 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 1, No. 1, Oct, 2004, pp. 33-40 Health Sector Reforms and Decentralization in Tanzania: The Case of Expanded Program on Immunization at National Level Innocent AJ Semali1, Don de Savigny2, Marcel Tanner3 and Caroline Akim4 Dept. of Epidemiology and Biostatistics, 2Research
Manager, Tanzania Essential Health Intervention Project, Dar es Salaam
Tanzania, 3Director, Swiss Tropical Institute, University of Basel,
Basel Switzerland, 4Manager; Expanded Program on Immunization
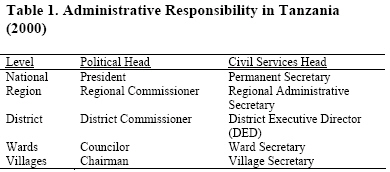
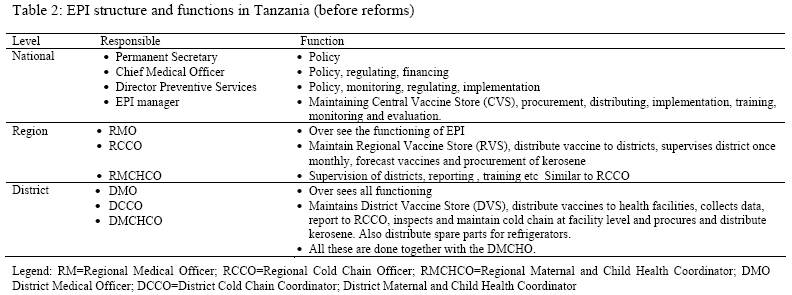
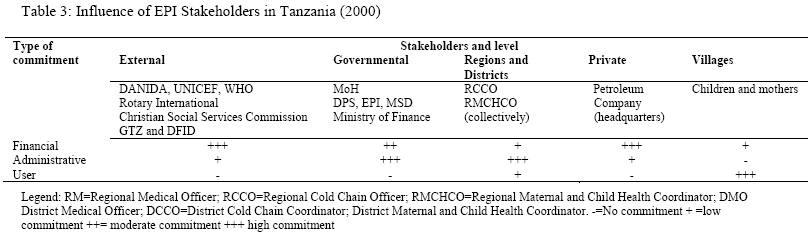
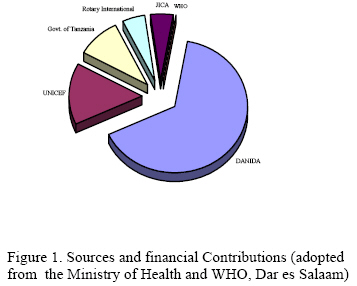
program. Ministry of Health Tanzania. Code Number: lp04006 Abstract Following successful establishment of Expanded Program on Immunization (EPI) in the 1970’s as vertical program, the burden of disease for many of the vaccine preventable diseases was pushed to low levels. The current round of health reforms in Tanzania calls for decentralization and integration of vertical programs. This has the potential to assist or erode generally good performance of EPI. Reforms on the programme have been undertaken in Tanzania since 1996, and have included 1) integration of the procurement, storage, and distribution of vaccine and related equipment into the operations of a quasi-autonomous drug procurement agency. 2) government financing of procurement of the oral polio vaccine, cold chain kerosene, and 3) the integration of kerosene and vaccine distribution, supervision and monitoring to district health system. Our analysis shows that the integration of the procurement and distribution of vaccines into the operations of the drug procurement agency, and privatization of the distribution of the cold chain kerosene initially stalled EPI reforms for several reasons and had an adverse effect on EPI decentralization and coverage. The major cause of the problems was opposition from the EPI providers at district level who had to accept decreased income consequent to the reforms. We conclude that greater involvement of all stakeholders in the planning of the programme, would have presented an opportunity for forecasting the opposition and developing mitigating strategies. Introduction This paper presents an analysis of the extent stakeholders enhanced or retarded reforms in vertical program in developing countries using Extended Program on Immunization (EPI) as a case study. Among developing countries vaccine preventable diseases were the fourth cause of the remaining burden of disease (1). This was the situation after more than ten years from launching of EPI. There was an overall increase in the EPI coverage and parallel reduction of mortality among children under five years and infants. The UNICEF report on the State of the World Children in 1994 observed that among other countries Tanzania from 1960s to 1992 achieved mortality reduction among children under five years old from 249 per 1000 to 176 per 1000, and among infants dropped from 147 to 111 per 1000. Vaccination coverage had also increased to about 82 percent (2) The successes and remaining challenges in health were apparent by the early 1990s when most countries started to reform their health sectors (3). Developing countries including Tanzania started to implement health sector reforms with the objective to increase health system efficiency and financing (4) The current round of health reforms in Tanzania calls for decentralization and integration of vertical programs such as EPI. This has the potential to assist or erode the generally good performance of EPI and observed need to reduce burden of disease among the target population. The EPI reforms are addressing financing, decentralization, and integration of some generic functions. Notwithstanding the good intensions of the reforms, the process should avoid triggering opposition from any of the stakeholders, since such a situation could stall the implementation momentum of an effective intervention, cause a reversal of the reforms, or even loss of the earlier gains. The pre-reform situation analyses should, among other things, identify the interests of each of the stakeholders so that appropriate adjustments are made in the reforming process. This analysis of the Tanzania Mainland EPI reforms was undertaken with the objectives of evaluating process performance, and identification of issues requiring the attention of policy makers for future reforms. This study focused at the program level at national level. Integration of vertical programs to the main health care system is one of the health sector reform strategies. There are several benefits that are associated with integration and include increased utilization, coverage, improved quality and cost-effectiveness(5-6). There are similarities and synergies between vertical programs and health sector reforms. The similarities include having similar goals to improve access, high quality care, integrated approach, decentralization and finally improved health of the people(7). There are also conflicts between health sector reforms and vertical programmes and include possibilities of neglect of vertical programs in resource allocation, risk of being transformed to another vertical program, cost saving will override access and donor unwillingness to disburse funds. Thus there are concomitant threats to achieving the objectives of both. It has been proposed that in order to realize the objectives strategies to increase resources, human capacity and community participation need to be adopted(8). Thus resource input and careful balancing in prioritization process are need to safeguard reform and vertical program objectives. The study was undertaken to answer the question “what is the role of stakeholders in the process to integrate EPI to the general health care services?” Integration and decentralization is a political process that attracts stakeholders(9-10). Policy analysis framework was then adopted to answer the question. It was also assumed here that integration as a policy change altered equilibrium that existed. Consequently those affected by the alteration could affect the integration process at any stage(11). Thus the interactive model of implementing policy reforms was then adopted in this analysis. The period of the reforms targeted by this analysis is from 1995 to 2001. The study used document review, secondary data analysis, in-depth interviews and key informant. A search was conducted to retrieve published and un-published documents from the Ministry of Health, EPI offices, Medicals Stores Department, regions and districts. The documents were filed chronologically starting from 1995 a year before the reforms started. The initial review was to answer two baseline questions that were what were the reforms and integrations that took place in the EPI and progress each year to 2001. The second question was who were the stakeholders at each point in time since 1995 and their role. From the documents stakeholders were identified and their relation to the EPI program was identified. The stakeholders were groped in to those who provided funds, political support and administrative and users. Having reviewed some of the documents it was realized that procurement storage of vaccine and kerosene supply were issues being contested highly. Thus at national level the analysis focused on integration of procurement and distribution of vaccine. The study identified goals, strategies and activities to meet the desired goals and time lines. At each point in time the support or opposition of identified stakeholders on goals, strategies or activities was assessed. The extent of support was decided from the amount of financial resources, administrative, implementation and other activities directed to EPI. After review it was then decided that +++ was high support, ++ medium support and + minimal support. Subsequently an assessment was done to find out whether there has been a progressions, stagnation or reversal of the refrom process. The findings were discussed with key stakeholders who clarified and confirmed the findings. Records on EPI vaccine procurement and distribution from 1995 to 2001 were retrieved. Data on EPI vaccine received in six regions were also retrieved from three regions. This was to validate central data on amount of vaccine distributed to regions. I all three comparisons there was no discrepancy between regional and central records, hence it was concluded regional records at national level reflected truly the amount of vaccine distributed to the regions. The data was then entered in a Microsoft Excel and secondary analysis was then done. The findings were discussed with one key informant to clarify the findings. Reference and vaccination target populations were estimated using the National 1988 Census data and growth rates. The population at each point in time was estimated using exponential population growth model (12) Study settings included national, regions and districts. Documents studied included documents from the EPI Management Unit such as the programme’s annual and other reports from districts, regions, and zones. The other information sources were consultants’ reports, proceedings and minutes of various meetings, open administrative files, and delivery records of vaccines from EPI and the Medical Stores Department (MSD) to the regions and districts. In depth interviews were also held with key officials at the Ministry of Health (MoH), EPI Management Unit, MSD, Regional Cold Chain Officers (RCCOs), District Cold Chain Officers (DCCOs), and District Executive Directors (DEDs). Results Administrative setting Overall administration in Tanzania rests with the President who is the Head of the State. Under the president are political and civil servant leaders as illustrated by the administrative structure in table 1 by 2001. For the current health sector reforms, the major EPI stakeholders at the national level are the policy and decision makers in the MoH, Ministry of Regional Administration and Local Government (MoRALG), and Ministry of Finance (MoF). Pre-Reforms National EPI and Functions EPI was established in Tanzania in 1974 as a vertical programme funded by donors and the central government. Early success of EPI included the establishment of an efficient EPI infrastructure, and increasing EPI coverage from 15% to about 80% in the 1990s (13). The national EPI structure and functions of the stakeholders in the health sector at the national, regional, and district levels are summarized in table 2. Several stakeholders were active within the EPI services before reforms. These can be categorized as government, external, or private. The Ministry of Health was leading among the stakeholders with the EPI Program Manager as a key advisor of the Ministry on issues of EPI and a link between the Ministry, regions and districts. MoH operational staffs in the regions, districts and facilities were recognized to have low morale due to poor remuneration and physical quality of the health facilities services (14) In context EPI regional and district level managers (RCCOs, RMCHCOc, DCCOs, DMCHCOs and RCCOs) had access to self -driven EPI vehicles and predictable extra income as daily subsistence allowances. These stakeholders could be expected to resist reforms that would decrease their extra income and associated benefits. Pre-Reforms Positioning of Known Stakeholders The stakeholders before and after reforms remained the same. The level and type of commitment to EPI operations of all known stakeholders at the national, regional, district, and village levels are shown in Table 3. The major roles of the external stakeholders were mostly financing the programme and technical backstopping at the national level. The World Health Organization (WHO) facilitated the availability of technical expertise and training. Besides monitoring the quality and quantity of vaccines, UNICEF promoted immunization at the regional, district, and village levels. Thus donors wielded the financial power while the government and districts shared the administrative power. Pre-Reforms Funding and Distribution of Supplies External stakeholders met most of the EPI programme costs (Figure 1). Indeed some external stakeholders supported procurement of specific vaccines. Since there was no traditional donor for the Oral Polio Vaccine (OPV), its availability was intermittent resulting in recurrent shortages (15). External stakeholders met the costs for fueling the cold chain but its financial management and procurement was already decentralized. However, the government district and regional accounting systems failed to account adequately for donor funds spent on cold chain kerosene procured by the district (16) Pre-Reform Coordination of Stakeholders Interaction among stakeholders was provided through the EPI management and the Technical Committee on Immunization, whose members were drawn from the MoH, donors, co-opted institutions and individuals. There was, in addition, the Interagency Coordinating Committee with members from MoH, and donors; and the Health and Population Committee whose membership was restricted to donors only. They meet regularly on monthly and make very important decisions on funding and progress of EPI. Interaction at the regional and district levels is facilitated by the:
Thus these bodies were functional and effective to a large extent. Policy Goals for the EPI Reforms The EPI policy goals for the reforms for Tanzania Mainland were coverage of 90% for all antigens for children under one year by 2004; coverage of 90% for tetanus toxoid for pregnant women by 2004; polio eradication by 2003; elimination of neonatal tetanus by 2003; control of measles and hepatitis B infection (Ministry of Health Tanzania Mainland, 2000). Strategies for the EPI Reforms
Major Issues for the Reforms
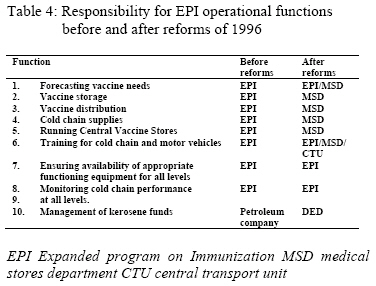
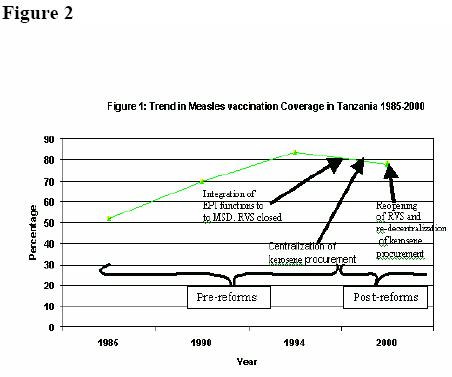
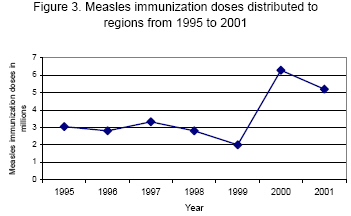
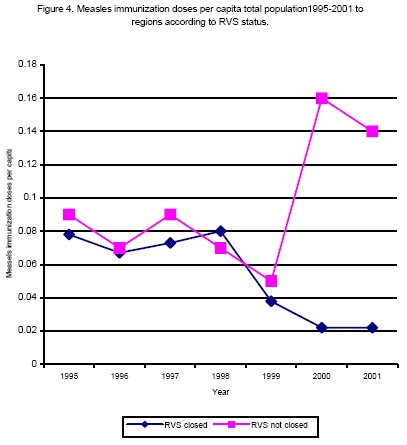
EPI and MSD Agreement MSD was previously known as Central Medical Stores (CMS). It was a unit in the Ministry of Health responsible for procurement, storage and distribution of drugs and equipment to the districts. In the early 1990s DANIDA assisted to rehabilitate CMS and it was transformed to a semi-autonomous Government agency under the Ministry of Health known as Medical Stores Department. The ongoing health sector reforms included integration of EPI generic functions to MSD. The EPI and MSD signed the Transfer of Selected Activities of EPI into MSD Operations to effect the integration of procurement, storage, and distribution of vaccines and related equipment into the operations of the latter. Under the agreement, EPI retained the last say on who should be the supplier, and on distribution instructions for the supplies and equipment. The reforms were to be implemented in two phases. During Phase one starting in July 1996, the Central Vaccines Store (CVS) at the national level was moved to MSD, which therefore on EPI instructions supplied distributed and transported vaccines and related equipment to Regional Vaccines Stores (RVS) and District Vaccines Stores (DVS). Front line health care facilities collected their requirements from DVS. Phase two of the integration agreement started in 1998, and was to involve closure of RVS and transferring their functions to the Zonal MSD stores. The RVS closure was to be staggered by regions, and the initial closures affected Dodoma, Morogoro, Coast, Dar es Salaam City, Lindi and Mtwara regions. The 1998 EPI annual review meeting attended by all DCCOs, DMCHCOs, RCCOs and RMCHCOs reported that EPI coverage was falling because of the reforms(Ministry of Health, 1999b). In the same year regional medical officers in their annual regional medical officers meeting discussed the report on falling EPI coverage due to reforms. The annual regional medical officers meeting recommended that a study should be done to determine the impact of HSR on EPI services in the country. The MOH concurred and directed that further integration of EPI functions to MSD should stop until evaluation of the performance in the six regions that had closed their RVS was done. The MOH appointed an evaluation team that did the evaluation from December 1998 to February 1999. The report of the evaluation concluded that there was falling of EPI coverage due to the reforms thus concurring with the RMO conference and EPI annual review meetings. A lesson that emerged was to reopen the closed RVS. On September 1st, 1999 the MOH wrote a letter to MSD instructing them to restore the RVS immediately. Since then (September 1999) there was several communications between the MoH and the MSD. The main subjects were, concerns that information available to MoH was not similarly made available to MSD, reforms did not affect EPI performance and need to form a joint team to evaluate former sites of the closed RVS. In December 2000 (more than a year later) MoH and MSD formed the joint team that completed its work January 2001. Its recommendation was that the equipment and buildings were in good state and that the RVS could be restored immediately. The MOH officially informed MSD on the findings and instructed them to comply and the restoration process started. The ministry managed to reverse the situation using evidence available along with pressure from the RCCO, RMCHCO, DCCO, DMCHCO and RMO. The two (MOH and MSD) managed to work together to finalize reversal of RVS closure. Procurement of OPV In 1998 the government took over the responsibility of funding the procurement of OPV through its contribution to the Vaccine Independence Initiative (VII) Cold Chain Kerosene Since establishment of EPI in late 1970s kerosene for powering the cold chain refrigerators was purchased at district level. Funds were disbursed from the center through RCCO to DCCO via the DMO. Review of the previous annual EPI evaluation meetings most often the Ministry made call to the districts to properly use kerosene funds as well as being accountable. Interview of key informants revealed that some of the providers diverted kerosene funds or the kerosene for other uses. One of the informants in addition revealed substantial financial irregularities were discovered when an auditing firm was commissioned to audit kerosene funds at district level. The reforms affecting financing and distribution of cold chain kerosene aimed at rectifying its mismanagement by districts, improving accountability for funds used for the purpose, and timely disbursement of funds. In January 1999 the MoH entered into an agreement with a trans-national petroleum company with a network of franchised fuel stations at rural level to supply kerosene to all districts. This petroleum company was one among which the Government had shares. According to the agreement, MoH paid the petroleum company headquarters to reimburse upcountry franchised petroleum service stations for the kerosene supplied to EPI at district level. The agreement was made as an emergency and on the assumption that the petroleum company headquarters had authority over upcountry branches and service stations in the districts, and that it had service stations in each of the 121 districts in the country. In fact the petroleum company had only 58 service stations in the whole country compared to 121 districts. Thirty-five (60.3 percent) of the services stations were concentrated on the main paved roads covering four (19.0 percent) of the regions. During the subsequent annual EPI evaluation meetings attended by the RCCOs and DCCOs and also letters to the ministry there were several complaints of shortage of kerosene. Interviews with key informants revealed three problems associated with the shortage. Districts without a franchised petroleum service station had to get kerosene from the nearest district and pay the transportation cost. Some had found the cost to be so high that they had to negotiate with the franchised petroleum service station to give them discounted equivalent cash to purchase kerosene from a more convenient source. It was a departure from the usual cash-based transactions of the franchise stations that would now need to operate on trust that they would be reimbursed for EPI kerosene by their headquarters. Interviews revealed that districts had to operate with full cash otherwise they got only a small proportion of the required kerosene on credit. Three interviewees each from a different districts reported that at some time kerosene transported from franchised petroleum service stations was contaminated, refrigerators stopped working and it had to be discarded. The lesson that emerged was that kerosene funds should again be sent directly to the districts directly instead of contracting the petroleum company to supply kerosene and that districts would purchase from the nearest local supplier. The option of sending funds to districts through the National AIDS Control Program (NACP) financial disbursement system was considered costly because it would involve use of Micro Finance Bank and too many hands namely MoH, NACP, Regional AIDS Control Coordinator, and DED and complex accountability. Pre- and Post-Reforms EPI Operational Functions The EPI operational functions by actor before and after the reforms are summarized in Table 4. Performance of the Reforms The 1998 EPI annual review meeting reported that vaccination coverage in the country was falling, and attributed the decline to the reforms. The Annual Conference of Regional Medical Officers made the same observation (13). Figure 2 shows the trend of measles vaccine coverage with time since early 1980s. The coverage increased rapidly to above 80 percent in 1992, after which it started falling gradually (four years before the EPI reforms started). The claim by the DCCOs, DMCHCOs, RCCOs and RMCHCOs that EPI coverage was falling due to reforms was not actually supported by the data. Figure 3 shows the measles vaccine as a tracer antigen for vaccine amounts delivered to the regions for the period 1995 to 2001 covering both the pre- and post-reform periods. Although the vaccine amounts delivered were erratic, there was no significant reduction in the amounts. Figure 4 compares the delivered measles vaccine doses per capita for the regions with and without closed Regional Vaccine Store. Here it is drawn that there was no significant difference of doses received between regions between 1997 and 2000. From 2000 and after the reversal the regions in which Regional Vaccine Store were closed received significantly fewer doses of measles vaccine per capita. An interview with one of the key informants revealed that amounts delivered was exactly what each respective region ordered. Thus less amount of vaccine delivered to regions in which Regional Vaccine Store reflected management decisions in those regions. Kerosene Supplies Shortly after the petroleum company started to distribute cold chain kerosene the MoH began receiving regular complaints from RMO, RCCO and DCCO that cold chain was performing poorly due to kerosene shortage. Reports elicited by the interviews showed that some of the problems were pilferages in the cold chain kerosene delivered to health facilities, some deliveries were contaminated, and non-availability at places of procurement. Upcountry petroleum services stations preferred doing business on cash basis, and were both administratively and financially decentralized. The petroleum company headquarters attributed some of these problems to a communication breakdown between RMOs and the upcountry company branches. Kerosene supply remained erratic in the districts until April 2000 when the MOH concluded that erratic kerosene supply was the leading cause of falling EPI coverage. A decision was made to stop the petroleum company from any further distribution of kerosene. Several options for sending funds to districts were considered at length. When consulted on the problem of disbursing finances to districts, MoF offered to disburse the kerosene funds directly to districts starting July 2001. It then needed interim arrangements to procure kerosene for districts until when MoF finance took over. The discussions took time to be concluded during which there was no sustainable kerosene availability in the districts thus compromising further EPI coverage. Discussion The analysis aimed at understanding the role and reactions of stakeholders in the process to implement EPI decentralization, at national level and impact on EPI services. The study found that there was a substantial stakeholders’ opposition to the EPI reforms that involved vaccine and kerosene procurement and distribution policies, particularly from the cold chain operators and other MoH implementers namely the RCCOs, RMCHCOs, DCCOs and DMCHCOs. Further analysis of vaccine delivery showed that there was no reduction of vaccine delivery following the reforms. Another analysis of trends in measles vaccine coverage revealed that EPI coverage started to fall since 1990 about six years before the EPI reforms. Thus the analysis did not support the reaction of stakeholders to oppose the reforms. The decisions were based on anecdotal statements made during the meetings without thorough analysis. Hence the integration of vaccine supply to MSD was partially achieved. Since decisions in EPI operation were often based on anecdotal evidences there is a need of generating data and doing proper analysis of such data to facilitate evidence based reform rather than being driven by stakeholders’ interest only. The pre reform decentralized kerosene procurement at the district level failed due to poor management at district level. The reform attempts to centralize financial accountability and regionalize procurement of kerosene failed because of the opposition from stakeholders and flaws in the distribution structure. The stakeholders used the shortcomings in the kerosene procurement reform plans and implementation to reverse reforms in kerosene procurement. During the period of planning for the changes in kerosene distribution, districts went without kerosene for the cold chain. Thus the opposition resulted in reduced kerosene availability at the affected areas consequently. Plans to integrate EPI functions were promoted by DANIDA since early 1990s as one of the major external stakeholder (17). When the HSR started, it offered a good opportunity to implement the integration of some of the EPI functions into MSD operations. However, despite the willingness and desire on the part of the donors, MSD seemed not to have taken sufficient steps to prepare for the new task. In the retrospect among the preparations and planning that would have been helpful would have been a study of EPI operations, and development of strategies to involve all stakeholders in the health reform process. MSD and allies would have benefited from a mapping of all stakeholders, their interests and levels of support. Such precautions have been shown elsewhere to facilitate the design of appropriate interventions that improved the reform process (18-19). Before the implementation of the health sector reforms a state of equilibrium existed around the EPI delivery system as a result of acceptance of the arrangements that existed. The reforms altered the equilibrium making the stakeholders react some with intentions of maintaining status quo while others supporting the changes. Positive progress in the EPI reforms as any other policy process depended highly on the power of the supporters overriding those in opposition(20). When planning for reforms it was then important to understand which stakeholders would support and which would oppose the changes and important contexts. Thus the planning would take into consideration such information and assume strategies that will increase the likelihood of success for the EPI reforms. The influence of stakeholders in the EPI program were complimentary i.e donors provided most finances, government provided most administration at central level, DCCOs and DMCHCOs provided most administration in the districts and communities were the primary beneficiaries. The influences though differed were complimentary to achieve the EPI goals. Despite complimentary influence the underlying interest of some stakeholders did not follow the respective influence. The underlying objective of the DCCOs DMCHCOs was financial gain while the petroleum company was to make profit and MSD was business efficiency. Such nonalignment in stakeholders primary interest in reforms have been observed elsewhere with negative impacts (21). Hence then stakeholder analysis at the planning stage should be deep enough to understand also undeclared interests. Health systems in developing countries have been experiencing poor financing leading to poorly paid workers. In compensation, health workers had been seeking alternative incomes from various sources, which could compromise the quality of their services (13, 22-23). For example MoH employees attached to EPI were sure of predictable supplementary income from EPI travel allowances, command of transport and other benefits offered by EPI. Such workers could easily join forces to oppose reforms abolishing or decreasing such supplementary income. The analysis also revealed that EPI coverage started to fall about four years before the EPI reforms and the amount of vaccine per capita distributed to regions did not change significantly over the period of reforms. This suggests that the reforms had no significant direct effect on the EPI coverage. Certain stakeholders made use of an already existing gradual decline in EPI coverage to oppose the reforms to justify status quo. After reversing of some of the reforms in 2000, regions that had closed their RVS received significantly lower doses of measles vaccine per capita compared to the rest of the country suggesting regional level management problems. Also at global level EPI coverage had been observed to be falling since early 1990s(24). This further supports that proper analysis of the EPI services was not done or else it was to camouflage a primary interest of the stakeholders in order to oppose the reforms. Camouflaging a primary interest is also supported by an analysis of health sector reforms and new public management agenda which observed that the agenda was blocked by existing state institutions and vested interests which were suspicious of the reforms(25). Thus lack of proper analysis and vested interests jointly explains the opposition to reforms. It took more than one year since decision to reverse the closure of RVS to when the reversal was effected. The time was used in exchanging communications between the Ministry and MSD. The communications concerned unavailability of information to MSD and need of evidence to justify the claims. However it could be construed that it was a way of a stakeholder to resist reforms in order to protect vested interests. Stakeholders’ opposition thus manifested as a process to justify status quo, which required time for the reform manager to respond and reach a compromise. In response to the stakeholders’ reaction the EPI service provision was limited until an understanding was reached. The need to understand the role of stakeholders in policy process and its management has been stressed(26-27). One could have made use of existing opportunities to facilitate the communications such as establishing regular consultative meetings with relevant stakeholders, which would also facilitate their participation(28). Such strategies to enhance communication between MSD and MoH are now in the process of being setup. EPI delivery system generated several types of management information at all levels. Among the analysis done was the percentage of children vaccinated against the expected. The other data generated was not analyzed routinely. Asking appropriate questions on program performance followed by proper analysis of relevant data should provide important management information for the program. Thus there should be more analysis of data to understand the different aspects of program performance and hence making the reforms evidence based. The role of information from routine sources and research to facilitate evidence-based reform of the health sector has been stressed at various places(29-32). Had there been appropriate analysis it could have been easy to understand some of the claims that EPI performed poorly due to the reforms were baseless. Conclusions Changes of policy like the integration of EPI functions into the MSD operations or the centralization of kerosene procurement should be anticipated to generate positive as well as negative reactions among stakeholders. The reforms centralizing the procurement and distribution of cold chain kerosene brought aboard new stakeholders and changed the positions of some of the old ones. These changes provoked negative reactions from some stakeholders, and brought the reforming process to a stand still, and in some cases reversal of the reforms by the experiences from elsewhere, these negative reactions could have been forecasted, and appropriate precautions instituted. The petroleum company awarded the contract to distribute the cold chain kerosene to the districts was not studied its capacity and efficiency for undertaking the assignment. The recommendations for future reforms are therefore that:
This analysis was focused at national level; it demonstrated how donors and the government supported reforms in the EPI program. The regional and district providers (RCCOs, RMCHCO, DCCOs, and DMCHCOs) agued and reversed the reforms. Underlying the argument that reforms were reducing coverage was their personal gains. These arguments were not supported by analysis of vaccine availability. District level health staffs would be the implementers of the EPI reforms within the decentralized health services in the local governments. Next paper presents an analysis of the immediate response to EPI reforms and decentralization at district level References
© Copyright 2004 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp04006t2.jpg] [lp04006f1.jpg] [lp04006t4.jpg] [lp04006f4.jpg] [lp04006f2.jpg] [lp04006f3.jpg] [lp04006t3.jpg] [lp04006t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}