 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 2, No. 1, April, 2005, pp. 27-31 Breastfeeding and Complementary Feeding Practices in Tanzania AK Hussein Correspondence to: A.K Hussein, School of Public Health and Social Sciences Muhimbili University College of health Sciences, P. O. Box 65015 Dar-Es-Salaam, Tanzania Dept. of Community Health Code Number: lp05007 Abstract Objective: The main objective was to assess infant feeding
practices in Tanzania as part of the process towards the development of the
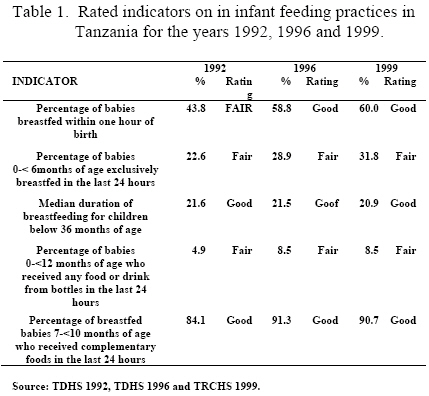
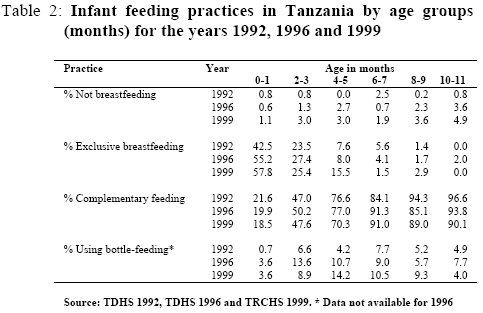
National Infant and Young Child Nutrition Strategy for Tanzania. Key words: Breastfeeding, complementary feeding practices, infant and young child feeding practices, WHO/ Linkages Tool, Tanzania Introduction Tanzania is the largest of the three East African countries. It lies between degrees of latitude 1° and 12°S and degrees of longitude 29°and 41° East. It shares borders with Kenya and Uganda on the North; Rwanda, Burundi and the Democratic Republic of Congo on the West; Zambia, Malawi and Mozambique on the South. On the Eastern side, the country is bounded by the Indian Ocean. The people of Tanzania belong to over 120 different ethnic groups and according to the 2002 Population and Housing Survey, the population is 34.5 million. Children under the ages of one and five years constitute 3.5% and 16.5% of the population respectively. Malnutrition among underfive year old children is a public health concern in Tanzania with the high prevailing rates showing little improvement over the years. Data from demographic and health surveys show that the prevalence of stunting and underweight have remained constant at around 43-44% and 29-31% respectively (1,2,3). The prevalence of wasting however increased slightly from 6% in 1992 to 7% in 1996 and then declined to 5% in 1999 (1,2,3). Infant and young child feeding practices are important determinants of the health and nutrition status of children below the age of five years (4). Tanzania was one of the countries that had adopted the Global Strategy on Infant and Young Child Feeding (4). An assessment of the status of infant and young child feeding practices was undertaken as part of the process towards the development of a National Strategy on Infant and Young Child Nutrition for Tanzania and a Plan of Action for the National Infant and Young Child Nutrition Programme. In this paper some of the findings of the assessment which was done between February and March 2004 are presented. Methodology Information on breastfeeding and complementary feeding practices in Tanzania was collected by using Part One of the WHO/ Linkages tool - Infant and Young Child Feeding: A tool for assessing national practices, policies and programmes (5) and through search of published and grey literature. Part one of the WHO/ Linkages tool has been specifically designed for assessing infant and young child feeding practices. Information collected using the WHO/ Linkages tool can be presented as rated or non-rated. Rated information compares a country’s achievement with that of others and this is classified as “poor”, “fair”, “good” or “very good” (5). The tool ratings had been developed based on an analysis of percentages achieved by countries on the various indicators using Demographic and Health Survey (DHS) data as well as that from selected national studies. Data was collected for five indicators which are: percentage of babies breastfed within one hour of birth; percentage of babies 0-< 6 months of age exclusively breastfed in the last 24 hours; median duration of breastfeeding for children below 36 months of age; percentage of babies 0-<12 months of age who received any food or drink from bottles in the last 24 hours and; percentage of breastfed babies 7-<10 months of age who received complementary foods in the last 24 hours. Data on each of the five indicators assessed were obtained from Tanzania Demographic and Health Surveys of 1992, 1996 and the Tanzania Reproductive and Health Survey of 1999 in order to assess the country’s performance over time. The exclusive breastfeeding and bottle feeding rates were calculated using the “automatic calculators” that were available in the electronic version of the WHO/ Linkages tool. Appropriate two–month increment data from published DHS tables were entered in the specified areas of the “automatic calculators”. Data for the other three indicators were obtained straight from the Demographic and Health Survey tables. The level of achievement for each of the five indicators for 1992, 1996 and 1999 was then rated as “poor”, “fair”, “good” or “very good” using the WHO/ Linkages tool criteria. Search for published and grey literature from Tanzania on breastfeeding and complementary feeding practices entailed contacting informed persons in the area of infant and young child feeding; local library searches; web search- Pubmed and internet search using Google search engine. For this article, additional literature published in early 2005 has also been included. Results A. Trend in breastfeeding and complementary feeding practices from Demographic and Health Survey data The rated indicators presented in table 1 reflect the situation on breastfeeding and complementary feeding practices in Tanzania for the years 1992, 1996 and 1999. Table 1 reflects an improvement on three indicators i.e initiation of breastfeeding rate, exclusive breastfeeding rate and percentage of breastfed babies 7-<10 month complementary fed. Table 1 also shows that over time, the median duration of breastfeeding has remained constant while the bottle feeding indicator has regressed. The ratings have however, remained constant throughout the years with the exception of the initiation of breastfeeding indicator that had changed from “fair” in 1992, to “good” in 1996 and maintained the same rating in 1999. Indicators for exclusive breastfeeding and bottle feeding were both rated as being “fair”. It is important to note that none of the indicators had ever scored “very good”. Table 2 shows that early complementation is very common in Tanzania with about 20% of children aged 0-1 months having been already started on complementary foods and 50% of those aged 2-3 months of age being already complemented. A small proportion of infants who were supposed to have been already started on complementary foods at 6 months of age were still on breast milk only (Table 2). While the proportion of Tanzanian infants who are not breastfed is small, table 2 shows that generally there has been an increasing trend in the proportion of infants not breastfed for all age groups. Table 2 also shows that there has been an increasing trend in exclusive breastfeeding rates in the age groups 0-1 and 4-5 months between 1992 and 1999. The proportion of infants receiving complementary foods at age 0-1month has also decreased from 21.6% in 1992 to 18.5% in 1999, while it had increased for infants aged 6-7 months i.e. 84.1% in 1992 to 91.0% in 1999. Although bottle feeding is not common in Tanzania, it is seen that this peaks around age 2-7 months (See table 2). B. Findings from review of literature There is paucity of literature on recent infant and young child feeding practices in Tanzania. About eighteen articles and documents on the subject that were written between the years 1981 and 2005 were reviewed, with only nine having been written within the last five years. The study setting included Dar-es-Salaam, Arusha, Moshi, Njombe, Makete, Mbulu, Dodoma urban and rural, Morogoro urban and rural, Igunga and Kilimanjaro. Most of the documents were reporting on results obtained from cross sectional studies both community and facility based; only two articles reported on the findings of an anthropological study. Breastfeeding Practices i) Initiation of breastfeeding Initiation of breastfeeding was reported in seven articles. Studies done in Dodoma, Mbulu and Dar-es-Salaam reported that this was universal. The interval between delivery and initiation of breastfeeding ranged from one hour, to a few hours and to a whole day (6-9). In a study done in Morogoro, Shirima et al established that urban mothers initiate breastfeeding earlier compared to rural mothers (10). ii) Prelacteal feeds The practice of giving prelacteal feeds was reported to be common in Igunga and Dar-Es-Salaam i.e. 25% and 17% respectively (8,11). The prelacteal feeds were either formula milk, glucose water or plain water (8,11). Agnasson et al established that the type of prelacteal feed given to the newborn infant depended on where the baby was born (11). For babies born in a health facility this was usually glucose water while for babies born at home plain water was more commonly given. iii) Colostrum feeding A high proportion of babies were reported to have been fed colostrum. This was 100% in Dodoma and 99% in Dar-Es-Salaam (6,8). A substantial proportion of the mothers in Igunga (46%) and Mbulu (34%) were reported to discard colostrum (7,11). Mothers from urban areas of Morogoro were less likely to discard colostrum compared to mothers from rural areas (10). iv) Exclusive breastfeeding The practice of exclusive breastfeeding was reported to be rare among mothers from South Western Tanzania (12). In Igunga and Mbulu districts exclusive breastfeeding was only practiced for the first two and four months of life respectively (7,11). Shirima et al established that mothers living in urban areas exclusively breastfed longer compared to those living in rural areas (10). v) Duration of breastfeeding Children are breastfed for a long time in Tanzania. Studies reviewed showed that the duration of breastfeeding ranged from 18 to 36 months in Arusha; 2 to 3 years in Dodoma and 2 years in South Western Tanzania (6,12). In Dodoma it was reported that mothers abstain from sex while breastfeeding and that mothers who get pregnant before weaning were ashamed as they would be unable to continue breastfeeding (6). vi) Other undesirable breastfeeding practices Undesirable breastfeeding practices that were documented include practice of unilateral breastfeeding and abrupt weaning (6,13). Cessation of breastfeeding before age of two years was found to be linked with malnutrition in 68% of children admitted at the Dodoma regional hospital (13). Complementary Feeding Practices i) Timing of introduction of complementary foods Reviewed literature shows that other foods apart from breast milk are usually introduced at an early age in Tanzania (6,7,13). The exact time when these are introduced depends on many factors including geographical locality and ethnic group. Amongst the nomadic tribe of Wadatoga in Mbulu district, animal milks are usually introduced before two months of age with grain based solids introduced at nine months of age (7). In Dodoma complementary foods were reported to be introduced when the infant is three to four months of age (14). Sellen and Mabilia established that weaning patterns were influenced by seasonal factors, with adult staples being introduced at the end of long rains in Mbulu district and Dodoma (7,14). ii) Maternal socio-economic status In Morogoro, mothers in medium and high-income groups introduced other foods earlier compared to those in lower income groups i.e. 1-2 months in the medium and 5-6 months in the high-income group, respectively (15). Urban mothers were found to delay longer introducing other foods compared to rural mothers (15). iii) Type of complementary foods Cereals were usually the first foods to be introduced in Dodoma and South Western Tanzania (6,12,13). Common cereals reported were maize and millet; these are prepared as thin gruels that are gradually thickened. By the time the child is 12 month of age it is already on an adult diet (14). iv) Frequency of feeding complementary foods Frequency of feeding was reported being three times per day but becomes less during peak labour season (16). v) Impact of women’s participation in economic activities Wandel et al established that women participation in food production had both positive and negative effects on the nutrition status of children (16). This was because although there was an increase in household food supply, mothers had less time for cooking and care of young children. HIV and infant feeding Information on HIV and infant feeding practices in Tanzania is very limited. It has been established that wasting among HIV positive pregnant women in Dar-es-Salaam is associated with increased risk of intrapartum and early breastfeeding transmission of HIV-1 infection (17). Poggensee and de Paoli interviewed women attending antenatal clinics on their breastfeeding and complementary feeding practices (9,12,18). Poggensee et al assessed infant and young child feeding practices in Tanzania and Uganda in the context of global recommendations on infant feeding options for HIV positive mothers (12). The practice of exclusive breastfeeding for the first 6 months was found to be rare in Tanzania and they concluded that this had important implications on the infant feeding advice given to mothers whose HIV status may not be known (12). In the study done by de Paoli et al in Kilimanjaro district, pregnant women were also asked on the infant feeding option that they would choose if they found that they were HIV positive (18). Most of the pregnant women interviewed expressed concern over the safety of exclusive breastfeeding and responded that they would opt for alternative infant feeding if they were found to be HIV positive. The most feasible infant feeding option identified was cow’s milk as commercially prepared infant formulas were reported as being too expensive; heat treated breast milk and wet nursing were not practical options(18). Women also expressed a great concern for the social consequences of not breastfeeding and they specifically cited lack of support from partners and associated stigma (18). Discussion The importance of good nutrition and appropriate infant feeding practices on achieving optimal health outcomes cannot be over emphasized (4). It has been documented that appropriate feeding practices have both short and long term impacts. These include growth failure, increased susceptibility to childhood infections, poor school performance, impaired intellectual and social development (4,19-21). Findings from review of literature on infant and young child feeding practices in Tanzania compare well with published Demographic and Health Survey data. Compared to other countries, Tanzania is doing well on three of the five WHO/Linkages rated indicators on infant and young child feeding. These are percentage of babies breastfed within one hour of birth, median duration of breastfeeding for children below 36 months of age and percentage of breastfed babies 7-<10 months who received complementary foods in the last 24 hours. Tanzania did not score well on the other two rated indicators i.e. percentage of babies 0-<6 months exclusively breastfed in the last 24 hours and percentage of babies 0-<12 months of age who received any food or drink from bottles in the last 24 hours which were both rated as “fair”. The good performance on three out of five rated indicators could be attributed to implementation of national guidelines aimed at promoting optimal infant and young child feeding practices. While the majority of women in Tanzania breastfed their babies, a very slow increase in the proportion of infants not breastfed has been observed over time (1-3). Although the increase is small, this is alarming and needs to be addressed urgently through increasing awareness to health workers and community members on the dangers of bottle feeding as well as stricter enforcement of the Tanzanian Code of Marketing of Breast Milk Substitutes. The practice of discarding colostrum which is a rich source of various nutrients and immunological substances for the newborn infant was found to be common in some parts of the country (7,10-11). Another documented undesirable infant feeding practice in Tanzania is that of giving prelacteal feeds. Studies have shown that this practice ranges from 17% to 25% in different parts of the country (8,9,11). The practice of giving prelacteal feeds has been established as being more prevalent in Pakistan (94%), Bangladesh (77%) and India (77%) compared to Tanzania (22-24). Study findings have established that women in urban areas are more likely to initiate breastfeeding earlier, to exclusive breastfeed longer and to discard colostrum less compared to those in rural areas. A likely explanation is that women in urban areas are more educated and more informed on good infant feeding practices. Rural residence, illiteracy and low socioeconomic status have also been found to be associated with shorter duration of breastfeeding in Pakistan (23). Although the rating on the duration of exclusively breastfeeding was “fair”, exclusive breastfeeding for the first 6 months of life is not a common practice in Tanzania with some infants being introduced to foods and drinks other than breast milk as early as day one (7,11-12). As most of the studies have been done in rural areas, the duration of exclusive breastfeeding in urban areas is largely undocumented. Working mothers in Tanzania are entitled to twelve weeks of fully paid maternity leave eligible after three years from the last birth and to have paid one hour or two half hour breaks to go and breastfeed their infants. According to a recent unpublished report, the majority of working mothers are unaware of their entitlement to the one hour or two half hour paid breastfeeding breaks. The duration of paid maternity leave, limited awareness to entitled breastfeeding breaks during working days and lack of baby crèches at work places makes it very difficult for working mothers to exclusively breastfeed their infants for the first six months of life. The timing of the introduction of other foods and drinks apart from breast milk to infants is very important. The term “weanlings dilemma” was coined to reflect the predicaments facing young infants associated with “too early” and “too late introduction of complementary foods. There is overwhelming evidence to associate occurrence of diarrhoeal diseases, upper and lower respiratory tract infections with introduction of complementary foods below the age of six months (19-21). None of the reviewed publications on infant and young child feeding in Tanzania addressed the issues of safety of complementary foods. Research done elsewhere has established that when prepared under unhygienic conditions, complementary foods become contaminated with various pathogens and this causes diarrhoeal diseases and consequently malnutrition and sometimes even death (20). Conclusion There is paucity of literature on recent infant and young child feeding practices in Tanzania especially that related to HIV and infant feeding; feeding practices of working mothers; safety and adequacy of complementary foods. The high levels of malnutrition in underfive year old children in Tanzania that have not shown much change over the years is a reflection of inappropriate breastfeeding and complementary feeding practices. Some progress has been made on the rates of initiation and duration of breastfeeding and complementary feeding which have been rated as good using the WHO/ Linkages assessment tool. Recommendations In order to improve breastfeeding and complementary feeding practices in Tanzania the following recommendations are put forward: I. There is a need for more research work focusing on young child feeding practices, more specifically on exclusive breastfeeding and complementary feeding practices among HIV positive and working mothers, nutritional adequacy and safety of complementary foods. II. Strong advocacy on the importance of colostrum, exclusive breastfeeding especially for the first 6 months, on the dangers of prelacteal feeds and bottle-feeding and optimal complementary feeding practices to both health care providers, community and the policy makers is needed. III. Working women should be made aware on their entitlement to paid breastfeeding breaks. Acknowledgements: The author would like to acknowledge Dr. D. Nyagawa who took part in the data collection as an assessment team member, the unconditional assistance provided by the Tanzania Food and Nutrition Centre and WHO Afro for funding the assessment. I also acknowledge all the people from the Ministry of Health, Muhimbili National Hospital, District Hospitals and Muhimbili University College of Health Sciences who willingly agreed to spend time responding to our many enquiries. Rerences
© Copyright 2005 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp05007t2.jpg] [lp05007t1.jpg] |
| |||||||||

{kind=link}
{kind=link}