 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 1, No. 1, Oct, 2004, pp. 6-10 Utilization of Health Care Services for STD Treatment in Kahe Community of Kilimanjaro Region in Tanzania. Felix S. Kisanga1, Kagoma S. Mnyika,2 Anna Tengia-Kessy1 Candida Moshiro2 Knut-Inge Klepp3 and Gunnar Kvåle4 1Department of Community Health,2Department of Epidemiology
& Biostatistics, MUCHS, 3Department of Nutrition Research,
University of Oslo Norway, 4Centre for International Health,
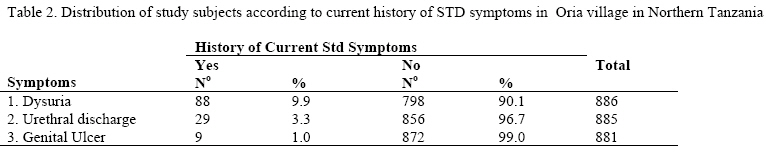
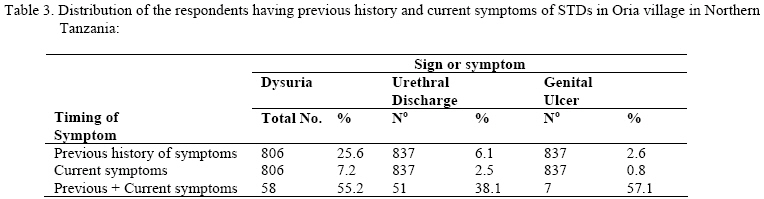
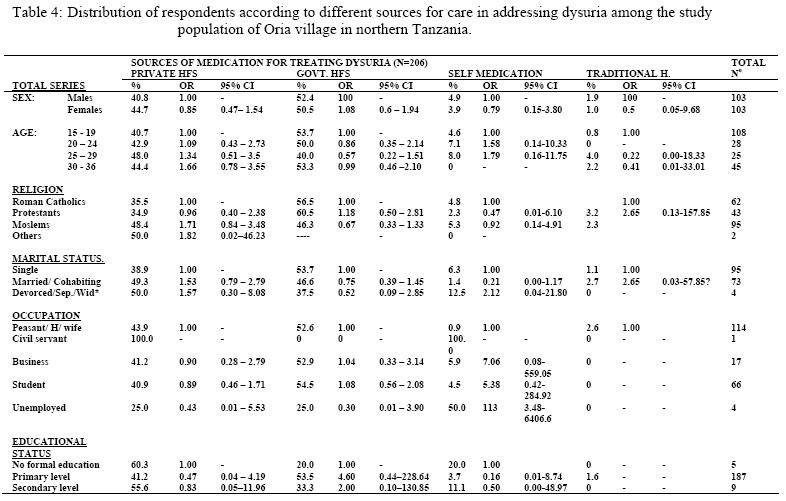
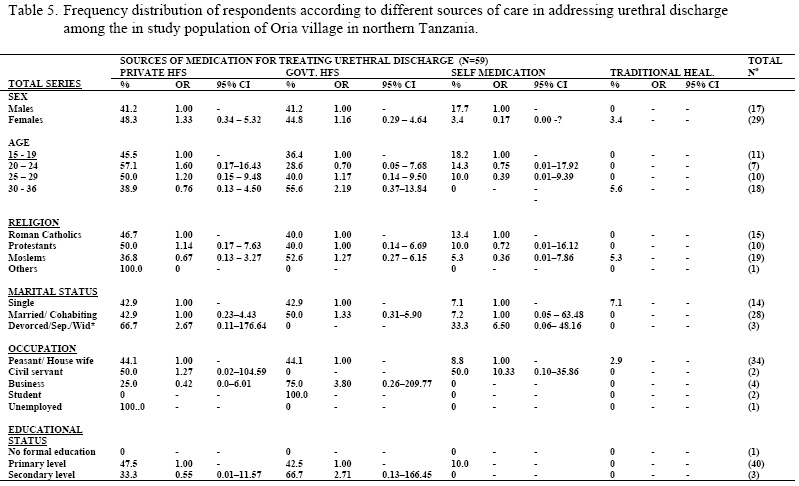
University of Bergen, Norway Code Number: lp04002 Abstract A population based survey set to find out the existence of Sexually Transmitted Diseases (STDs) and use of health care services among residents of Oria village in Kahe ward of Kilimanjaro region in northern Tanzania in 1997. A few of the STDs symptoms covered were history of painful micturation (dysuria), urethral discharge and genital ulcer(s). This was a cross-sectional study using quantitative data collection technique in which a total of 898 villagers were interviewed. Findings revealed that in the past 223 (25.4%) had dysuria, 69 (7.7%) had urethral discharge while 28 (3.1%) had genital ulcer. At the time of the interview, 88 (9.8%) people had dysuria, 29 (3.2%) had urethral discharge and 9 (1.0%) had genital ulcer. Health care was sought from different sources, mostly from modern health care especially government health facilities (HFs) followed by private HFs and less so to pharmacies and traditional healers. No significant differences were found between the proportions of respondents that pertained to the different demographic variables with regard to utilization of the different health services. However, it is doubtful as to whether people treat themselves adequately since among those currently having STDs symptoms, some had previous history of treatment for the same problems. This may be due to either inadequate treatment, re-infection from untreated partners or new infections. A real explanation ought to be explored through future studies. Meanwhile, there is need to re-direct the existing strategies in addressing STDs in Oria village. The increasing demand for STDs management requires an increase in the number of HFs both private and public that have skilled health workers, the necessary supplies and drugs. Special efforts be made to target high risk groups using different health education packages on STDs and reinforce contact tracing while alternative sources of health care need to be explored further. Introduction STDs occur both in developed and the developing world. However, they are more prevalent in the developing world where health services are inadequate in terms of number of health facilities, diagnostic laboratories, skilled health workers, drugs, supplies and the strategies to target the clients (1). In Tanzania, the demographic variables and movements of the population determine the pattern and distribution of the various STDs (2-3). They are more associated with urbanization and mobility pattern of the population. The large urban centers have the highest prevalence followed by small towns situated along the main trunk roads throughout the country and thus considered as high transmission areas. The most common STDs include Gonorrhoea, Syphillis, Chancroid, Herpes genitalis, Lymphogranuloma venereum, Trichomoniasis, HIV/AIDS and Chlamydia. The infected and asymptomatic individuals pose a big risk of transmission of the diseases to their sexual partners hence indicating the necessity of contact tracing and referral for treatment. Commercial sex workers, bar workers, street children, beggars and inter-country as well as intra-country petty business traders are among high-risk groups. The study area is also overwhelmed by different kinds of immigrants in search of petty businesses especially selling and buying fish, rice, maize, etc. The study was conducted in this area with an objective of finding out past experiences as well as during the time of interview, the occurrence of 3 STD symptoms namely dysuria, urethral discharge and genital ulcer. In treating the various STDs, enquiry about respondents’ preferences from among the available health care services was also done. Methods Study Area The study was conducted in Oria, one of the eleven villages that make Kahe ward. The other villages are Rau, Chekereni and Kahe. The ward is located 30 kilometres south of Moshi town within Moshi rural district of Kilimanjaro region in northern Tanzania. Kilimanjaro region is composed of six districts. These include Moshi rural, Mwanga, Rombo, Hai, Moshi urban and Same district. According to the 1988 population census, Kahe ward had a population of 16,400 composed of about 40 ethnic tribes but the main tribes are the Pare and Chagga. The main occupation is rice farming while a small proportion of the population is engaged in petty business. Subjects The study was a cross-sectional population-based. It was conducted in 1997 in Oria village that has about 4,000 residents. The inclusion criteria were; being a resident of the village and falling in age group 15-36 years since this is the group highly affected by HIV-1 infection in Tanzania. During this survey, all eligible subjects for the study were registered through house-to-house registration, and interviews took place in their households. The study was conducted after receiving ethical clearance from the Ministry of Health (MoH) in Tanzania and the Muhimbili University College of Health Sciences (MUCHS) in Dar es Salaam, Tanzania. The permission to carry out the study was sought from regional, down to village level of the study region through meetings held to inform the leaders on the purpose of the study. Data Collection Data was collected using a pre-tested structured interviewer-administered questionnaire that consisted of pre-coded and open-ended questions in the Swahili language. Information collected pertained to people’s past experience of STDs symptoms and any efforts undertaken in treating the diseases. The symptoms covered were; painful micturation (dysuria), urethral discharge and ulcer(s) on the genitalia or any other illness in which one was required to explain. Similarly during the time of the interview, participants were asked whether they still had any of the symptoms. In case of treatment, people were asked where they went to seek treatment during the last episode. The range of possibleoptions; private pharmacy or drug store, doctor/ private HF, government HF, traditional healer or used standby drugs. Research assistants to carry out fieldwork were recruited from Mawenzi hospital and the Kilimanjaro Chistian Medical Centre (KCMC) in Moshi, Tanzania. Before commencement of data collection, the assistants were trained on all aspects of the study including questionnaire administration. Preceded by each interview was a verbal informed consent for participation in the study of the respective clients. Confidentiality was maintained by having each of the research assistants administering the questionnaire to each consenting participant in a room/ place where nobody else could access the interview conversation. Two consecutive follow-up visits were made to try and meet all eligible participants who were absent/ missed following each household visit after which they were registered as non-responders. At the end of the interviews participants were given chance to ask questions and any misconceptions regarding HIV and other STDs, and these were cleared by the interviewer. Condoms and posters regarding HIV and some other STDs were distributed. Anyone found suffering from any minor ailment was offered treatment on the spot by the field team otherwise some were referred to either Mawenzi Regional hospital or Kilimanjaro Christian Medical Centre (KCMC) using project transport facilities. The response rates were 76% for females and 80% formen in this study. Statistical Data Analysis All questionnaire forms were checked for missing and out of range data as well as for illogical and inconsistent data. Checking for completeness and other errors was done at the end of each data collection day. The open-ended questions were coded before data entry. All the data were entered into a computer using the Statistical Package for Social Sciences (SPSS) for Windows Version 10.0. Statistical analyses were also performed using the same. Odds ration (OR) were calculated and statistical significance was assessed using 95% confidence intervals for the odds ratios (OR) and presented in the results. Results Eight hundred ninety eight (898) randomly selected respondents aged 15 – 36 years including 27.3% males and 72.7% females were interviewed. Questionnaire with incomplete information for some of the symptoms were excluded from the analysis. Two hundred twenty three 223 (25.4 % n=878) respondents gave history of dysuria. Among them, 113 (50.7%) sought health care from government HFs whereas 94 (42.2%) had gone to private HFs. While 13 (5.8%) respondents consulted drug pharmacies, 3 (12%) went to traditional healers. None used standby drugs. Urethral discharge was experienced by 69 (7.7%) respondents. The source of health care for the highest proportion (43.5%) was government HFs. Almost the same proportion (42.0%) went to private HFs. Pharmacy and traditional healers were contacted for care by 10.1% and 1.4 % of respondents respectively. Genital ulcer was experienced by 28 (3.1%) respondents where government HFs offered services to 35.7% of them and the rest went to private HFs (28.6%) and pharmacies (25.1%) (table 1). Current illness was elicited for “dysuria”, “urethral discharge” and “genital ulcer” from 88 (9.9% n=886), 29 (3.3% n=885) and 9 (1.0% n= 881) respondents for the three symptoms respectively (table 2). Their health seeking behaviour was not assessed. However, in the analysis the proportion of respondents who had STDs symptoms during the time of interview and a positive previous history of the same was found out. Out of 206 (25% n=806) respondents who had a previous history of dysuria, 32 (15.5%) had the same during the time of the interview. This is same as 55.2 % (n=58) of the subjects currently having such symptoms. Similarly, of the 51 (6.1% n=837) subjects who admitted to have history of urethral discharge, 8 (15.7%) had the symptom currently. This is same as 38.1% (n=21) who currently have the symptom. Genital ulcer was expressed by 7 (2.6% n=837) people that were sick during the time of interview, 4 (57.1%) of whom had previous history of the same syndrome (table 3). The distribution of the respondents according to the series of demographic variables was compared by the sources of treatment. Modern health care was mostly sought on equal basis from private HFs, as well as government HFs and less so from traditional healers as well as self-medication. No statistically significant differences were found between the proportions of the different demographic variables with respect to source of care ( table 4 &5). A small proportion of the respondents, reported the occurrence of combinations of the symptoms in the following order. Both dysuria and urethral discharge symptoms were reported by 30 (3.6% n = 842) respondents of whom 12 (40%) were males and the rest 18 (60%) were females. During the event of dysuria in this group, 23 respondents had to seek health care. Out of these, 13 (43.3%) attended private HFs, 9 (30.0%) went to government HFs and one had to go to a traditional healer. On the other hand, when they had urethral discharge, equal proportions of respondents (11 or 36.7%) sought health care from either private or government HFs. Discussion From this study, it is realized that STDs are highly prevalent in Oria village since it was possible for the villagers to recall their previous experiences for the three symptoms, i.e. dysuria, urethral discharge and genital ulcer. For dysuria, health care was sought from modern medicine (all other sources together) (98.7%) compared to traditional medicine (1.3%) in addressing STDs. This is similar to findings from a study in Zambia(4), where there were less responses pertaining to use of traditional healers compared to other sources of care although this proportion was larger in Zambia where they feel like combining the different forms of treatment (5) compared to their counterparts in Tanzania. Information on care seeking from traditional healers is probably more secret n Tanzania hence the small proportion of respondents who reported traditional healers as their source of health care. Unlike the two studies, a study done in the United States found that almost half of all respondents (49%) who had ever had an STD sought care from private practice while only 5% of respondents had sought treatment at an STD clinic (6). Urethral discharge as one of the STD symptoms, had majority of respondents (43.5%) attended in government HFs. This is a high proportion although not as high as the proportions encountered from a similar study conducted in Cameroon (7) whereby 53% of men with history of urethritis in the general population and 56% of factory employees with history of the same problem had sought care in the formal sector. Focusing on the different socio-demographic variables, majority of respondents with history of dysuria fell in the age group 15 – 19years. This group sought health care mostly from government and private HFs on equal basis. Fewer respondents sought care from other sources with no statistically significant differences observed between the different proportions pertaining to the sources of treatment. The same observations were made for religion, marital status, occupation, and educational status. Considering educational status as a possible influencing factor on choice of place for treatment, findings from the study conducted in Cameroon (7) found preference for formal health services to be associated with higher educational attainment. Although in Oria it was not so, it could probably be due to the fact that the vast majority of respondents were primary school leavers hence remaining with only a few having higher educational status. Having no association between any of the socio-demographic variables and choice of a particular place of treatment for the various STD symptoms found in this study is more or less similar situation that was reported in the study done in US where age, sexual history and geographic location did not predict particular types of treatment seeking (6). Comparison was also made between the proportions of respondents having previous history of symptoms, presence of current symptom, and appearing in both timings for the 3 symptoms “dysuria”, “urethral discharge” and “genital ulcer”. The proportions tend to decrease from previous history, current illness to a situation where one had a role in both. Such findings indicate that while some people get cured following health care seeking, some maintain the infections either from inadequate cure or from repeated infections from untreated contacts. It is not uncommon to encounter new infections. This study was not geared to explore such aspects. However, they are important and need to be explored and be taken care of should there be a need for having an effective STDs control programme. Conclusions and recommendations The occurrence of various STDs symptoms among the respondents is most likely indicative of the existence of high prevalence of STDs in Oria village. Although health care was sought from different sources with no particular influencing factor where the bulky of respondents sought care from government HFs followed by private HFs and less so to the rest, it is worth asking ourselves as “To what extent is the health care delivery system equipped to care for the growing need for STD management? The question is posed following the existence of the small proportion of respondents that expressed having STDs symptoms at the time of interview and which gave a previous history of the same problems doubting whether people treat themselves adequately! If this is not the case then people are re-infected from untreated partners or have new infections. In view of the findings of the above study, there is need for exploring the adequacy of the existing health services in caring for STDs need. Similarly there is need to increase the number of both private and public HFs geared in caring for the increasing demand of STDs management. Integration of the existing services with STD management is a strategy that will increase utilization. Provision of treatment to contacts through cases that reach HFs may lessen the burden of STDs. In attracting such customers, there is need to design different health education packages on STDs to target the different population segments. This should go hand in hand with the training of health care workers. Either frequent seminars on syndromic management of STDs (Skills) need to be organized especially for front line health workers. Acknowledgements Sincere gratitudes are conveyed to the Moshi District Medical Officer, Dr. E. Ngomuo and the research team for their tireless efforts during the data collection exercise in Oria village. The same goes to the Oria village community for their good cooperation during this survey. Special thanks are also due to Mr. F. Mayunga for computer data entry, and finally, the researchers are indebted to the Norwegian Universitie’s Committee for Development Research and Education (NUFU) for providing financial support. References
© Copyright 2004 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp04002t3.jpg] [lp04002t2.jpg] [lp04002t4.jpg] [lp04002t1.jpg] [lp04002t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}