 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 2, No. 1, April, 2005, pp. 1-5 Associations of Cement Dust with Occurrence of Respiratory Conditions and Lung Function Seter Siziya Correspondence to: Seter Siziya, Department of Community Medicine, School of Medicine, University of Zambia, P.O. Box 50110, Lusaka, Zambia Code Number: lp05001 Abstract Objective: To determine associations between cement dust on one
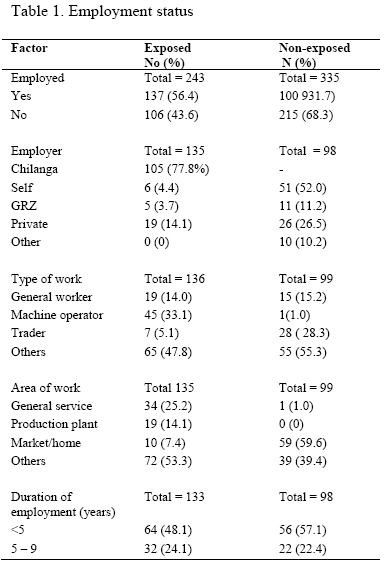
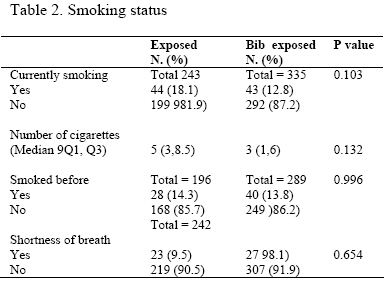
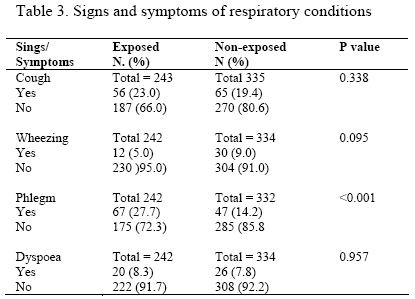
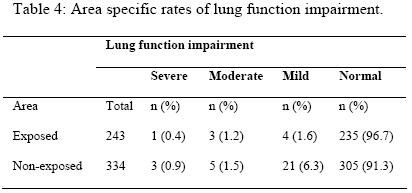
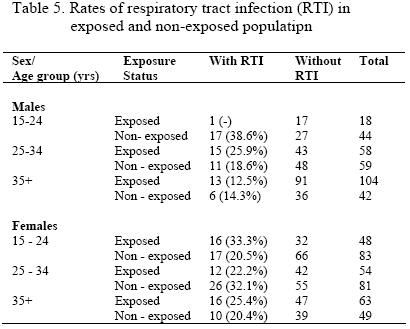
hand and occurrence of respiratory conditions and lung function on the other. Key words: cement dust, respiratory conditions Introduction There were reports that the air pollution from the Chilanga cement factory had adversely affected the inhabitants of the township. UNEP/EEU (1) reported that respiratory complaints among the locals were higher than national averages. However, there were no figures to support this statement. Concerns in the press suggested that persons living within the vicinity of the factory could have suffered from respiratory conditions because of the cement dust emitted from the factory. There is conflicting evidence in the literature on the association of cement dust and respiratory conditions. For example, while Abrons et al (2) found no significant difference in the rates of phlegm between cement workers and controls, Al-Neaimi et al (3) reported a higher percentage of phlegm among the exposed workers (25%) than among the unexposed (5%). Futhermore, Abrons et al (2) found similar prevalence rates of wheezing between cement workers and their controls. Contrary, Al-Neaimi et al (3) found a higher percentage of exposed workers reporting wheezing (8%) than unexposed workers (3%). This difference was not due to low power of the study in the Abrons’ study, (2) which recruited 2736 cement workers and 755 controls. Current information also suggests that there is inconsistent evidence in the association of exposure to cement dust and lung function. The following are some of the studies that found no association between lung function and exposure to cement dust. Izycki et al (4) found mean values of dynamic spirographic indices not to differ significantly from those of the controls. A similar finding was reported by Abrons et al. (2). In a cross-sectional epidemiological survey of a selected group of former and present cement factory workers and a random sample of the corresponding urban population, no significant differences in lung function between cement factory workers and other blue collar workers were observed (5). AbuDhaise et al. (6) in a cross-sectional survey of cement workers in Jordan, concluded that inhalation of cement dust irritates the respiratory tree without markedly affecting lung function. Contrary to the above findings, the following are some of the studies that found an association between lung function and exposure to cement dust. In Malaysia, the workers showed significantly lower FEV1% and FEF25-75%, and higher FMFT than the controls (7). Al-Neaimi et al. (3) in the United Arab Emirates found that ventilatory function (VC, FVC, FEV1, FEV1/VC, FEV1/FVC and PEF) was significantly lower in the exposed workers compared with unexposed workers. The authors concluded that decreased ventilatory function probably was caused by exposure to cement dust. Workers exposed to cement dust in Nigeria had significantly lower lung function compared with nonindustrially exposed population (8). In Taiwan, Yang et al (9) found that the exposed group had a significantly lower mean FVC, FEV1, FEF50-75 than the control group. Because of conflicting evidence on the health effects of cement dust, and that no studies had been done on the effect of cement dust on the health of the inhabitants in Zambia, the current study was conducted in order to determine associations between cement dust on one hand and occurrence of respiratory conditions and lung function on the other. Methodology Study areas The study was conducted in two residential areas: Chilanga (exposed population to cement dust) and Chelstone (unexposed population). Chilanga is 25 km south of Lusaka on 15.39oS latitude and 28.19oE longitude. Meanwhile, Chelstone is 15 km east of Lusaka. The Chilanga cement company was founded in 1949 by the Government of Northern Rhodesia and the Colonial (now Commonwealth) Development Corporation. The company had two plants: one in Chilanga and the other in Ndola, which is about 400 km to the north of Lusaka. The plant in Chilanga produced more cement than the one in Ndola. Study design The basic study design was cross sectional and review of clinic records. Data collection Clinic records: Daily attendance records for the months of January, July and October in 2002 in the cement factory clinic and control clinic were reviewed in order to determine rates of respiratory conditions. Questionnaire: A structured questionnaire was used to obtain information on socio-demographic characteristics, employment status, smoking status, signs and symptoms of respiratory conditions, and health status relating to asthma, bronchitis and sinusitis. Spirometry: Lung function was determined using a spirometer, Spirobank-G. Sample size and Sampling Survey: We did not have reliable information on the prevalence of respiratory conditions nor the population size that we could have used to determine the sample size. Hence, an optimum sample size was determined by considering a prevalence of 50+5%, which gave a sample size of 384. We considered enrolling 400 subjects (200 males and 200 females) in each residential area. All workers in the cement plant that were present during the time of collecting data were asked to participate in the study. Workers who were off duty at that time were followed up in their homes. Female participants residing closest to the cement factory were sampled using a 1 in 2 systematic random sampling technique. A household was the sampling unit. The oldest female present at the time the research team visited the household was recruited into the study. In the control area, a 1 in 2 systematic random sampling technique was also used to select participants living closest to the clinic. The oldest male and female present when the research team visited the household was asked to participate in the study. Clinic audit In the exposed area, 345 records were selected from the clinic register using a 1 in 8 systematic random sampling technique. Male dependants and female employees were excluded because they were few. Meanwhile, all cases totaling 358 with reported diagnosis in the control clinic register were sampled. Inclusion criteria Spirometry requires a cooperative participant. An individual must take in a deep breath and then blow all the air out quickly and forcefully. Because young children and old subjects may not be cooperative, only individuals of age between 15 and 59 years inclusive were asked to participate in the study. Furthermore individuals must have stayed in the study area for at least two years. Data processing and analysis Completeness of the questionnaires was checked while in the field. Data was entered in a computer using Epi Info. Data was edited using range and consistency checks as well as validation of the duplicate files. FEV1/FVC% was categorized as follows: <40=Severe, 40-54=Moderate, 55-70=Mild, >70=Normal. In the logistic regression, categories Mild to Severe were classified as impaired lung function. Preliminary analysis involving bivariate analysis (the Yates’ corrected Chi-squared test for association of two qualitative variables, and the t-test or Kruskal-Wallis (H) test for two independent samples for continuous factors) was conducted in Epi Info. The stepwise logistic regression in SPSS was used to determine independent predictors of the outcome. Odds ratios and their 95% confidence intervals were used to estimate the magnitude of associations. The cut off point for statistical significance was set at 5%. Ethical consideration The project was approved by the Ethical Committee of the University of Zambia (Assurance No. FWA00000338, IRB00001131 of IOR G0000774). Further approval was given by the Chilanga Cement Plc management and the Director of the Lusaka Urban District Management Team. Finally, permission was sought from the individual participants to enter the study. Participants were not forced to enter the study and were free to dropout at any stage of the study. No individual person was identified by name. Results In total 105 cement workers and 138 females exposed to cement dust were recruited into the study. Three workers refused to participate in the study. Meanwhile, 172 males and 163 females were recruited from the control area. Socio-demographic characteristics Out of the 243 participants exposed to cement dust, the sex of one participant was not recorded. There were 127 (52.5%) males and 115 females in the exposed group, compared to 172 (51.3%) males and 163 females in control group (p=0.853). On average, exposed persons were older than those in the control group (Median (Q1, Q3) age for exposed persons was 33 (25, 40) years compared to that for persons in the control area of 26 (21, 34) years, p<0.001). The duration of stay in the areas was similar in both exposed and non-exposed areas [Median (Q1, Q3) years were 10 (5, 16) for exposed and 9 (5, 15) for control areas, p=0.058). Employment status Table 1 shows the employment status of the respondents. Significantly more respondents were employed in the exposed area compared to those in the control area (p<0.001). About half (48.1%) of the exposed employees had been in employment for less than five years. Meanwhile, 56 (57.1%) of the non-exposed employees had been in employment for less than five years. Smoking status The proportions of persons who smoked and the number of cigarettes smoked between the exposed and non-exposed groups were similar as shown in table 2. Asthma Six (2.5%) of the 242 exposed persons were asthmatic, compared to 13 (3.9%) of the 333 non-exposed individuals (p=0.479). Bronchitis and sinusitis Four (1.6%) of the 243 exposed individuals had bronchitis in the previous two weeks compared to seven (2.1%) of the 335 controls (p=0.768). As regards to sinusitis, 5.8% of the 225 exposed persons and 9.9% of the controls had sinusitis in the previous two weeks (p=0.113). Signs and symptoms of respiratory conditions Cough, wheezing, dyspnoea and shortness of breath were equally prevalent in both exposed and non-exposed groups. Phlegm (p<0.001) was more prevalent in the exposed (27.7%) than in the control (14.2%) group, as shown in table 3. Area specific rates of lung function impairment Table 4 shows the distribution of lung function impairment between the study areas. Overall impairment was more prevalent in the non-exposed (8.7%) than in the exposed (3.3%) group (p=0.015). Associations of cement dust with phlegm or lung function Confounding factors in the relationships between cement dust and phlegm were length of stay in the area, age, sex, height and smoking status. Upon considering these confounding factors in a logistic regression, exposed persons were 2.24 (95%CI 1.46, 3.44) times more likely to have had phlegm in the previous two weeks before the study compared to non-exposed individuals. Sex was the only confounding factor that remained in the model for lung function impairment. Males were 3.45 (95%CI 1.53, 7.77) times more likely to have had impaired lung function than females. Exposed individuals were 62% less likely to have had impaired lung function than non-exposed persons (OR=0.38, 95%CI 0.17, 0.86). Clinic data Evidence from the clinic records (Table 5) suggests that there was no association between cement dust exposure and respiratory tract infection. After stratifying for age, exposed male employees were equally likely to have reported to the clinic for respiratory tract infection compared to their male controls [Mantel-Haenszel (M-H) weighted odds ratio = 0.79, 95%CI 0.42 to 1.48]. Similarly, exposed females were equally likely to have reported to the clinic for respiratory tract infection compared to their female controls [M-H = 1.13, 95%CI 0.69 to 1.86]. Discussion This is the first study to be conducted in Zambia on health effects of exposure to cement dust. The findings in the current study will be useful in the design of similar future studies in Zambia. In the present study, no significant associations were observed between cement dust exposure on one hand and asthma, sinusitis, bronchitis, shortness of breath, cough, dyspnoea nor wheezing on the other. A similar result was reported by Abrons et al (2) who found similar prevalence rates of wheezing between cement workers and their controls. These findings contradict the results reported by Al-Neaimi et al (3) who found higher percentages among exposed persons than controls of bronchial asthma (6% against 3%), sinusitis (27% against 11%), bronchitis (13% against4%), shortness of breath (8% against 4%), recurrent and prolonged cough (30% against 10%), dyspnoea (21% against 5%), and wheezing (8% against 3%) respectively. In another study, Izycki et al (4) found 17% of cement plant workers and 10% of controls to have chronic bronchitis. The inconsistency results on the association of cement dust and respiratory conditions remain unresolved. The finding by Al-Neaimi et al (3) who reported a higher percentage of phlegm among the exposed workers (25%) than among the unexposed (5%) concurs with the result in the current study in which exposed persons (27.7%) had a higher rate of phlegm than non-exposed persons (14.2%). However, both results differ from the result of Abrons et al, (2) who found no significant difference in the rates of phlegm between cement workers and controls. The difference in findings may not have been as a result of low study power because the sample sizes in the study by Abrons et al (2) were very large. The results may not be consistent in different study areas because of different dust control measures that may be in use in these areas. Although, age was reported to be associated with lung function (6, 10-12), it was not a confounder in the current study in the relationship between cement dust and lung function. Meanwhile, the result that male respondents in the present study were more likely to have impaired lung function than females, contradicts the finding of Alakija et al (11) who reported that FEV1, FVC and PEFR were higher in males than females. The fact that most female respondents in our study were less exposed than males because most females did not work in the cement factory, may explain the apparent contradiction between the study results. Studies have shown that the lung function of the cement workers decreased with the duration of employment (8, 11), smoking status (6, 13) and that the prevalence of chronic phlegm (2) increased with duration of work in exposure to cement dust. These factors did not confound the relationship between cement dust and lung function impairment in the current study. The finding in the current study may partly be due to most respondents being non-smokers and having had a short period of exposure to cement dust. In conclusion, the inconsistency findings in the current study that the proportion of lung function impairment among non-exposed participants was higher than among exposed individuals, and that rates of phlegm were higher among exposed persons than non-exposed persons suggest that cement dust may not have been associated with the impairment. Acknowledgments We would like to thank our research assistants for working tirelessly. To the respondents we say thank you for your cooperation. We are grateful to the Management of Chilanga cement company and the Lusaka Urban District Management Board for permission to conduct the study. We acknowledge with thanks the British Council for funding the study. References
© Copyright 2005 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp05001t5.jpg] [lp05001t4.jpg] [lp05001t3.jpg] [lp05001t1.jpg] [lp05001t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}