 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
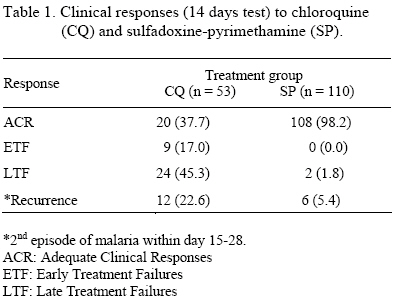
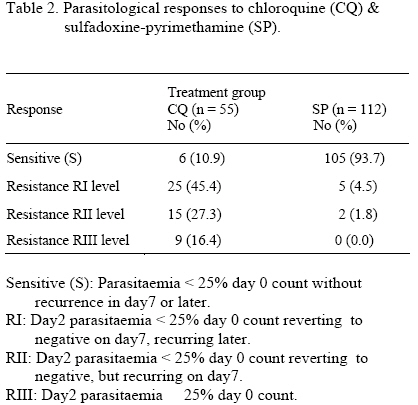
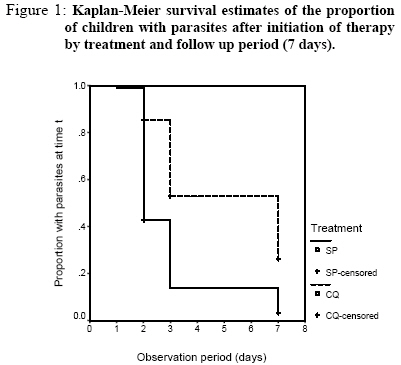
East African Journal of Public Heath, Vol. 2, No. 1, April, 2005, pp. 13-16 Sulfadoxine-Pyrimethamine for the Treatment of Falciparum Malaria in Tanzanian Children and Implications for Policy Change DS Tarimo Correspondence to: DS.Tarimo, P.O.Box 65217 Dar es Salaam, Tanzania, Muhimbili University College of Health Sciences, Department of Parasitology & Medical Entomology, Institute of Public Health, Code Number: lp05004 Abstract A trial of SP versus CQ was carried out in a holoendemic area as part of the antimalarial drugs efficacy monitoring in Tanzania prior to policy change from chloroquine (CQ) to sulfadoxine-pyrimethamine (SP). The aim was to obtain comparable data as reports from one holoendemic area had shown an SP resistance > 25% past the level for change. Therefore using the WHO in vivo test guidelines, the efficacy of SP versus CQ for the treatment of uncomplicated malaria in children was assessed. Children with fever ≥37.5°C, haemoglobin > 5g/dl, mono P. falciparum infection 2000 – 250000 parasites /μl were recruited in the ratio of 1:2 (CQ: SP) to obtain a sample of 58 for CQ and 120 for SP. SP showed a very high efficacy (98.2% adequate clinical response) in contrast to CQ (37.7%). There were only 1.75% RII responses to SP, in contrast there were 43.7% RIII/II responses to CQ. The decline in parasite density was fast in SP, and the median survival time to parasites clearance was 2 days, 86.7% of the children being aparasitaemic on day3. SP was therefore highly efficacious in this area. The 1.8% clinical and 1.75% parasitological failure rates to SP observed in this area sharply contrasts the 34.0% clinical and 84.4% parasitological failures reported in Muheza emphasizing the need of comparable countrywide data for policy decisions. Keywords: Malaria, children, chloroquine, sulfadoxine-pyrimethamine, efficacy, policy change. Introduction The high level of Plasmodium falciparum resistance to chloroquine (CQ) has compelled malaria endemic countries in Africa to change policy from CQ to sulfadoxine-pyrimethamine (SP). Thus the countries of Kenya, Malawi, Botswana and South Africa replaced CQ with SP (1). In Tanzania, P.falciparum resistance to CQ had surpassed the upper threshold for replacement and the policy has been changed to SP (2). However, prior the change, available data showed that resistance to SP was already established in some parts of the country (3-5). Policy decisions on antimalarial drugs are often hampered by the lack of adequate comparable clinical and scientific data to enable a critical assessment of the magnitude of the problem of resistance for decision-making. This is so because some of the data documenting SP efficacy in Tanzania and other malaria endemic parts of Africa are from studies that included older (> 5 years of age) as well as asymptomatic children who are likely to self-cure (3, 5-6). Moreover, most of the antimalarial drugs efficacy data were based on parasitological (7) instead of clinical (8) criteria, findings that may not give the true problem of clinical resistance. The pharmacokinetic properties of SP (late parasites stage specificity of action) and pharmacodynamic properties (lack of antipyretic effects) raise concerns on possible delayment of parasites and fever clearance that might delay the desired clinical outcome (9-12). These have made some prescribers and clients to maintain the notion that SP is slow acting, which might negatively influence acceptability of the wider use of SP for malaria control. This study was therefore undertaken to: (i) generate comparable SP efficacy data in underfives using the WHO in vivo guidelines (8)thatdocument clinical, rather than parasitological (7) outcome and (ii) prospectively evaluate the hypothesis that, by acting on the late stages of the parasites, SP will lead to delayed parasites clearance (9-11). The study was approved by the Tanzanian Ministry of Health, and consent for participation in the study obtained from parents/guardians on behalf of the children. Patients and Methods Study site, population and sample size The study was carried out at Kibaha District Hospital in a holoendemic area along the coast of Tanzania between April & August 1998. Anticipating a ≥25% P.falciparum resistance to CQ and ≤10% to SP(2), a sample of 58 evaluable patients was calculated as being necessary for a 0.05 significance level and power of 0.85. Given that resistance was higher to CQ than to SP, patients were recruited in a ratio of 1:2 (CQ: SP) to obtain a sample of 58 for CQ and 120 for SP. Consecutive children 12 – 59 months old, attending to the MCH clinic with fever, were selected as described (8). Briefly, haemoglobin was estimated by the Haemocue (a semi-quantitative haemoglobin reader), and parasitaemia assessed by Giemsa stained thick and thin films. Parasites were counted against 200 WBC and converted into count/μl assuming a mean count of 8000 WBC/ l of blood. Enrolment, treatment and follow up Children were selected if febrile with temperature ≥ 37.5°C, haemoglobin >5g/dl, mono P.falciparum infection 2000 – 250000 parasites/μl, not severely sick, not malnourished, and without other co-existing diseases; and were enrolled if parents/guardians consented and were ready to follow the study protocol. History of chloroquine intake was not an exclusion criterion. Consecutive children were serially allocated to either CQ or SP in the ratio of 1:2, following the registration serial numbers. Each child was treated under observation with a standard oral dose based on body weight (8), three doses for CQ spaced in 3 days or a single dose for SP, and if vomiting occurred within 30 minutes, the same dose was repeated. The children were reviewed clinically and parasitologically on each day for the first 3 days and subsequently on day 7, 14, 21 and 28 or any other day as clinically dictated. Quality control Two experienced technicians, unaware of the treatment outcome, did microscopy independently, comparing their results. At enrolment and thereafter, a blood film was declared negative when 100 fields were negative. The PI (DST) closely supervised the study to ensure consistency and accuracy of the data. Evaluation of therapeutic responses Clinical and parasitological responses were assessed as described elsewhere (7-8). Children given a rescue drug on day 0 to 3 were classified as early treatment failures (ETF), and those given alternative drug between day 4 to 14 were classified as late treatment failures (LTF). If no alternative drug given over 14 days, the response was adequate clinical response (ACR). Parasitologically, the children were classified as sensitive (S) & resistant (RI, II & III). Sensitive (S): drop of parasitaemia < 25% day 0 count without recurrence on day 7 or thereafter, RI: day 2 parasitaemia < 25% day 0 count reverting to negative on day 7 but recurring thereafter, RII: day 2 parasitaemia < 25% day 0 count reverting to negative but recurring on day 7; and RIII: day 2 parasitaemia ≥25% day 0 count. Analysis The data were entered into the SPSS statistical package, checked for consistency and analysed. The baseline demographic, clinical and laboratory data for the studied children were explored. Clinical and parasitological responses to CQ & SP were compared using proportions. To assess the speed of action by SP and CQ, survival analysis of the time to parasites clearance (limited to 7 days) was performed. Survival proportions were compared by the Kaplan – Meier curves and the difference in survival times assessed by the log-rank test at the 0.05 significance level. Results A total of 178 children were enrolled, 3 were excluded from the study and 9 dropped out in days 4 to 28. There was no death or severe morbidity/complications recorded and there were no adverse effects. There were no significant differences between treatments with respect to the distribution of baseline attributes except for the geometric mean parasite density (GMPD), which was higher in the SP (42658/μl) than CQ group (35237/μl); and more patients in the SP (40.3%) than CQ group (23.3%) had a previous history of CQ intake. The clinical responses over 14 days (Table 1) showed that SP had a very high ACR rate (98.2%) with only 2 (1.8%) treatment failures on day 14; in contrast, CQ had a very low ACR rate (37.7%) with a cumulative treatment failure (ETF & LTF) of 62.3%. Both SP and CQ treatment outcomes were not associated with the baseline GMPD or previous history of CQ intake. The rate of recurrence (2nd episode of malaria in day 15 to 28) was significantly lower for SP (5.4%) than CQ (22.6%) (P = 0.001). Thus, in 28 days, significantly less children on SP (7.2%) than on CQ (85%) had a 2nd episode (P < 0.001). The three-day fever clearance rates showed that, although up to day 2 a significantly high proportion of the children on SP (40.3%) than CQ (12.5%) had no fever (P < 0.001), the overall fever clearance rate was slightly slower for the children on SP than CQ irrespective of resistance to the latter. Although not statistically significant (P > 0.1), from day 2 to 3 more children on CQ (71.4%) than SP (59.7%) were afebrile. However after day 3, all children on SP had no fever, while 26.1% of those on CQ still had fever due to resistance. The parasitological responses (Table 2) showed that there were only 1.75% RII responses to SP with no RIII responses. In contrast, there were 27.3% RII and 16.4% RIII responses to CQ. The cumulative prevalence of high-level parasitological resistance (RIII/II) to CQ was 43.7%. Given the high rate of transmission in this locality it is probable that RI responses were re-infections (8), thus the cumulative sensitivity (S/RI) was 98.25% for SP and 56.3% for CQ, the difference being highly statistically significant (P<0.001). The distribution of geometric mean parasite densities (GMPD) as % of Day0 count over 3 days showed that overall the % GMPDs for the two groups were almost dropping at the same rate irrespective of the high level of resistance to CQ, except for day2 when the % GMPD was significantly lower in SP (60.5%) than CQ (77.4%) (P = 0.034). Over 14 days, the parasite clearance rates showed that up to day2 significantly more children on SP (57.1%) than CQ (14.5%) had no parasites (P < 0.001), and that up till day3 significantly more children on SP (86.6%) than on CQ (50.9%) had no parasites (P < 0.001). As from day4–7 onwards, the majority (97.6%) of the children on SP in comparison to only 67.3% of those on CQ had no parasites (P < 0.001). Survival analysis of the speed of action in parasites clearance by SP and CQ over 7 days after initiation of therapy (Figure 1.), show that the median survival time to parasites clearance was highly significantly shorter for SP (median survival time = 2 days) than CQ (median survival time = 7 days) (P < 0.001). Discussion The data showed a very low level of P.falciparum resistance to SP in the study area in comparison to other areas (3-5). Indeed, by the clinical and parasitological criteria (7-8), the efficacy of SP stood at 98.2% ACR and 98.25% S/RI sensitivity. However, an unacceptably low CQ efficacy was observed with a cumulative treatment failure of 62.3% and high-level parasitological failure (RIII/II) of 43.7%. Clearly the observed CQ failure rate had surpassed the upper threshold (≥ 25%) for replacement (8) hence the need for the policy change (2) for which the findings clearly support. The peculiar observation of 34% clinical and 84.0% parasitological failure rates to SP in Muheza Tanzania is conceivably attributed to a prophylactic intervention with antifolates (3) and the widespread use of SP for uncomplicated malaria following prescribers’ dissatisfaction with CQ as the use of CQ in the Muheza area has had been unrealistic for some years before the current official policy change (13-15). Although SP is still effective in most parts of the country, the lack of antipyretic effects have the potential to make the drug less readily acceptable by prescribers and clients as well. Thus, although after day3 all the children on SP had no fever while 26.1% of those on CQ still had fever (due to resistance), though not statistically significant, CQ was slightly faster than SP in fever clearance, especially between day2 to 3. This indicates that despite the high efficacy (98.2%), SP has a slow symptoms relief. This forms the basis of the widespread notion among researchers, prescribers and clients that SP is slow acting conceivably due to the absence of antipyretic effects (12). Thus, even when resistance is not a major problem, SP is thought to produce clinical improvements rather too slowly. The late parasites stage specificity of action raises concerns on possible delayed clinical and parasitological responses to SP treatment (9-11). However, from the distribution of % GMPDs over 3 days and the parasite clearance rates over 14 days, it appears that in the absence of resistance, SP has a rapid parasite clearance as shown by the relatively short median survival time of two days to parasites clearance, with 86.7% of the patients being aparasitaemic on day3. The rapid parasite decline and high therapeutic efficacy support the wider use of SP as a first line drug. The observation that significantly more children on SP than on CQ were malaria free in day 15-28 indicates that SP maintains sub-therapeutic drug levels responsible for preventing re-infections. The long residence of SP in the body (elimination phase extending to days 15-52 after treatment) serves two clinical purposes: eliminates the parasites responsible for the illness (clinical cure) and ensures an infection free period in days 15-28 (a beneficial prophylactic effect), but however, this is also the span of selection for resistance in holoendemic areas (16). Acknowledgement This work was supported by DANIDA / ENRECA under the Tanzanian – Danish Collaborative Research and Training Programme, Phase III 1998 – 2001, Project III. We are thankful to the Permanent Secretary, Ministry of Health Tanzania for approving the study. Special thanks go to Mr Federick Kalokola for handling the laboratory work. Thanks are due to the parents / guardians and staff of Kibaha Hospital for their co-operation in this study. References
© Copyright 2005 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp05004t1.jpg] [lp05004t2.jpg] [lp05004f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}