectively. Stunting was highest among children aged 1-2 years (10). This implies that interventions to reduce malnutrition in the area have either not been effected or are unsuccessful. In Indonesia, biannual vitamin A supplementation significantly affected growth in males 3-6 years of age (17). In west Java, increasing the intake of vitamin A by fortification of monosodium glutamate significantly improved linear growth in preschool children (18). Improved physical growth following vitamin A supplementation could be due to a direct effect possibly involving stimulation of growth factors, or may result from a reduction in the incidence or severity of common infections (19). Most of the children - 88% had been ill 2 weeks prior to sampling. During infections, acute phase proteins ( C-reactive protein, α -1-acid glycoprotein (AGP) and serum amyloid A) rise. Serum amyloid A and C-reactive protein fall soon after infection while AGP follows a time course similar to the fall in levels of vitamin A during infection. It is thought that reduced hepatic release of retinol binding protein rather than preexisting nutritional deficiency is the major pathogenetic factor and that administration of vitamin A during initial treatment appears to be beneficial (9). In the present study, C-reactive protein and α -1-acid glycoprotein were significantly negatively correlated with serum retinol. There was a high significant difference in the retinol levels of the children who had low and high serum C-reactive protein. Twenty six percent (26%) of the children had counts ≥ 5001 /μl usually associated with clinical malaria (20).The correlation between intensity of malaria parasitaemia and C-reactive protein was significant.This implies that malaria parasitaemia induces an immediate acute phase response which has an indirect effect on serum retinol levels. During malaria infection,the material released when schizonts rapture induces activation of macrophages and release of mononuclear cell-derived cytokines including tumour necrosis factor and interleukin which cause fever and other pathological effects (21). Increased release of interleukin-6 causes a reduction in serum level of retinol binding protein and pre-albumin, thus impeding the transport of vitamin A from the liver to the target tissues (22). Low concentrations (< 0.35 μmol/l) of serum retinol are closely associated with clinical signs of vitamin A deficiency (23). To assess the public health significance of xerophthalmia and vitamin A deficiency, WHO has used several criteria. These are: - prevalence of night blindness (XN) ≥ 1.0%, Bitot’s sports (XIB) ≥ 0.5% corneal xerosis and or ulceration / keratomalasia ≥ 0.01%, xerophthalmia related corneal scars (XS) ≥ 0.05% with supportive serum retinol < 0.35 μmol/l (10 μg/dl) ≥5.0% (24). From this study a prevalence of Bitot’s spots of 2% with 29% of the children having serum retinol values less than 0.35 mmol/l indicate that vitamin A deficiency is a public health problem among these children. These results are similar to what Takyi found in Ghana – a malaria endemic area- the mean serum retinol of children aged 2-6 years was 16.8±1.7 μg/dl (0.58±0.24 μmol/l) – similar to a mean serum retinol of 0.54 ± 0.26 μmol/l in the present study. Seventy one percent (71%) compared to 76.6% of the children in the present study had vitamin A deficiency. No significant difference was found in the albumin levels of the vitamin A deficient and the normal children in Takyi’s and the present study (25). A survey done in the same district in 1993 showed that 37.8% of pre-school age children had vitamin A deficiency; 18% of those aged 1-3 years had serum retinol levels less than 0.35 μmol/l while 69.6% had marginal vitamin A deficiency (serum retinol 0.35 - 0.7 μmol/l) (10). The high prevalence of vitamin A deficiency could be partly explained by the low intake of vitamin A and protein-containing foods. None of the children in the present study consumed carrots, butter and pumpkins, which are known to be rich sources of vitamin A (see table 3). Helminth infestation may have contributed to the low serum retinol as there was significant correlation between worm infestation and serum retinol. Eighty-eight percent of the children studied had been unwell prior to enrollment into the study. Children aged 1-3 years are more prone to malaria infection among others. In this study, 76% of the children had malaria parasitaemia. In Kilifi district hospital at the Kenyan coast the incidence of malaria parasitaemia varied with age from 27-59% and was highest in the 3-year old age group (26). Febrile illnesses are associated with low serum retinol due to impaired transport from the storage sites. During infection an acute phase response is mounted with an increase in positive acute phase proteins (α -1 acid glycoprotein, C-reactive protein and serum amyloid A among others). This results into the binding of retinol to negative acute phase proteins – retinol binding protein and transthyretin. The serum concentrations of these proteins fall as endothelial permeability increases to allow an influx into extracellular space (27). The above is followed by increased utilization of vitamin A in tissues accompanied by losses in urine, in which case the reduction in serum retinol may reflect a reduction in liver reserves of vitamin A (28). Infections have been thought to cause reduced intake and absorption of vitamin A with increased tissue utilisation and increased renal loss (20) leading to low serum retinol. Ninety one point seven percent of the children studied were anaemic. This is similar to what Takyi found in Saboba in northern Ghana –a prevalence of anaemia of 92% with a high incidence of malaria of 32%. The cut off point for normal haemoglobin was12g/dl (25). Weight, height and left mid upper arm circumferance of the children significantly correlated with haemoglobin levels. Haemoglobin is essential for the transport of oxygen required for nutrient metabolism and hence growth. The high prevalence of anaemia may be partly due to malaria and vitamin A deficiency. In the 1930s studies in children showed that vitamin A deficiency results in anaemia and hemosiderosis in the liver and spleen (29). It was noted that the correction of vitamin A deficiency was followed by regeneration of bone marrow, disappearance of haemosiderin from the spleen and liver, and an outburst of erythroblast activity. This would suggest that vitamin A deficiency interferes with some step in the transfer of iron from storage in the liver to incorporation in haemoglobin and haematopoietic tissues. Vitamin A is required for the synthesis of transferrin. Marginal vitamin A deficiency has been shown to impair mobilisation of iron from stores (30). The statistically significant difference in the retinol levels of the stunted and normal children suggests that an impovement in the vitamin A status and subsequently the haemoglobin level may reduce the prevalence of malnutrition among these children. Conclusion Vitamin A deficiency, which could be a result of acute phase response during infection, is a public health problem among the children studied. This appears to have contributed to stunted growth as shown by significant difference in the retinol levels of the stunted and normal children. The high prevalence of anaemia among these children could also have contributed to impaired growth as the weight, height and left mid upper arm circumferance significantly correlated with haemoglobin levels . Acknowledgement My gratitude goes to the following for their essential participation:- NUFFIC for funding the project.The mothers for granting consent. The MOH and Matron of Webuye District Hospital for granting permission to use the hospital laboratory. Leonard Chelotti, Joan Senden,Frank Cox & Yohan for sample analysis. Prof. Burman for immunological tests and Dr. Rotich for data analysis. References
© Copyright 2004 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp04001t2.jpg] [lp04001t1.jpg] [lp04001t5.jpg] [lp04001t4.jpg] [lp04001t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}