 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 2, No. 1, April, 2005, pp. 17-20 Lung Function Among Low- and High-Exposure Workers in Small-Scale Wood Industries in Tanzania. Larama MB Rongo1, Anoek Besselink2, Françoise Barten3, Gernard I Msamanga1, Wil MV Dolmans4, Dick Heederik.2 1Dept. ofCommunity Health,
Muhimbili University College of Health Sciences, Tanzania Code Number: lp05005 Abstract Objective: Exposure to wood dust can cause a variety of lung
problems, including chronic airflow obstruction. The aim of this study is to
evaluate lung function and its determinants among workers exposed to wood dust
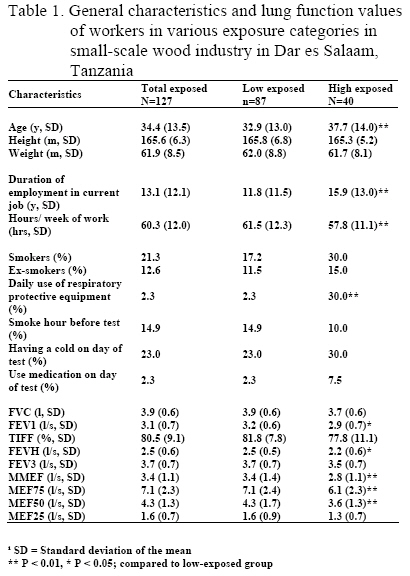
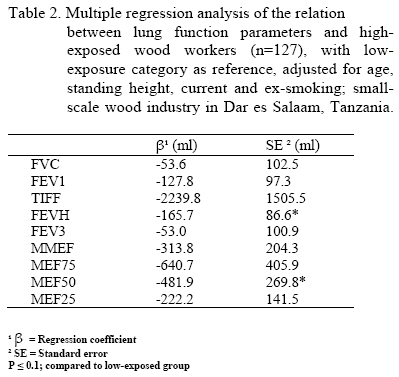
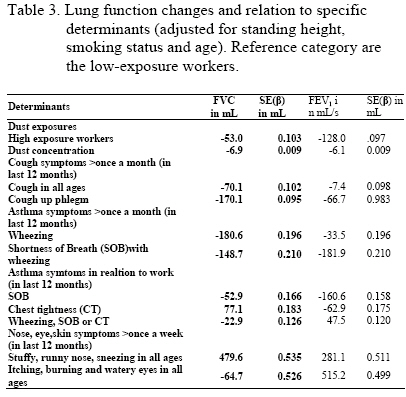
in small-scale wood industries in Tanzania. Keywords: Lung function, respiratory health, small-scale wood industries, Tanzania Introduction Exposure to wood dust has been associated with respiratory effects including acute and chronic changes in lung function, rhinitis and eye and nose irritation. Most evidence comes from studies in Western Europe and North America (1-4). Three studies have been conducted in the continent of Africa assessing lung function indices in workers in large industries (5-7). Shamssain (1992) in Umtata, Republic of Transkei (South Africa) showed lower lung function in 145 exposed male workers than in the control subjects, and the proportion of the men with an FEV1/FVC below 70% was higher in exposed workers than in control subjects (5). Fatusi and colleagues studied respiratory symptoms, peak flow and spirometric measurements among 59 sawmill workers from privately owned sawmills and in 199 control subjects matched for age and sex (6). The results showed a high prevalence of respiratory symptoms (cough, chest pain and sputum production), conjunctivitis, and skin irritation among the exposed. Ige and Onadeko in Nigeria assessed occupational related symptoms, and peak expiratory flow rates among 500 saw millers and 500 university workers and students free from fumes and smoke as a control matched for age and sex (7). A sub-sample of 120 saw millers and 120 controls did full spirometry tests and the mean values of the spirometry measured were lower in saw millers than the controls. In previous study, we observed increased respiratory symptoms prevalence, elevated nose and eye irritations, skin symptoms, and high prevalence of allergy/sensitivity symptoms among workers exposed to wood dust compared to unexposed (7). We conducted lung function measurements among 87 high exposure workers to wood dust and 40 low-exposure workers to see whether the exposure was associated with a lower lung function. Materials and methods Subjects In the previous study (8), a respiratory health questionnaire was administered to 546 workers exposed to wood dust and 565 non-exposed workers and the association between symptoms and job-title based exposure was studied. We categorized the exposed workers into low (415) and high (131) depending on exposure levels and job-title (8). In this study, we evaluated lung function in randomly selected sub-sample of 87 workers from low exposed group and 40 workers from high exposed group. All the workers were Africans from different tribes in Tanzania. Small-scale wood industries The characteristics of these small-scale wood industries are different from those found in large-scale industries in developed countries. Most of the industries consist of a temporary shelter with four poles supporting a roof thatched with old corrugated iron sheets or palm leaves. Most of the tasks there were done manually. The only small-scale industries with permanent shelters were the ones fitted with wood machinery. No exposure control equipment such as exhaust ventilations were fitted in any of the workshops. The wood machine operators receive tasks from other small-scale wood industries using hard wood that is difficult to process manually. The tasks commonly done are planing, sawing, carving and drilling hardwood like East African teak tree (Chlorophora excelsa), mahogany (Khaya nyasiga), blood wood (Pterocarpus angolensis), East African camphor (Ocotea usambarensis) East African Afzelia Burl (Afzelia quanzensis), ”mtanga” (Albizia ssp), African pencil cedar (Juniperus procera) African blackwood (Dulbergia melanoxylon and “kawilia” (Grevillea robusta). Podo (Podocarpus gracilion), cypress (Taxodium distichium) and pine (Pinus patulla) are the common soft wood species. Questionnaire A short questionnaires were administered face-to-face to the workers from SSWI and the following variables were recorded:- age, height, weight, sex, temperature, smoking last 1 hour, colds in the past 24 hours, and taking medicines against respiratory problems in the last 24 hours. Exposure Categories We sampled wood dust measurements in 115 wood workers. Dust exposure categories were formed on the basis of observations during a walk through survey prior to measurements based on workers area and job title. Two categories (low exposed and high exposed) were formed as described elsewhere (8). Lung function measurements Spirometry was performed at the worksite using Vicatest VCT-5 dry spirometer (Mijnhardt, Bunnik, The Netherlands). Age was recorded in full years; standing height was measured with a standard anthropometric scale attached to the body weight scale. Weight was measured to the nearest 0.1 kg and height to nearest 0.1 cm. All the subjects were advised to leave smoking one hour before the test and not eat a big meal two hours before doing the test. The spirometer was used to determine Forced Vital Capacity (FVC), Forced Expiratory Volume in 1 second (FEV1), the ratio of FVC to FEV1 (TIFF), partial Forced Expiratory Volume (FEVH and FEV3), Maximum Mid-Expiratory Flow (MMEF), and Maximum Expiratory Flow at 25, 50 and 75 % of the FVC (MEF25%, MEF50%, MEF75%, respectively). The spirometer was calibrated with a 3-litre precision syringe (PULL-MARK III pump) before testing. The same equipment and observer were used to all subjects and the recordings were made between 8.00 and 17.00 and directly entered into a computer. Subjects performed the lung function tests while seated, wearing a nose clip, and all volumes were corrected to body temperature and pressure saturated with water vapour (BTPS). Each subject was instructed to practice deep inspiration and forceful expiration before completion of the forced expiration. The subjects were allowed to rest for 2 minutes between each measurement. Repeated FVC measurements were performed until at least three acceptable curves were obtained. A satisfactory test required that the FVC and FEV1 of two manoeuvres be reproducible within 5%. The best test per individual (highest FVC and FEV1) was recorded as the lung function capacity of the worker (9). A total of 127 out of 130 workers participated in the study and the response rate was 98%. Analysis: After all the corrections, data were analyzed using SAS statistical software (SAS 6.12; SAS Institute, Cary, NC) (10). Multiple regression analysis was performed for the different lung parameters (adjusted for age, standing height, and smoking status) to determine if there was a difference in distribution between the low exposed group, and high exposed group. Results Table 1 shows the characteristics and lung function values of the 127 wood workers involved in the study stratified by exposure category (low=87 and high =40). Significant differences existed in age, duration of employment in the current job, smokers and daily use of protective equipment between low-exposure workers and high-exposure workers, and these factors were therefore adjusted for in multiple regression analyses. The mean crude FVC for low-exposure and high-exposure workers was 3.9 litres and 3.7 litres, respectively. Mean FEV1 for low- and high-exposure workers was 3.2 L/s and 2.9 L/s, respectively. Significant differences were detected in all lung function indices when low-exposed and high-exposed workers were compared except in FVC and FEV3. Table 2 shows the results of multiple regression analysis with a comparison of low- and high-exposure workers. Current and ex-smoking, age, and standing height, were adjusted for in the regression analysis. Lung function parameters seemed to decrease slightly with increased exposure to wood dust. The low-exposure category was taken as the reference group because no lung function data were available for a non-exposed group. We performed additional data analyses in which everyone below the age 25 years was considered of age 25. This was done to allow for potential lung growth effects, which can result in a plateau in lung function between the ages 18 and 25, and a decline from age 25. No clear differences were observed with earlier analyses. Symptoms were associated with a lower lung function as well (Table 3). Discussion. We found a weak and statistically insignificant negative relationship between lung function and wood dust exposure, but the relationship was not statistically significant. After considering age effects between age 18-25 years, correlation for smoking in different ways (yes/no, smoking/ex-smoking versus pack years) and inclusion of duration of exposure, the negative relationship with exposure remained the same. The observed changes could be explained by the small power of the study, small sample size or lack of comparison group. We found elevated respiratory symptoms in high-exposure workers compared to control group (8). Pulmonary reduction for high-exposure workers seems to be consistent with the high prevalence of symptoms, suggesting the existence of a dose response relationship. Age, smoking status and standing height were confounding factors in the study and were adjusted for in the calculation of odds ratio and regression analysis. All the workers were Africans so race was not considered as a confounder. Similarly, the few females who were involved in the study were removed from the analysis and hence sex was not considered as a confounder. Since we had no reference values to compare with, we used low-exposure workers as control and high-exposure workers to dust as exposed. Although misclassification can play a role, it is unlikely that the small decline differences observed in lung function indices is due to misclassifications of the exposure groups. Other factors like low immunity, malnutrition, past TB or even malaria could affect lung function indices but this is unlikely for most of the work is done manually and workers with these conditions would be less likely to continue working and this would be random in both groups. Since most of the workers were self-employed, change of employment is also unlikely. Although it difficult to compare this study done in SSWI with studies done in organized industries like those of Ige and Onadeko 2000, and Fatusi and Erhabor 1996, the decline in lung function indices in high-exposure group is seen in all when low-exposed and high-exposure workers were compared (6-7). The methodology used in this study is also different. Other studies compared lung function declines across-shift (11-12). In our study, FEV1 and FEV1/FVC% (TIF) were higher in the low-exposure compared to high-exposure workers. A study done in Republic of Transkei in South Africa (5), and in a sawmill in west-central Alberta (2,13) have shown similar results. All these studies had a control group not exposed to wood dust. Halpin’s study compared the mean-normalized FEV1, and mean-normalized FVC in low-exposure workers, high-exposure workers, and non-exposed workers and found that the indices were in high-exposure workers (14). Therefore a more rigorous study including a control group outside wood industry should be done to confirm dose-response trends observed. In conclusion, exposure to softwood and hardwood in small-scale wood industries is also associated with a non-significantly reduced lung function. Acknowledgements The authors are indebted to the management and workers of the small-scale wood industries for their participation. The authors also thank the Research Assistants for their assistance in data collection. Larama MB Rongo was supported by a research fellowship from the Netherlands Foundation for the Advancement of Tropical Research (WOTRO) and Netherlands Organization of Scientific Research (NOW). References
© Copyright 2005 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp05005t3.jpg] [lp05005t1.jpg] [lp05005t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}