 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 1, No. 1, Oct, 2004, pp. 11-17 The Tanzanian Policy on Health-Care Fee Waivers and Exemptions in Practice as Compared With Other Developing Countries: Evidence from Recent Local Studies and International Literature Godfrey Martin Mubyazi Department of Health Systems and Policy Research,
National Institute For Medical Research (NIMR), Ubwari Research Station, Muheza
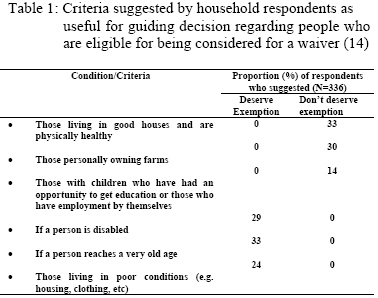
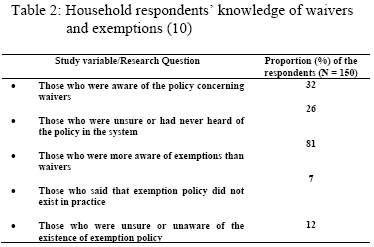
Tanga, Tanzania Code Number: lp04003 Abstract After introducing user charges in government hospitals and the presence of similar charges in the private health sector, the Tanzanian government established a policy for protecting poorest and vulnerable populations from healthcare charges. By citing evidence on similar experience from other developing countries, this paper presents, although in descriptive form, findings from technical research reports based on recent studies in Tanzania and critically analyses the relationship between government policy and its translation into practice. Evidence from previous but recent local studies indicates that while the policy explicitly identifies people with certain medical conditions as vulnerable groups eligible for exemptions, the issue of ‘waivers’ has been left to be decided at the discretion of local community leaders and health workers on ground that they know better the lifestyles, backgrounds and health conditions of the people surrounding them. This was viewed as a way of decentralizing decisions to local government authorities in granting such mechanisms to eligible people at the existing rates of health-care payments. This policy failure to define ‘who are the poor’ or how the poor should be assessed has caused confusion among health-care providers in identifying people who are eligible for waivers. It has also been used as a loophole for some health administrators to ignore people who deserve waivers since some people eligible for exemptions or waivers still pay either directly at the counter or indirectly under the table in order to get the better services they need. Other people delay or fail to contact health facilities due to lack of money or by avoiding the institutional bureaucracy in confirming who deserves a waiver. Some people do not benefit from exemptions because of lack of knowledge if they qualify and/or the procedures for presenting their claims. Meanwhile some exemptions are granted to people other than the targeted vulnerable groups. On the other hand, health workers hesitate to approve exemptions and waivers to avoid losing revenue on the side of their health facilities. Additional findings, discussions, conclusionand recommendations are presented. Key words: cost-sharing; waivers; exemptions; user-fees; care reform; Tanzania Introduction In the past two decades, the world has noted many developing countries putting great attention on cost- recovery financing systems such as user charges in their public health sectors, this being viewed as a means for improving efficiency in the financing and provision of quality health services to the majority of populations (1-2). In most publications, proponents of user charges argued that, if user charges are properly administered, they provide an opportunity for the realization of stable drug availability and other basic supplies, stimulate the working morale of health workers who may get incentives from savings of the revenue collected from patients, and increase the accountability of health providers who have to impress their clients (patients) by providing health careof desirable quality. However, in last decade (as is still the case today), there has been controversial arguments and research evidence that user charges have deterrent impact on the utilization of health care among the poorest income groups (1,3-8). The United Republic of Tanzania is one of the poorest countries in the world, whereby in the last two years, the country had an estimated annual per capita subsistence expenditure US $ 170 (9). The Ministry of Planning estimated that the country has had a total population close to 34 million by year 2001. The government introduced user charges as part of cost-sharing policy in public health facilities for grade 1 and level 2 services in year 1993, and on grade 3 services at referral and regional hospitals, fees were introduced in 1994 (10). Before that, all medical services delivered right from government (public) dispensaries through to health centres, district hospitals and even regional and national hospitals were free of charge to national citizens (11-12). The government waived medical charges for such levels of services in the 1960s with the ambition of enabling the poor majority of citizens to access them. The private-for-profit medical practice was banned in 1977 ten years after the Arusha Declaration of 1967, after which the government declared the principal of universal free medical services for all Tanzanians (11). But the private-for-profit medical practice was re-instituted in the formal health sector in 1991 in line with government’s structural adjustment programs (13-14). Due to their not-for-profit motivation, mission (voluntary agency) health facilities were allowed to continue charging their clients some modest fees as they have been doing since 1928 since they also attempted to waive the poor of such payments (10). Following the introduction of user charges in public health facilities, a number of public, research, and political concerns regarding their possible impact on the poor have risen, although on the other hand, the government’s cost sharing policy recommends that the very poorest population groups should not to be denied the service because of their inability to pay (11, 15-16). This paper is intended to share information with the international community about the Tanzanian policy of waivers and exemptions in the health-care delivery system implementing cost recovery programmes in medical services. Preceded by a description of the government cost sharing policy, the results section in this paper presents information formatted on two types of evidence: first, primary and secondary evidence on studies that took place recently in Tanzania. Second, citations of similar evidence as presented by other authors in international literature concerning the viability of such mechanisms in developing countries. Probably it would be useful to tell readers why I have seen it useful to develop this paper. After going through a number of publications in international literature, I discovered that despite several studies undertaken in the country and technical reports submitted to the Ministry of Health and other agencies, there is as yet no published article that systematically and in-depth has ever drawn and synthesised research findings to inform the international community about the status of health-care fee waivers and exemptions and the contemporary challenges facing health-care providers and the general public in translating the government policy into practice in Tanzania. It is widely known that much research findings remain unpublished in developing countries and by no means there is no exclusion of Tanzania. Tanzanian Government’s Policy of Waivers and Exemptions in Theory According to the government policy, exemptions are targeted to vulnerable groups. These have been defined to include pregnant mothers and children under the age of five years who are in greater chance of being affected by diseases, especially the communicable ones. These are directed to get free-of-charge medical services on essential reproductive and child health related problems. Also, the policy identifies people who are suffering from diseases such as diabetes, HIV/AIDS, leprosy, TB, polio, and cancer, as eligible for exemptions (11, 17-18). Furthermore, in 1999 the Minister for Health officially announced in one of the National Parliamentary Budget Sessions that all Tanzanian citizens aged 60 years and above should be exempt from user charges at government health facilities. The government emphasizes private-health care providers to administer exemptions and present their bills to the MoH for them to be compensated provided that appropriate procedures have been observed. As for waivers (a temporary relief that forgives patients who prove to be very poor and unable to pay), the government has made it clear that, these have to be granted based on the experience and discretion of health workers in consultation with local (community) leaders who may officially recommend people who are too poor to afford charges at health facilities. Results: Evidence on Government policy on waivers and exemptions in practice in Tanzania In a way to translate the policy into practice, the government funded and sent several officers from the MoH to Thailand to learn about design and administration of exemption card scheme for the purpose of learning what could be instituted (where desirable) in the national health-care cost-sharing system (11). Nevertheless, as yet there is no information published regarding the benefits gained from such a study visit and as yet no official exemption card (as it is in Thailand) has systematically been designed and officially implemented with input from the community. Also, as yet there is no standard criteria or characteristics officially provided to guide health-care providers and health facility administrators in identifying people who can’t afford to pay the existing rates of health-care charges. In my attempt to ask key informants at national, regional, district and health facility levels about the reason for the policy on waivers remaining ambiguous I have found that the decision regarding those who can’t afford top pay was left to local government leaders and health-care providers on ground that they know better the living conditions of the populations surrounding them. This verifies what was said earlier (8) that, ‘waiving the poor and exempting the vulnerable groups has remained part of the Tanzanian government health policy but little has been done to ensure their effective implementation’. And this statement supports what was said earlier (19) that, ‘in theory, charges might be made according to ability to pay. But this theory could not be applied in Tanzania because of the formidable, if not insoluble, problem of ascertaining income for every patient’. Several studies undertaken recently in the country concerning cost-sharing policy have reported quite similar findings concerning the practicality of waivers and exemptions. Case Study 1 – in two regions A study by Msamanga and others in 1995 covered 609 outpatients in Kilimanjaro and Mara Regions (14). The study adopted alternative data collection methods, including semistructured interviews with 609 outpatients (190 at public facilities, 256 at mission facilities, 149 at private-for-profit facilities), and 336 heads of households, FGD with some health workers and administrators, and self-administered questionnaires among some health workers at hospital outpatient departments. The study found that: 256 (42%) of the patients felt as qualifying for exemptions; patients attending private health facilities were less likely to ask for exemptions than those who contacted public and voluntary agency (mission) health facilities; 29 (4.7%) of patients confirmed to have ever benefited from exemptions at health facilities, and out of these, 17 (8.3%) were among those who were interviewed at public facilities, 5 (3.2%) were among those who were interviewed at private-for-profit facilities, while 6 (2.3%) were among those who were attended at mission facilities. Of the interviewed household members, the following are answers obtained from a number of patients interviewed at different health facilities in view the presence of poor people in their villages who deserved to be exempted from health-care charges: at public facilities 115 (84.5%); at mission facilities 66 (94.3%); at for-profit facilities 269 (89.4%). Asked further about the basis for identifying the poorest and the non-poor upon whom the decision for waivers could be made, household respondents mentioned the following (as presented in Table 1). Only 17 (5%) of the household respondents reported to know someone in the village who had benefited from an exemption. The authors also report that, while a little less than half of the health workers at public hospitals and about a quarter of those at mission health facilities experienced some involvement of the community in the decision procedures for granting waivers, none of their counterpart staff in private-for-profit facilities knew if there were any community involvement. Furthermore it is reported that, although there was a generally high awareness of the existence of user-fee waivers, 21.1% and 57.1% of health workers interviewed at public and at private-for-profit health facilities indicated not to appreciate if waivers were really implemented. Other results showed that, only 70%, 48% and 14% of health workers interviewed at public, mission, and for-profit health facilities respectively were aware of the government policy guideline that patients under vertical programs like TB/Leprosy etc. were supposed to be exempted from health-care user charges (although the report doesn’t show the number of staff interviewed). Furthermore the report identifies that, in general, 55% of the health workers (though the solid number of such health workers was not shown in the report) interviewed at all hospitals in both regions were confident that their clients knew of the existence of waivers/exemption system, although more proportionately health workers in public hospitals were sure about that, followed by those in the mission health facilities than their counterparts in the private-for-profit facilities. FGD participants in all types of hospitals acknowledged to be aware that some people are granted waivers, some of those who have no cash decide to opt for paying in-kindly (e.g. piece labour as agreed upon with the hospital administration) at mission health facilities, some get allowed to pay later after getting the service. For those who die before settling their bills, their relatives are sometimes exempted at private-for-profit hospitals. Case Study 2 - nationwide A study by Newbrander and Sacca covered health administrators and other health staff, exit hospital patients, and members of households living closer to health facilities. They also made a review of official documents concerning waivers and exemptions in the government cost-sharing policy. The team visited the Muhimbili National hospital, one regional hospital, four district hospitals, two mission hospitals, one private-for-profit hospital, and one parastatal organisation hospital. The study covered 187 patients at 8/10 hospitals, 150 household members, and health workers (total number not indicated in the report) at the hospital studied. Larger hospitals (regional/tertiary hospitals) had a permanent social welfare worker responsible for deciding on persons who were eligible for waivers, while exemptions were judged at clinical level based on laboratory test results. Only 2 hospitals were found with records on waivers and exemptions although they did not show any calculation of their actual costs. From the household respondents, Table 2 summarizes the main observations from the information collected: Overall more patients seemed to be aware of exemptions than waivers, although more than 94 (50%) of them did not know if exemptions existed for all diseases. Case Study 3 – in one district A study was undertaken in Korogwe district between April 1999 and May 2000 (16) to cover 451 individual household respondents, 442 exit patients at 11 health facilities (1 district hospital, 5 private-for-profit facilities, 5 mission facilities), 44 health staff at private health facilities, 29 local government (community) leaders, and 6 members of the district health management team (DHMT). Also, 24 focus group discussions (FGDs) were held with selected male and female village residents making a total of 261 participants the discussions. It was found that 21 (72%) of community leaders perceived that waivers were not known to most of the village residents, although they personally reported to be aware the policy. Such leaders defined the ‘very poor’ as people who are not able to work either because of their age e.g. the very old persons (60+ years) and young children or due to their permanent or prolonged ill-health conditions or body disfiguring e.g. the disabled. Only 102 (23%) of patients reported to have had been aware of the existence of waivers and exemption policy, 71 (16%) said that the policy did not exist, while the majority 270 (61%) were not sure. Twenty two (50%) staff at private health facilities reported to have had never witnessed a waiver being granted to any patient, 8 (20%) were not sure whether they mechanism really existed at all, while 13 (30%) reported to have waived some patients. Meanwhile 8 (28%) of community leaders reported to have had recommended a few villagers to be considered for waivers by health facility administrators, although they could not confirm whether or not their recommendations were accepted. In addition, 10 (83%) of mission health facility staff reported that waivers were being implemented at their health facilities. Despite report from district level health staff, administrators and health managers that waivers and exemptions were actually granted as recommended, no substantial records were obtained to confirm this. It was only for year 1999 when it was indicated that only 9 patients were waived of user charges at the district hospital. In general, the characteristics of patients who were granted waivers, as reported by the District Health Management Team members and other health staff at private health facilities include the following: when a patient admitted while seeming to be poor has stayed at the health facility for a long time, and physical appearance of the patient in addition to the patient’s or their relatives’ self-expression, e.g. most disabled people automatically get waivers. As for exemptions, children under five years, the elderly, people suffering from certain diseases (as per government guideline), were mentioned. The majority of FGD participants especially in rural villages were not in support of the question that waivers were actually granted at the district hospital and private-for-profit health facilities, while there was a great acknowledgement that mission health facilities were more considerate in case a patient proved to be unable to pay. The discussants argued that, apart from health workers (under the matronship or patronship of a Priest or Sister) looking at the patient condition themselves and making immediate decision to waive someone or ask him/her to pay later after recovery, a letter of recommendation from any respected community leader was also used as a basis for granting a waiver at mission facilities. Case Study 4 – in one district In a study undertaken in Kwimba district along Lake Victoria in northwest Tanzania (20), opinions were collected 500 outpatients, 293 inpatients, 1500 householders and 22 FGD participants regarding specific population groups who deserve exemptions. The following groups were identified: underfives 1011 (44%), disabled 971 (42%), and the elderly 746 (33%). Similarly, 20 (91%) FGD groups mentioned the disabled, 18 (82%) groups proposed underfives, 5 (23%) groups identified pregnant women while 2 groups proposed schoolchildren. Evidence about whether exemptions were granted in practice was limited. Case Study 5 – nationwide Another study is the one that was undertaken by three officers of the Cost Sharing Implementation Unit at the Ministry of Health to assess, among other things, the implementation of the waivers and exemption policy, availability of information to patients and the general public and the cost of exemptions granted (17). The study covered 13 hospitals including two voluntary agency tertiary referral hospitals (Bugando under Roman Catholic Church) and Kilimanjaro Christian Medical College (KCMC) in Moshi (under The Lutheran Church), five regional government hospitals and six district government hospitals. The government hospitals include those that had at least implemented user fees at least in the last 12 months (since before July 1993 health services at government health facilities were free of charge throughout the country). The sample population interviewed was 776, including 368 health workers, 52 members of hospital advisory committees, and 356 patients or their escorts, and of these 41% were males and 59% were females. The research team also observed the existence of posters about waivers and exemptions at the study hospitals. It was found that, all the hospitals had established an exemption mechanism, and there was a personnel responsible for administering waivers to patients in need, although few hospitals had posters indicating the existence of the waivers mechanism. Also, information collected from some of the health facilities indicated in the period of the last six months (July-December) of year 1995, a total of 103,913 people were exempted and these were correctly people targeted by the national policy. In absolute terms, records showed that more exemptions and waivers were granted at regional hospitals, followed by tertiary hospitals. The study report reviewed does not, however, indicate any evidence for difficulties or drawbacks faced by health workers in administering waivers. Evidence on the problems limiting the practice of waivers and exemption in Tanzania Msamanga’s team noted health workers complaining against the tendency of some patients claiming for waivers while they could afford to pay and the lack of explicit official criteria for identifying those unable to pay. In private-for-profit health facilities, it is reported that, there were too much blames from both patients who felt that exemptions are not granted as desired and from hospital administrators who disliked seeing many patients waived since this would lower their profit. In Newbrander and Sacca’s research report (18), it is documented that, altruistic motives do not appear to exist in government facilities to the same degree as in mission facilities, as social workers at government facilities displayed strong negative attitude to the idea that a patient is really unable to pay. Another observation made is that, although exemptions are also granted to the poor owing to the fact that most of patients who present conditions of vulnerability as stated in the government policy guidelines are also poor. Likewise some government hospitals opted not to implement the exemption policy because the hospital administration emphasized revenue generation. It is also reported that, some facilities do not want to publicize waivers and exemptions in order to avoid abuse. Like Gilson, the authors remark that, ‘the theoretical construct of the waiver mechanism is sound, but its implementation is flawed’ (18). Likewise, in the Korogwe district case (16), the majority of FGD participants showed their little belief that even if the government policy exists on paper, not all health workers appreciate to put it into real action. Some of the respondents reported to have even witnessed some patients being denied of service at private health facilities because they had no money to pay. At the Magunga district hospital, some health staff the author of this article that, sometimes whenever they were personally on duty and came to be consulted by patients who complained to have no money to pay, the staff had been finding it even more convenient to pay for such patients from their own pockets and avoid following up all the too bureaucratic (and yet) unreliable procedures for reporting to the hospital administration. It was also reported by community leaders that sometimes they write letters to health facility management to recommend people like widows and very old persons but in most cases their letters are not approved. There was also a concern among FGD participants and some local government leaders that, even if the government decided to announce waivers, some people do not have a radio in their homes while others do not read newspapers either because of lack of money to buy them or due to their low reading culture of things like newspapers. Case Study 6 – in one district Reports from Kilombero district suggest that some household respondents recognized some village residents who due to their inability to pay user fees, some either stayed at home trying alternative medication or end up incurring higher costs such as selling household property or asking for assistance from a friend or relative (21). Meaning of poverty and international experience with waivers and exemptions in health Barker (22) argues that most people would regard poor people as those having inadequate money, or inadequate food. The author criticize this narrow definition by saying that it is almost impossible to achieve what is enough since some people have different needs and priorities and different ideas about what constitutes poverty. Meanwhile, the author acknowledges the difficulty of having a standard definition of poverty. With experience from Ghana, Wadington and Asiama (23) observed that, “we learnt two lessons about exemptions. First, rules have to be clear. Stating that ‘poor people’ should be exempt is too vague. You need to decide who should identify the poor people and what definition of ‘poor’ should be used”. Other authors also appreciate the difficulty of such a definition (6,24-26). Meanwhile, reports from Thailand indicate that in 1990 the Ministry of Public Health played a proactive role in identifying the poor and encouraging them to receive cards (27). And one way was to use criteria other than income assessment, such as housing conditions and whether people came from vulnerable groups such as landless farmers, migrant workers, or ethnic minorities. For this reason, procedures for issuing the cards became easier and simpler in such a way that by 1993 about 20% of the Thai population were covered by the free card scheme, more coverage being in rural areas than in prosperous urban residents. It has been reported that, inadequate translation of exemption policies into practice has partly been attributed to the reluctance of health providers to grant them on ground that they would bear the cost themselves (7-8, 28-29). Similarly, in accounting for the actual situation in sub-Saharan African in general, exemptions are rarely, if ever, implemented since the primary objective of the fee system is financial sustainability, as the Bamako Initiative type of scheme, because of their effect on lowering levels of revenue generation (8). In Kenya, it was found that, health facility managers had no uniform way of dealing with patients who were unable to afford medical care charges, as there was no formal system of exempting the poor, and this being due to the MoH leaving exemptions to be judged based on the discretion of health facility managers, some of whom treated patients on credit, others treated them free of charge, while others turned them away (30). A similar situation was reported from Zimbabwe (7). The latter authors continue identifying that in a number of sub-Saharan African countries also the coverage of waivers is inhibited by the reluctance of some eligible patients to ask for them and their stigma to seek treatment. Even countries like Thailand and Vietnam that have moved a sound step in designing an exemption card system to protect the poor face leakages and other shortcomings (28, 31-32). Discussion In light of the evidence cited above, it is appreciable that targeting waivers to all the real poor is not as easy as the policy advocates. It is obvious that without a clear definition and explicit criteria for identifying the poor and systematic ways to monitor the administration of such mechanisms, it becomes difficult for the eligible populations to benefit as the policy expects them to be. As reported from other African countries, the possibility of some poor populations in a community having a stigma to apply for waivers in Tanzania cannot be underrated. In some communities there are likely to be populations who on ground of wanting to maintain their social dignity, they might feel ashamed of being seen or heard of asking for waivers in the medical care system, particularly where there is a system for the community to be informed of those who were waived. Little systematic behavioural research has been carried out to establish personal reasons other than institutional factors that inhibit a person to hesitate to seek/ask for waivers at health facilities in a developing country like Tanzania. In Swahili language, there is a common saying that, ‘Maskini Jeuri’ meaning ‘a proud poor’, which is often used when people want to tell others that despite their being poor they can manage to do what they want for their survival and therefore they should not be mistreated or to be told to do what they don’t want to do. On the other hand, it is obvious that without the government ensuring compensation of health-care providers for the medical services they might have had provided to eligible patients, there will be little incentive for the care providers especially in the private-for-profit facilities to implement exemptions and waivers as the policy directs. Increasing overemphasis by governments on efficiency driven by higher motivation for revenue collection to recover the cost of medical care services is likely to compromise the efforts to ensure that the poor are protected. There is also another issue that has never been made clear in most national policies concerning exemptions of underfives. The policy is supposed to be specific by stating which types of health facilities should exempt underfives and for which types of illnesses. It is likely to remain difficult both to public and private-for-profit agencies to adhere to such a policy if in addition to the fact that they are clear arrangement for them being compensated for the exemptions they may provide to various categories of patients, it would be a nightmare if it were decided to exempt all underfives attended at health facilities regardless of the type of diagnosis. In areas like Tanzania where most of the underfives are attended either at outpatient departments or admitted in wards due to illnesses related to malaria, acute respiratory tract infections, diarrhoeal diseases and pneumonia it means that if exemptions were granted based jut on the policy statement ‘exempt all the underfives and pregnant women’, it would be impossible for the health service to be recovered even by 5-10% of the actual cost of their delivery. It is possibly this reason that some health workers and health facility managers feel reluctant to exempt many patients, and it is probably this reason that partly has made national policy makers in Tanzania decide to leave the statement ‘exempt the underfives’ as open and vague as it is. Russell argues that, in serious conditions of poverty, health-care payments can be made at the expense of an individual or household losing other household or family properties, thus implying a high opportunity cost on the side of the patients and/or their relatives (33). It should therefore be borne in mind that, assessing poverty by relying on factors like one’s house condition, level of education of their children or relatives, ownership of property like radio, TV, bicycle, etc. should just be taken as proxy and temporary indicators rather than being regarded as permanent and confirmatory indicators of ability to pay. Consider a woman living in a good house owned by her husband, or whose family has a large plot of land and many cows owned by a husband or some other family members, as is in most traditional African societies, it may be a great mistake to directly conclude that such kind of woman can afford medical care charges even if she is complaining of having no money. This brings us to the point that, in most African communities, it may be important to consider the intra-household relationships with a gender perspective if we really want to establish a sound system of developing criteria for targeting subsidies to eligible populations. Evidence from the three of the six case studies in Tanzania as cited in this paper indicates that compared with private-for-profit and government health workers, those at mission health facilities were more willing to assist those who find it difficult to pay for medical services. This is possibly due to the fact that they are not-for-profit in nature as their services are driven by faith (i.e. they are ‘faith-based health institutions’). However, we cannot underscore the fact that by virtue of their faith and nature of their activities, they receive various government tax subsidies more than or unlike the private-for-profit entities. Most of them also get subsidies or sponsorship from other mission communities or organizations abroad, which assures them to survive as compared with other health facilities. But for the purely government health facilities, failure to grant waivers and exemptions in the appropriate way should be unnecessary since they also receive various government subsidies from the government and in most cases their mission is to provide equitable and affordable services rather than generating profit. Conclusions and Recommendations There are mixed evidence regarding the practicality and limitations of administering exemptions and waivers in the Tanzanian health care system. Almost all the case studies indicate the existence of such protective mechanisms both at public and private health facilities but to a limited scale. It generally remains evident that targeting the poor through the waiver system is rather difficult to implement in Tanzanian settings than the government policy stipulates, and this makes the whole cost sharing policy questionable on its effects on the poor. Probably Tanzania like other countries would gain from Thailand’s experience with the exemption card system had there been a deliberate attempt to develop one since as yet no systematic strategy is in place to grasp such an opportunity. This does, however, not mean that all countries have to copy exactly the same system as the Thai’s case, but at least to pilot the system in some areas to see if it can work before it can be adopted throughout the country. A systematic intersectoral research approach led by experts in the socio-economic and epidemediological arena in collaboration with the experience of local community leaders can be useful towards reaching a commonly acceptable formula for identifying the too poor to pay. As in other health policy reform programs, the policy on exemptions and waiver is a process that can be modified with time neither can it directly satisfy all populations overnight. While this should not be a reason for the governments and other parties concerned to take appropriate action, it is important for governments to create an enabling environment for the policy to work, including periodical monitoring and consultations to evaluate the progress with the view to modifying where necessary e.g. monitoring leakages and abuses that can be contributed by some community leaders or health administrators with habits of nepotism or accepting payments under-the-table from patients who ask to be considered for waivers. As was partially done in the study by Mmbuji’s team, it would be much more informative if more studies were conducted to evaluate the cost of exemptions and how health facilities have improved their system of record keeping and reporting on such targeting mechanisms. This would help to widen the base of evidence and reduce any dissatisfaction by health-care providers and the government who might feel that the policy is well implemented but not supported by research findings. This is because of my experience from Tanzania that, sometimes national policy makers and health care manager of health facilities get disappointed when they hear about or personally see research presentations indicating that in real situation, there the poor translation of policy into practice. Acknowledgement To all authors appearing in peer reviewed journal, and those who published books and researchers whose papers and technical reports, as well as the government of Tanzania whose official health policy documents have provided reference for this paper. I am also grateful for comments and moral support from Prof. Norman Hearst of the University of California, San Francisco (USA), on the initial draft manuscript of this paper when we met for the first time in a TDR Workshop in Bangkok in year 2001. Again, I thank the two editors of the Tropical Medicine and International Health Journal who constructively commented on the earlier manuscript I submitted for review and consideration for publication, including their encouragement for me to revise some sections of the paper and to resubmit it to that journal or elsewhere. In addition, I wish to remember the useful opinions and answers obtained from the study populations in all the case studies referred to in this paper, and the cooperation I got from my colleagues at Amani Medical Research Centre with whom we worked together in Korogwe district, Tanzania, their names are as indicated in two of the above referenced publications we developed together. The Director General of NIMR on behalf of the Medical Research Coordinating Committee and the Ministry of Health, Tanzania is thanked for providing permission for this manuscript to be submitted for publication in an international journal. I can’t forget my tutors at the Nuffield Institute For Health, University of Leeds in the UK who equipped me with useful analytical skills while I was doing my M.A. degree in Health Management, Planning and Policy between 1997-1998. Our research project in Korogwe district would not be carried out without funding from USAID through Abt Associates Inc. under the PHR Project, although the views/opinions presented in this paper are those of the author and not necessarily of Abt Associates Inc. nor USAID. References
© Copyright 2004 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp04003t2.jpg] [lp04003t1.jpg] |
| |||||||||

{kind=link}
{kind=link}