 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 1, No. 1, Oct, 2004, pp. 41-46 AIDS Knowledge and Risk Perception in Urban and Rural Communities in Arusha Region, Tanzania 1Knut-Inge Klepp, 2Kagoma S. Mnyika, 3Naphtal Ole-Kingóri, 4Melkizedeck T. Leshabari and 3Peter E. Kissila 1From the University of Olso, Norway, 2Dept. of Epidemiology
and Biostatistics, Muhimbili University College of Health Sciences, Dar es
Salaam, 3Mount Meru Hospital, Arusha, Tanzania, 4Dept. of
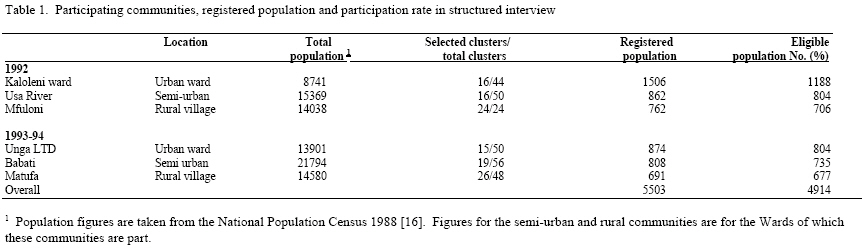
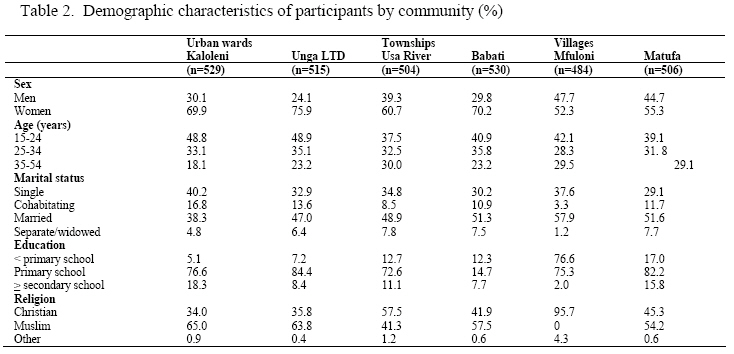
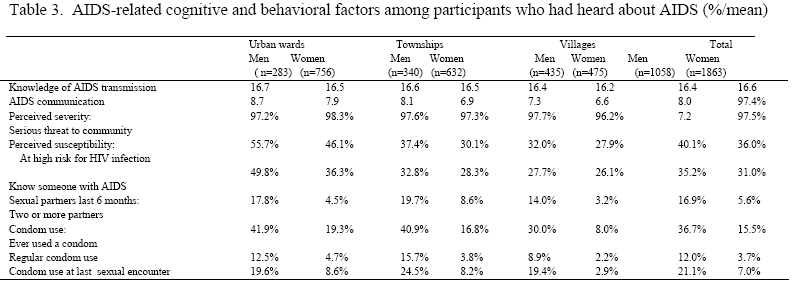
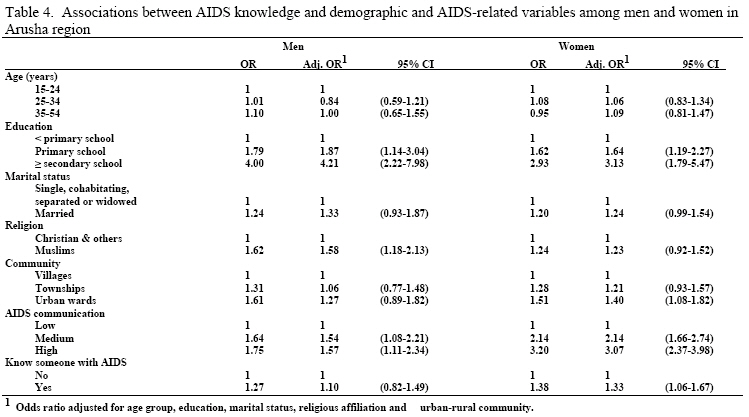
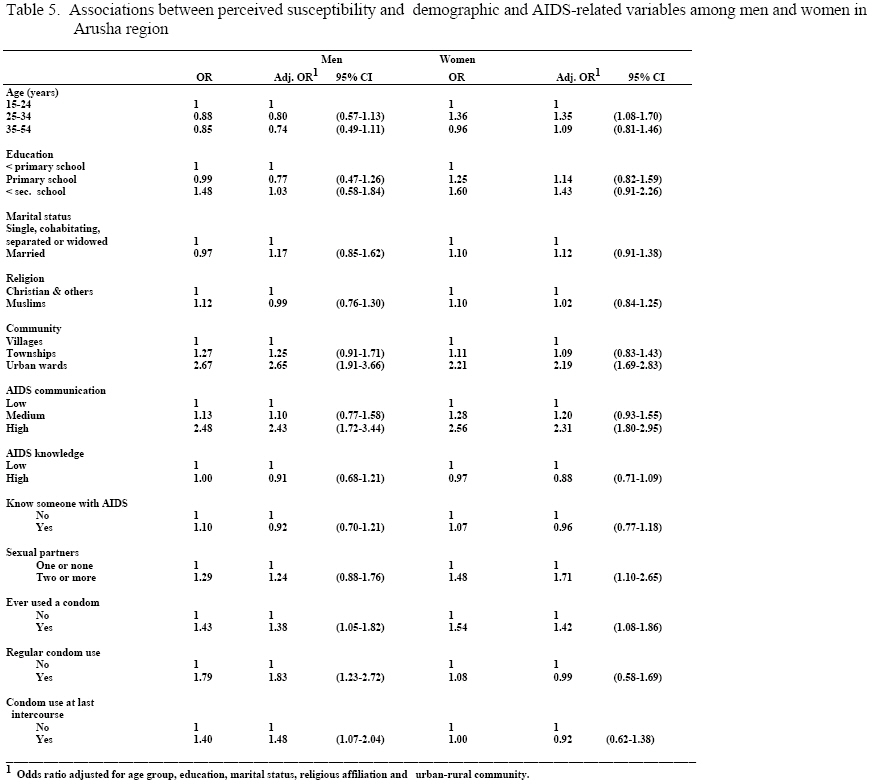
Behavioural Sciences, Muhimbili University College of Health Sciences Code Number: lp04007 Abstract The purpose of this study was to investigate demographic, cognitive and behavioral factors associated with levels of AIDS knowledge and perceived susceptibility to HIV. Cross-sectional, population-based surveys were conducted in two urban communities, two townships and two rural villages in Arusha region, Tanzania. Eligible participants were 15 to 54 years old living in randomly selected household clusters. A total of 3068 of the eligible men and women participated (62%). The large majority of participants from all six communities had heard of AIDS (96%) and perceived AIDS to be a serious threat to their community (97%). Both men and women had high levels of AIDS knowledge (67% answered at least 17 out of 18 questions correctly). Men reported to discuss AIDS more frequently than did women, and they perceived themselves as being at high risk for HIV infection more often than did women. For both men and women, having higher education and reporting having frequently discussed AIDS were significantly associated with a high score on the AIDS knowledge scale. Living in an urban community, frequently discussing AIDS and previous sexu al behavior were significantly associated with perceived susceptibility for HIV infection among both men and women. It is recommended that future educational efforts focus on creating opportunities for people to discuss HIV/AIDS in safe and supporting environments. Introduction S sexual intercourse is the primary mode of sexual behaviors is a major strategy of primary HIV transmission in sub-Saharan Africa, changing high risk prevention efforts (1). According to a number of behavior change theories, prior to changing high risk behaviors, a person needs to recognize that these behaviors are putting him/her at increased risk and that this risk can be reduced by modifying the behaviors (2-5). In their three-stage AIDS Risk Reduction Model (ARRM), Catania and his colleagues (4) suggest that people first have to label their own high risk behaviors as problematic. Knowledge of high risk sexual activities, feeling personally susceptible to contracting HIV, and seeing AIDS as a serious and undesirable disease are three factors hypothesized to influence labeling one’s own sexual behaviors as problematic (4). In reviewing research that investigates the correlates of AIDS knowledge in samples of the general population in developed countries, Peruga and Celentano (6) concluded that being highly educated, young and white increased the chances of being knowledgeable about AIDS. Furthermore, a relationship seems to exist between strong religious beliefs or conservative political convictions and low AIDS knowledge, while other social or demographic variables appear to have little effect on AIDS knowledge (6). While a number of surveys of AIDS knowledge have been conducted in sub-Saharan Africa (7), few have investigated the relationship between knowledge, risk susceptibility and other social and demographic factors. In a large study conducted in 1988 among a random sample of 20 to 49 year old men and women in Kinshasa, Democratic Republic of Congo (formerly Zaire), 17% of the men and 16% of the women perceived themselves to be at very high or moderate risk of getting AIDS (8). A significant proportion of the participants held serious misconceptions regarding the existence of an AIDS vaccine and cure (8). Applying ARRM in an African setting, Bertrand and colleagues (9) found that women in Bas-Zaire had heard of AIDS, but that their AIDS knowledge appeared to be superficial. A third of the women believed themselves to be at risk of getting AIDS (9). A study among child-bearing urban Rwandan women, also applying ARRM, found that as many as 57% perceived themselves to be at risk of AIDS (10). Perception of risk was associated with reported behavior change the previous year and with higher prevalence of HIV infection (10). Tanzania is one of the sub-Saharan African countries that has reported the most AIDS cases (11). In a nationwide survey of 15 to 49 year old Tanzanians, 32% of participating men and 14% of the women reported one or more non-regular sexual partners in the last 12 months (12). Furthermore, a substantial proportion of men (25%) and women (11%), reported having involvemd themselves in commercial sex during the last 12 months. In 1989, 65% of the participants in a small follow-up study to a population-based HIV/syphilis prevalence survey perceived themselves to be at risk of getting AIDS (13). No published reports of AIDS-related knowledge and perceived susceptibility of AIDS and their correlates in the general adult population are available from Tanzania. Arusha region, located in northern Tanzania, has seen a rapid increase in the HIV prevalence rate since 1986 (14). The HIV seroprevalence rates among 15 to 54 year olds have been found to differ according to sex, socio-economic status in the urban areas, and between urban and rural communities throughout the region (higher rates for women, low socio-economic and urban areas) (15). In this paper, we present the levels of AIDS knowledge, perceived susceptibility and perceived risk to HIV infection seen in population-based samples of 15 to 54 year olds from Arusha region in 1992-1994. Demographic and AIDS-related cognitive and behavioral factors associated with AIDS knowledge and perceived risk are presented. Furthermore, sex and urban–rural differences are examined. Methods Subjects and survey procedures: The Arusha region has an estimated population of approximately 1.3 million (16). It is divided into eight districts, and each district is made up of a number of administrative units called wards. Each ward has clusters of 10-cell household units under the leadership of a 10-cell leader. For this study, six communities were selected to represent the different urban, semi-urban and rural settings in Arusha region: two urban wards within Arusha town, two townships located along major roads (semi-urban), and two rural villages (Table 1). Clusters of 10-cell households were randomly selected from each community. All adults (15 to 54 years of age) living in households within the selected 10-cells were registered and invited to participate in the study. A trained field-team visited the target population at home and sought informed consent for participation in a structured interview. At the end of the interview, participants received educational materials pertaining to AIDS and potential misconceptions regarding HIV/AIDS were addressed. Following the interview, the interviewer sought informed consent for HIV-testing (15). This report is based on data from the structured interview only. Structured interview The interview consisted of 65 pre-coded questions and 15 open-ended questions adapted from the World Health Organization/Global Programme on AIDS's survey of knowledge, attitudes, beliefs and practices (KABP) (17). Prior to the study presented here, this questionnaire was pilot-tested (18). Each interview lasted approximately 25 minutes and included questions relating to socio-demographic characteristics such as gender, age, marital status, formal education and religious affiliation. The response categories and distribution by participating community is presented in Table 2. Participants were asked whether they had ever heard of a disease called AIDS (AIDS awareness; response categories: yes/no), and whether they had ever known anyone with AIDS (Knowing someone with AIDS; response categories: yes/no). HIV/AIDS knowledge was assessed by 18 questions concerning HIV transmission routes and potential misconceptions regarding casual contact. A sum score, range 0-18, in which 18 indicated correct answers to all questions, was created (Cronbach alpha=0.74). The overall mean score for the AIDS knowledge scale was 16.5 ± 2.1, and prior to investigating its relationship to other demographic and AIDS-related variables, it was recoded to ‘high’ (>16 correct answers) versus ‘low’ (≤16). Four items assessing how frequently participants were discussing AIDS with family members, friends, neighbors and spouses/regular sexual partners were combined to form a scale, range 1-13, where a high score indicated frequent discussions about AIDS (Cronbach alpha=0.92). This scale, AIDS communication, had an overall mean of 7.5 ± 4.5 and has been recoded to ‘low’ (score of 1.0-4.9), ‘medium’ (5.0-9.9) and ‘high’ (≥10) score. Perceived susceptibility to AIDS was assessed by asking participants how likely it was that they were infected by the AIDS virus (1=not at all likely; 5=chances are very high) which has been recoded to ‘high’ (very high or somewhat high risk) and ‘low’ risk. Perceived severity was assessed by asking how serious a threat AIDS was to their community (1=no threat; 4=serious threat). This variable has been recoded to ‘serious threat’ and ‘not a serious threat.’ Self-reported sexual behavior included number of different sexual partners within the past six months (recoded to ≥2 versus ≤ 1 partners), whether they had ever used a condom (yes/no), regular condom use (often use condoms versus never or infrequent use) and condom use at last sexual encounter (yes/no). Data analysis: Analysis of variance and logistic regression analysis were conducted on SPSS-PC (Version 10.1), and estimates were adjusted for age-group, education, marital status, religious affiliation and urban–rural location. The increase seen in the standard error due to the clustered sample design (10-cells) was small (5-15%), and adjusting for this increased variance did not significantly change the results. Thus, the unadjusted estimates are presented in this report. Results A total of 5503 people aged 15 to 54 were registered as living in the selected 10-cell clusters prior to the study. At the time of the study, we found that one person had died, while 588 had moved or were attending boarding schools elsewhere. These subjects (12.3% of the registered men and 9.3% of the women; age 24.3 years; 95% CI: 23.5-25.1) were excluded from the study. Of the 4914 eligible subjects, a total of 3068 participated in the structured interview (overall participation rate 62.4%). The refusal rate was 3.9% (n=191), 22.5% (n=1105) of the subjects could not be reached at home on repeated visits due to work commitments, while we have no information regarding reason for non-participation for 11.2% (n=550) of the eligible subjects. Participation rate by community is presented in Table 1. A larger proportion of eligible women than men participated in the structured interview (73.9% vs. 48.8%; p<0.00001), and participants were on the average younger than non-participants (28.1 years (95% CI: 27.8-28.5) compared to 30.9 years (95% CI: 30.4-31.3). Participants from the six selected communities differed in terms of their demographic characteristics (Table 2). We were primarily interested in the urban–rural differences, and comparing the three sets of community-pairs, we found that the urban communities had a higher proportion of women (χ2(2)=81.5; p<0.00001), younger participants (χ2(4)=51.3; p<0.00001), participants with higher formal education (χ2(4)=94.8; p<0.00001), and fewer married subjects (χ2(6)=55.8; p<0.00001), than did the rural communities. The reported religious affiliation differed as much within each pair of communities as it differed across the urban–rural communities (Table 2). The following analyses have been adjusted for the differences in demographic make-up between the urban–rural communities. The large majority of participants from all six communities reported having heard of AIDS (95.6%), with more subjects from the urban areas than from the townships or rural villages having heard of AIDS (99.5%, 94.4% and 92.6% respectively; F=25.3, p<0.001). Participants who had not heard of AIDS (n=136) were not asked any further AIDS-related questions, and are therefore excluded from the following analyses. Across urban–rural communities, we found both men and women to have high levels of knowledge regarding AIDS (67% gave a correct answer to at least 17 out of the 18 questions). However, men reported having discussed AIDS more frequently than did women (F=12.3; p<0.001), and they perceived themselves as being at high risk for HIV infection more often than did women (F=11.4; p<0.001) (Table 3). Furthermore, men more often than women, reported having had two or more sexual partners during the past six months (F=82.2; p<0.001), ever having used a condom (F=162.3; p<0.001), regularly using condoms (F=65.6; p<0.001) and having used a condom at the last sexual encounter (F=103.8; p<0.001). Adjusting for gender (as well as the other demographic factors), we found urban participants to be more likely to report frequently discussing AIDS than were rural participants (F=25.2; p<0.001). The large majority (97%) perceived AIDS to be a serious threat to their own community, but urban participants were more likely to see themselves at risk for HIV infection compared to rural participants (F=46.1; p<0.001), and they more often knew someone with AIDS (F=26.6; p<0.001). Rural participants reported less often having had two or more sexual partners (F=8.2; p<0.001), ever having used a condom (F=12.2; p<0.001), regularly using condoms (F=4.4; p<0.01) and having used a condom at the last sexual encounter (F=4.1; p<0.02) than did participants from the urban or semi–urban communities (Table 3). In Table 4, the associations between AIDS knowledge and the demographic and AIDS-related predictor variables are presented. For both men and women, having higher education and reporting having frequently discussed AIDS were significantly associated with a high score on the AIDS knowledge scale. In addition, Muslim men scored higher than other men, while for women, living in Arusha town and knowing someone with AIDS were significantly associated with a high knowledge score. Similarly, as seen in Table 5, living in Arusha town and frequently discussing AIDS were significantly associated with perceived susceptibility for HIV infection among both men and women. Previous sexual behavior was also associated with increased perceived risk for HIV infection. For men, condom use was, significantly and consistently across measures, associated with perceived susceptibility, while for women, having had two or more sexual partners during the past six months and ever having used a condom was significantly associated with perceived susceptibility. In addition, women 25 to 34 years old perceived themselves to be at higher risk than did younger or older women (Table 5). Discussion The results from this study demonstrate that most adults in Arusha region by 1992-94 had heard of AIDS, perceived it to be a major threat to their community, knew the main HIV transmission routes, and also knew the ways in which the virus is not transmitted to others (casual contact). Furthermore, most of the participants knew that there is no successful cure for AIDS. Consistent with research finding from surveys conducted in developed countries (6), we found that level of education was a strong predictor of AIDS knowledge, as was reported frequency of discussing HIV/AIDS with friends, neighbors, relatives and spouses/regular sexual partners. In Tanzania, where relatively few have access to mass media such as television and newspapers, personal communication is an important way of disseminating information. It is therefore encouraging that frequent personal communication about AIDS is associated with increased levels of knowledge, indicating that factual information rather than myths and misconceptions are being communicated. A number of religious organizations have been active in providing information regarding HIV/AIDS. The fact that men classifying themselves as Muslims scored higher on the knowledge score than did other men might reflect differences in the educational efforts between local mosques and churches. A similar, but non-significant trend was also observed for women even when adjusting for other demographic factors which might differ between these groups, including educational level and geographical location. For women, knowing someone with AIDS was associated with increased levels of AIDS knowledge. As AIDS patients are cared for at home by women, women who know people with AIDS are probably more likely to seek out information on HIV/AIDS. Perceived susceptibility to the HIV virus did reflect local differences in the HIV-prevalence as participants from the urban areas and, for women, those 25 to 34 years of age, perceived themselves to be at higher risk than did other participants. Those reporting frequent discussion of HIV/AIDS with others did perceive themselves to be susceptible to the virus, while AIDS knowledge was not associated with reported risk perceptions. Reported condom use, which may be seen as an indicator of involvement in sexual risk behaviors (having multiple or non-regular sexual partners) (15), and those with multiple partners correctly perceived themselves at higher risk than others. This indicates that in this population, where the level of AIDS knowledge was high, it is labeling one’s own behavior as risky and information about the local HIV/AIDS epidemic, rather than information about the virus, its transmission routes or the disease itself which might impact people’s sense of susceptibility. Interestingly, personally knowing someone with AIDS did not increase people’s perception of their own vulnerability. Thus, the participants might not identify themselves with the AIDS patients they know, and they are likely to attribute different risk estimates to themselves compared to those of people with AIDS. This study has several limitations. Attrition rates were high, particularly among men. While we did observe that participating men reported higher levels of risk behaviors than did women, these differences might be underestimated by the lower participation rates among men. Also, participating men might have more knowledge regarding AIDS and discuss AIDS-related issues more frequently than non-participating men in these communities. In general, we suspect that perceived risk behaviors might be somewhat underreported in this population of participants who are highly aware and knowledgeable regarding HIV transmission and AIDS. It is difficult to compare the reported levels of risk behaviors in this study to that reported in other studies due to differences in methodology. For example, while 17% of men and 6% of women reported more than one sexual partner during the past six months in this study, 32% of the men and 14% of the women reported at least one non-regular sexual partner in the last 12 months in the National Sexual Behavior Study (12). We do not know what proportion of participants reporting only one partner in our study actually had a non-regular partner, or to what extent people who reported two partners actually were referring to two spouses. Furthermore, the difference in time frame (6 versus 12 months) makes it difficult to compare rates between these studies. Finally, as this is a cross-sectional survey, we are not able to determine the temporal or causal relationship between the cognitive and behavioral factors reported in this study. In spite of these limitations, we believe the results from this study provide important information that has implications for future HIV/AIDS education in this region. As people are aware of AIDS and HIV transmission routes, there is a need to move from general information campaigns to more in-depth educational efforts empowering people to identify their own risk behaviors and learning skills for how to reduce their vulnerability. Also, making people aware of the rapid spread of the HIV virus throughout the region over the last decade might be important to help them make more accurate risk estimates. Creating opportunities for people to discuss HIV/AIDS in safe and supporting environments seems important since communication was such a strong predictor of perceived susceptibility. Such settings (schools, non-governmental organizations, local women/youth groups, health facilities and work-sites including market places) offer opportunities for changing the image of condom use, skills-building relating to negotiation of condom use, as well as information regarding prevention and treatment of other sexually transmitted diseases. The feasibility and potential effectiveness of such an approach in primary schools (19), women’s groups (20), bar workers (21), and on a local community level (22) has already been demonstrated. To help people move beyond phase I of ARRM (labeling your own behavior as putting you at risk) to personal commitment and actual behavior change (4), there is a strong need to further develop such strategies for use in other settings and to vigorously pursue them on a larger scale. Acknowledgment This work was funded by a grant from the Norwegian Agency for Development Cooperation (NORAD) and by the Tanzanian Ministry of Health through the Tanzanian - Norwegian AIDS Project (MUTAN). References
© Copyright 2004 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp04007t5.jpg] [lp04007t4.jpg] [lp04007t3.jpg] [lp04007t2.jpg] [lp04007t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}