 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 2, No. 1, April, 2005, pp. 21-26 Felt Occupational and Environmental Health Hazards Among Workers in Small-Scale Industries in Dar Es Salaam, Tanzania: Focus Group Discussion Study LMB Rongo 1, S de Haan 2, F Barten 2, G I Msamanga 1, WMV Dolmans 3, T van Naerssen 4, D Heederik 5 1Dept. of Community Health, Muhimbili
University College of Health Sciences, Dar es Salaam, Tanzania Code Number: lp05006 Abstract Objective: While the informal sector is rapidly emerging as the
major source of employment in poor countries, little is known to the health
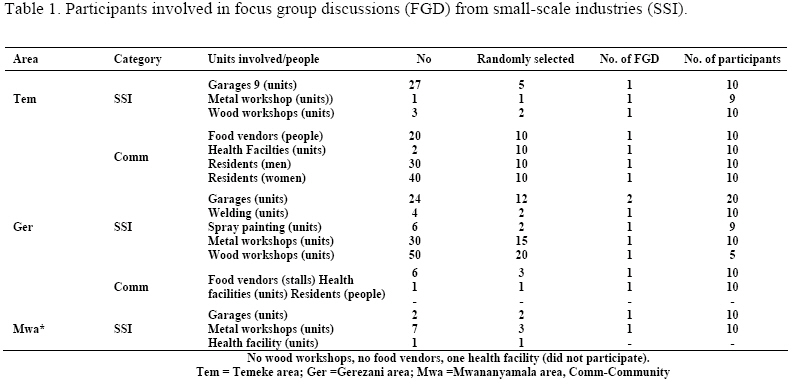
hazards encountered by the workers in small-scale industries (SSI). Key words: Urban informal sector; occupational health; environmental health; community participation; focus group discussion Introduction Urbanisation and its accompanying increase in urban poverty in many countries of the South has led to an increasing burden on the urban environment and thus on urban health. Although the population is predominantly rural, the proportion of urban residents has been increasing steadily from 6% in 1967 to 13.8% in 1979 to 18% in 1988 (1). A national census in August 2002 showed that the population of Dar es Salaam was 2,497,940 people (2). Urbanisation may also be a response to poverty especially in rural areas. The impact of the environment on the health of people is not equally distributed within cities but affects the urban disproportionately. Between September 1994 and February 1996 we conducted a qualitative study on the health aspects of the informal sector enterprises in Dar es Salaam. This paper describes the results of a FGD study on felt occupational and environmental health hazards among workers in small-scale industries, and the perceived occupational and environmental health hazards among health workers, food vendors and residents in the vicinity of SSI in three wards of Dar es Salaam. It is assumed that felt and perceived health hazards differ. We know about health hazards in SSI but people involved could experience them differently. This study uses focus group discussion to discover the differences. The participatory approach and the qualitative methodology used provided the participants with the opportunity to emphasize their own priorities and health needs and perspectives. Methods Study area Dar es Salaam City consists of three Municipalities (Temeke, Kinondoni and Ilala) which are divided in 52wards (3). Three of these wards (Temeke, Mwananyamala and Gerezani) were selected conveniently and included in the study. Concepts In this study a distinction is made between the felt health hazards and the perceived health hazards. The health hazards are "felt" by the exposed population (the population at risk) i.e. small-scale industries employees and workers and "perceived" by outsiders (e.g. health workers, food vendors and residents living near SSI). Participants The researchers made a selection of participants for FGDs after doing a walk through survey in the small-scale industries. The walk through survey also enabled the researchers to prepare a checklist to be used by a moderator during conduct of FGDs. Table 1 summarizes the categories of participants in the focus group discussions. Assessment of the felt occupational and environmental health hazards Focus group discussion. An interview schedule (checklist) to guide the FGD was designed and pre-tested before use with the help of a social scientist (SH). The moderator used a checklist containing questions for assessing crowding, exposures to dust, welding fumes, soldering fumes, excessive noise and chemicals (acids, benzene, kerosene, degreasing agents, asbestos, spray fumes)). We also discussed exposure to accidents and injuries, ergonomic conditions, working conditions and use of protective devices. The last question in the checklist was open to any other felt OHH. Sampling criteria We randomly selected small-scale industries from the three study areas. Then we informed the owners of the SSI in writing. The work of selecting a participant to join an FGD was left to heads or owners of the SSI. The participants selected in all the three areas are summarized on Table 1. Oral consent was requested from each participant. Conduct of the Focus group discussion Each focus group discussion had the following: a moderator, recorder, secretary taking notes, observers (researchers) and participants (either workers from garages, metal workshops, wood workshops, health workers, or comprising of residents living near the SSI, or potential food vendors. One FGD took one hour and consisted of 6-10 participants. Soft drinks were provided to the participants at the introduction and at the end of FGD. The checklist was prepared in English and translated in Kiswahili. Kiswahili is the national language of Tanzania. The moderator was a social scientist conversant in English and Kiswahili. Details of the conduct of FGD are explained elsewhere (4). Following each FGD the first impressions were discussed and written by the moderator, observers and the secretary. Transcription and translation of the FGD was done immediately after completion of the FGD. Data processing and analysis The transcripts and notes from each FGD were then analyzed using content analysis by means of a set approach according to guidelines given by Varkevisser and colleagues (1991)(4) and Kaguna-Amooti and Nuwaha (2000) (5). At the first analysis step, the transcripts and notes were ordered to the topics addressed by the discussion. At the second step of analysis, issues that were brought forward repeatedly or were discussed at length by the participants, and relevant parts from each FGD and notes were ordered by these issues, using a ‘cut and paste” method. The third step was to make a summary of the results for each FGD, based on the issues that were discussed by various groups. The summaries were reviewed by one other experienced person in qualitative methodological research, to test whether the summaries were good representations of the FGD and the summaries were then revised based on his comments. Finally, an overall summary of the discussion was made. Results Description of the study population The majority of the 88 participants 68% (60/88) had completed primary school education, 69% were married and 59% had a family to take care of (52/88). The mean age was 31 (range 15 to 55 years). Below are felt occupational and environmental health hazards by SSI workers, and reported health complaints. Overcrowding As a primary discontent overcrowding was expressed as a big problem in the SSI areas: 'There is no planning or separation of different activities, things are done randomly, you may work very close to someone who is doing a different job from yours and as a result you experience the hazards from someone else's job as well' (operator). Accidents In most of the FGD the risk of accidents and electric shocks was mentioned. In five of the nine FGD among employees and operators, cutting oneself and the risk of contracting tetanus was seen as a serious problem: 'It is quite normal for us to get cuts but we do not have any first aid. We apply acid or kerosene on the site and continue working '(employee, metal workshop). Exposures to excessive noise, dust, and welding fumes Exposure to high noise levels was rarely felt as a problem. On the contrary: there were several striking remarks on how noise could improve the hearing capacity of people: 'There are absolutely no hearing problems, as we are always exposed to all kinds of noises we can hear much better' (operator garage). 'First these hammering jobs cause hearing problems, but later as one gets used to the job there are no hearing problems' (employee, metal workshop). Working conditions The majority of the participants reported that they were working with old and inadequate equipment. Both the lack of adequate equipment and capital to purchase new equipment were directly related to the health problems encountered during their work. This was seen as the commonest reasons why workers got problems with their health. 'We know all the work safety rules and regulations which will enable us to avoid sicknesses, but the problem is lack of equipment' (employee, garage). Ergonomic conditions The participants in the FGD never mentioned the bad ergonomic conditions, that were common at the work places in the enterprises and these could have made an important contribution to health problems such as backaches and other joint pains. Environmental pollution The employees and operators of the small-scale industries felt that their enterprises did not cause many problems to the physical environment. Only the garbage disposed in the area, the fumes from the cars at the garages and the lack of sanitary facilities were mentioned as sources of pollution. ‘Since there are no toilets around and people relieve themselves in the open, when it is raining the filth is spread close to our working area' (employee enterprise). Permanent workplaces All open spaces (plots) in the City of Dar es Salaam are managed by the City Council. They are earmarked by the city for specific future developments. The owners of SSI invade these open spaces and illegally construct temporary shelters in which they conduct their business. Some of the enterprises had licenses to perform their business. This caused a lot of insecurity for the operators and did not encourage them to invest in their workplace to improve the working conditions. ‘'We are more or less like the street vendors, the City Council can kick us out any time' (operator, garage). 'The garages can get loans for improving their working conditions, but suppose they are chased out, who will repay the loan? We just need the authority to remain in our premises' (operator, garage). Investment in occupational health and safety The lack of investment by the operators in their enterprises was associated with several problems. The workplaces were mostly unsheltered and as a result they exposed the employees to sunburn and rain and lowered the availability of work during rainy season. Furthermore, the workplaces were unfenced which created an unsafe environment for the properties of both the operators and the customers. This had again an economic impact: ‘'We are unable to get bigger jobs because our working places are not sheltered and there is virtually no security for customers to leave their cars or items' (operator, garage). Reported chronic and acute health complaints by workers in SSI For the problems attributed to the occupational situation the participants made a clear distinction between “severe” (acute) and “normal” (chronic) health complaints. Chronic health complaints and causes Chronic health complaints were headaches and skin diseases. Headaches were caused by working in the sun or by working with thinner and paint. An operator of a garage mentioned that: 'Headaches are always there, we just take a Panadol tablet every now and then and it is over'. The exposure to paint, grease, working with chemicals, and welding was said to cause skin problems. An employee expressed himself: 'Most of us have the attitude that skin disease cannot kill an African, so sometimes we do not even care to wash our working clothes'. Acute health complaints and suggested causes The fact that respiratory tract problems, eye problems and accidents were felt and perceived as acute health complaints indicates how severe the problem is in relation to the impact it has on the capability for the workers to continue working. The employees and operators mentioned eye disorders, respiratory diseases and accidents as severe health problems. Eye problems were related to exposure to the radiation caused by welding, and to exposure to the bright fires used for metal work. The lack of protective gear was seen as the main reason for developing eye problems. However, some of the operators had a different opinion, one of them said: ‘We can buy the protective gears, but the workers may not use them unless you scold them and sometimes force them'. Respiratory diseases were said to be caused by exposure to welding fumes, to chemicals inhaled during spray painting, to chemicals from car batteries, and to saw dust. The majority of the employees and operators associated the exposures to welding fumes, spray painting, and (saw) dust with contracting tuberculosis (TB). The overcrowding of the working areas was only once mentioned as a possible risk factor for TB. The general living situation (overcrowding in homes) was never mentioned as a potential factor. A typical statement was: 'I think TB is caused by thick dust. When welding, especially in a dusty car, the dust really affects you; the first thing being a running nose and the worst effect is TB. And as you know we do not even get milk after such jobs, thus we can easily get sick'. Insecure working conditions of the small-scale industries These remarks have to be viewed in the light of activities of the Dar es Salaam City Council (under the authority of the Regional Commissioner) to 'clean the city'. In this campaign in the early 1995 large areas of the city centre were 'cleaned' from the street vendors with their merchandise. These people are also operating in the informal sector. Income from SSI Most of the operators and employees did not get a fixed salary. The income depended on the availability of work: 'You work, you get money and just eat it' (employee, metal workshop). 'But suppose it rains for two consecutive days, or you fall sick and have no money, so it is always wise to have a budget to cover for, at most, six days to come' (employee, metal workshop). The youngsters who were doing an on the job training received very little salary, under the guise of getting education. The consequence for almost all the workers was that they had an unstable and low income, which did not give them the security to provide themselves and their families with the basic needs of daily life. The income is so low, even if I would get TSH 500 (< US 1) a day it is still not enough' (employee, metal workshop). Other sources of income beside SSI Most of the participants said they had no other income generating activity besides their work in the small-scale enterprise. This corresponds to the results from the Informal Sector Survey mentioned before. However, some participants made remarks that would support another opinion: 'Living in this country you must use your brains, you must do something to supplement your income' (operator, garage). 'Depending on the income of your small-scale industry alone is just waiting for your death' (employee, garage). An operator of a garage said in a separate interview we had with him: 'I believe that everyone here has some other income generating activity, either a retail shop, a grain milling machine, or a grocery, but these are kept as secrets by the owners, they would not want anyone around here to know that they own such things'. A few employees came with concrete examples: 'I have a chips selling business at a Muslim school, my younger brother helps me in that' (employee, metal workshop). 'I have a cart and some gallons. I have employed someone as a water vendor. In the evening he brings me the income he has acquired that day and I pay him' (employee, garage). Occupational and environmental health hazards as perceived by food vendors, health workers and residents near SSI. Food vendors The food vendors complained about the lack of water, and the problem of garbage and dirt that were scattered in the area. They said they did not experience any problems related to the small-scale industries because 'they are our customers'. Residents Two FGDs were conducted among residents, one each among women and men. Of the 12 women who participated, 8 were involved in petty business or food vending and were often directly dependent on the small-scale industries as their customers. Of the six men who participated only one was working in the study area. He had his own small-scale enterprise (a grain milling shop). Environmental health hazards Among the residents different opinions were uttered. The female residents were not very keen on expressing their views on the activities of the enterprises in their residential area: ‘'We do not face health problems related to those enterprises because they are our customers'. Concerning the enterprises the problem of garbage, lack of sanitary facilities and excessive noise were mentioned as causing problems for their living environment. 'There is no water and the garages in this neighbourhood do not have toilets. Stomach problems and diarrhoea are prevalent here' (female resident). In the FGD among male residents the environmental health problems related to the enterprises were fairly exaggerated (varying from problems like dizziness to heart problems and diabetes). Occupational and environmental health hazards as perceived by the health workers from health facilities near SSI. In the FGD with the health workers their perception on the occupational health hazards of the informal sector workers was comparable to the felt health hazards mentioned by the operators and employees. The main health problems mentioned were related to respiratory tract, eye and skin diseases, trauma and accidents. There was a disagreement with the operators and employees on the risk of getting tetanus infection: 'They just demand tetanus injections whenever they get hurt, it is not that they actually get the disease'. Once a general remark was made related to the health of the workers. 'Most of these workers are weak, they do not eat properly, and some times they go without food for long periods'. In one of the FGD among the health workers the issue of plot allocation was again put forward as an explanation for the little initiatives observed for improving working conditions: ‘The enterprises know that they can be chased out of their premises anytime since they have no permits for their plots, that is why they do not even care to improve their premises'. The health workers mentioned the problems of sanitation and garbage: 'The area (Temeke) is overcrowded, there are no toilets for people to relieve themselves so they resort to do so in open spaces, thus the entire place is so polluted. The surrounding houses are affected. 'The environment is very dirty. The City Council trucks used to come for garbage collection, it is many years now since they stopped coming' The increasing number of mosquito breeding places, dirty water pools with the risk of billharzia and the garbage from which flies can transmit diseases were also discussed. Discussion Most of the workers reported overcrowding, accidents and injuries, exposure to excessive noise, and poor working conditions as their felt occupational health hazards. The felt environmental problems included environmental pollution, lack of permanent workplaces and poor investment in occupational health and safety. The reported health problems included what they called “normal” health problems and “acute” (or “severe”) health complaints. The perceived occupational and environmental health problems as seen by residents and health workers included shortage of sanitary facilities as well as poor solid waste disposal. Both employers and health workers reported non-use of personal protective equipment by the workers in SSI. Remarks that they should tell us about their problems and how to solve them showed a dependent attitude. These responses could partly be explained by the fact that the community was not involved in the set-up phase of the project. As described by Cornwall (1995) participatory research involves "recognizing the rights of those whom research concerns, enabling people to set their own agenda's for research and development and so giving them ownership over the process"(6). In the approach chosen in our study researchers defined the first priority after consulting the community. When we compared the findings from this FGD with those where the workers were alone, the results were similar. However, we did not include the findings in the major analysis because of fear that there might be an information bias that we had no means of correcting it. In any FGD we did not chase away intruders for they were looking for the truth and could influence attendance of subsequent FGD. All the participants in FGD from the SSI were males. This was in contrary to the results found in the study done in Dar es Salaam in the informal sector where male/female employment in the total informal sector in Dar es Salaam comprised of 60% males and 40% females (7). However, female informal sector workers were mainly engaged in the trade/restaurants and hotels industry. Primary school was the highest level of education attained by the participants and this finding was found to be similar to that of the Tanzania informal Sector survey in 1991 (8). The results of the FGD show that, except for the exposures to noise and the bad ergonomic conditions, which we perceived as serious occupational health problems for the workers, the operators and employees were aware of many health risks they were facing during their work at the enterprises. Although the knowledge on how a certain exposure could lead to an illness was often lacking, the result of different types of exposures was known and often the use of relevant personal protective equipment was mentioned as a possible way of prevention. In 1993, ILO conducted a pilot study on occupational health and safety in the informal sector in Dar es Salaam (7). The worksites for this study were selected from the informal sector enterprises connected to Non Governmental Organizations (NGOs) working on promotion of employment possibilities for youth. This NGO only accepted enterprises that had more or less permanent place to operate. This formed the main difference with the enterprises included in our study and the different results obtained could partly be related to this aspect. Thirty worksites were included in the ILO study representing the trades of: furniture making; metal work; tailoring and shoemaking; services like garage work, vending and butchery; traditional art; construction and food processing. In our case the issue of insecurity can, at least partly, clarify the lack of action from the side of the operators. As emphasized by Schulz (1995) and as shown in our study the (local) government has an important role to play in creating a more secure working environment (9). The input the operators and employees would be willing to give is of crucial importance for any further activities planned. Benavides (1992) wrote about the little environmental consciousness on the part of small-scale entrepreneurs who are usually working at the survival level and cannot afford to concern themselves with activities not directly related to their productivity (10). Packard (1989) (11) and Acheson et al (12) reported that urban people who are unemployed or marginally employed had high rates of common infectious diseases including TB, pneumonia and venereal diseases. The findings by Packard (1989) were similar to our study where we reported that occupational and environmental issues were given a low priority by workers. District health systems need to be strengthened and reoriented towards health promotion, prevention and protection (13). Attention is needed to ensure that integration of occupational health with Primary Health Care goes beyond the establishment of a separate, vertical programme (14). For example, health promotion aims to work with people in the 'settings' of their every day life, focusing on building 'healthy workplaces' or 'healthy neighbourhoods', rather than focusing on people at risk for specific conditions or already in contact with the health services (15). The level of awareness among the workers may be considered a positive factor and will make the workers themselves become more actively involved in improving their working or living conditions or in the decision making process about their future. Conclusions and policy recommendations This study conclude that workers in SSI felt that they were aware of the various health hazards they were exposed to and they could only invest on improvement of working conditions if there was a permanent land allocation for their workshops. References
© Copyright 2005 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp05006t1.jpg] |
| |||||||||

{kind=link}