 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 2, No. 2, Oct, 2005, pp. 1-5 Treatment Paths and Referral Patterns Among Caretakers of Under Fives Admitted with Malaria at a Regional and a District Hospital in Kilimanjaro Region, Tanzania Rachel N. Manongi1, A.M. Rønn2, W. M. V. Dolmans3 and I.C.Bygbjerg2 1Dept. of Community Health, 2Department of International
Health, Institute of Public Health, University of Copenhagen, Denmark Code Number: lp05009 Abstract Objective: To determine, in caretakers hospitalised
with children suspected of malaria, what action was taken at home, which health
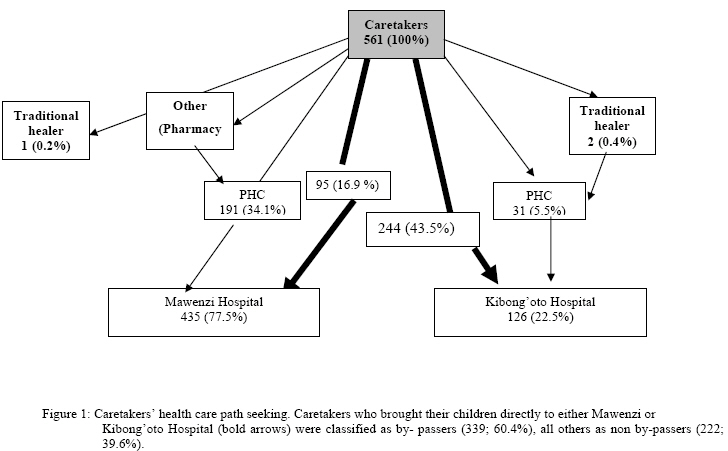
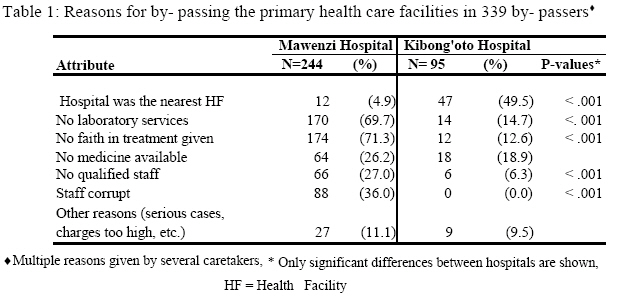
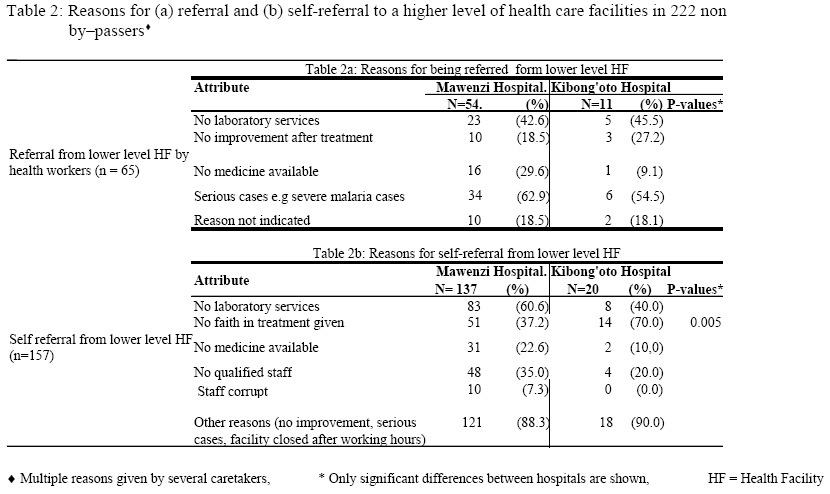
facility caretakers selected and the reasons for the choice made. Key words: Childhood malaria, home treatment, referral system, laboratory services, quality care, Tanzania. Introduction Early diagnosis and adequate treatment are the basic elements of any disease control programme and should be seen as a fundamental right of all populations affected by malaria (1). Realising this right, current reforms of health systems in sub-Saharan Africa focus upon decentralisation of health services to lower level of health care with the aim of bringing health care as near to the family as possible. In Tanzania, health services comprise a hierarchical system of different levels of health care (pyramid structure). The three lower strata (primary health care post, dispensary, and health centres) are referred to as primary health care units (PHCUs), which are the first level of care. In rural areas, the official health service is mainly carried out at primary health care posts (2). The quality of care is assumed by the users to be higher on each successive step. Within the PHCUs in rural areas there is often lack of well-trained personnel (3).Those with high training often remain in the urban centers. The referral and consultancy hospitals with highly specialized professionals in the urban centers usually cater for a very small percentage of the population (4). In Tanzania there is under-utilisation of the PHCUs which are close to the families, five kilometres being the greatest distance a patient has to walk to reach a modern health facility (5-6)The main reason for this phenomenon is assumed to relate to poor quality of services within these units (5,7). Malaria remains the number one health problem of Tanzania, primarily affecting children under five years of age (8). Nonetheless few researchers have explored the treatment paths and patterns for the caretakers of children aged under five admitted for malaria at district and regional hospitals and the reasons for choices of first health facility. Since the caretakers of the under fives are involved in diagnosis, making decisions for the choice of health facility and the promptness with which child care is sought, identifying factors that influence caretakers’ treatment paths and choices of health services could contribute to restructuring these PHCUs realistically and lead to better utilisation of health services. One feature of this work is that nearly all studies on treatment seeking behaviour are based on recall, i.e. asking people what they would do/what they did a month a go when their child experienced fever rather than a situation analysis of the present situation. The objectives of this study were: To determine actions taken by caretakers at home when perceiving a child under five years to have malaria and to identify choice of health facility by caretakers when perceiving malaria symptoms and the reason(s) for it. Materials and methods Study area and population This hospital based descriptive, cross-sectional study was conducted from April to June 2002 in Mawenzi regional and Kibong’oto district hospitals in Kilimanjaro region. Mawenzi hospital is situated in Moshi town in Moshi urban district while Kibong’oto hospital is in a rural area in Hai district. Both hospitals are located on the slopes of the highest mountain in Africa – Mount Kilimanjaro but at different altitudes (850 meters and 1300 meters above see level, respectively). The climate in Kilimanjaro region varies substantially throughout the region due to variation in altitude, which contributes to the variation in malaria endemicity. The two main tribes in the region are Chagga and Pare who are known for their relatively high levels of literacy and consciousness to economic development (9). Malaria transmission peak is usually during or soon after the rainy season, which is February to May. Caretakers of children under five years of age admitted with suspected malaria at Mawenzi or Kibong’oto hospitals were enrolled in the study, if all of the following criteria were fulfilled: a) malaria was symptomatically diagnosed using common signs and symptoms of malaria, b) children were not suspected to have other disease, c) children did not die before the time of interview. Caretakers were either parent or guardian (somebody taking care of the child after admission, other than the parent and not a staff of the hospital). Caretakers were regarded as non by-passers of the referral system, if they were (self-) referred from primary care level to a higher level of health care, in this case, to Kibong’oto or Mawenzi hospitals. In this study those who went to a pharmacy or visited a traditional healer before going to a hospital were also considered as non by-passers as they were few. By-passers were caretakers who did not follow the referral system, that is, went directly to one of the mentioned hospitals. Sample size and sampling technique Mawenzi hospital admits an average of 30 children under five years of age with clinical diagnosis of malaria, and Kibong’oto hospital about 10 per day. A feasible sample of 561 caretakers were recruited after they were admitted as follows. At Mawenzi hospital, every sixth caretaker, and at Kibong’oto every sixth caretaker, who attended the hospital during the study period was selected to participate using systematic sampling. Data collection Caretakers were interviewed face-to-face by a trained interviewer working as a clinical officer in the paediatric ward, the first day of admission using a structured interview schedule. The interview schedule included three fields of interest: a) demographic characteristics of the caretakers; b) care given at home if any and c) choices of health services outside home. Respondents were allowed to give more than one response when applicable. Data analysis Data were coded and entered into SPSS Version 9, Inc-Chicago, USA and checked for consistency. Descriptive statistics were calculated. Categorical variables were compared using Chi Squared test. Significance level was set at 0.05. Multiple responses were allowed. Ethical clearance Ethical clearance was obtained from National Institute for Medical Research (NIMR) as part of the Joint Malaria Programme and from the KCM College Research Ethics Committee. The study was explained to caretakers and discussed with staff in the hospitals involved, especially of paediatric wards. Informed verbal consent was obtained from caretakers. Results A total of 561 caretakers of children under five years admitted with malaria were interviewed, 435 at Mawenzi and 126 at Kibong’oto hospital. Overall, 90.6% were mothers, 2.1% fathers and 7.3% guardians. The majority (84.5%) of caretakers were married. Caretakers were Chagga (57%), Pare (13.0%), Masai/Meru (5.9%) and different other tribes (24%). There was no marked difference in education between parents and guardians as most (71 –92%) had seven years in school and were farmers/peasants. The age of children of caretakers included in the study ranged from 0.2 months to 59 months (mean 24.5 ± 16.1 months), and with no significant differences between the children from either hospitals. The commonest symptoms that prompted caretakers at home to perceive a child as having malaria were fever (89.7%) and vomiting (42%). After the perception of malaria, 78.6% of the caretakers gave tablets as a first remedy at home and these were mainly antipyretics. A small percentage (2.8%) gave local herbs at home, while 18.6% waited for further symptoms. For those who gave drugs, Antipyretics were used as the first remedy by 95% of caretakers for perceived malaria symptoms; 5% gave antimalarials or a combination of antimalarials and other drugs. Caretakers did not give anticonvulsants even when convulsions had occurred. Fever (72.3%), was the most common symptoms that prompted caretakers to seek treatment outside home. The decision to seek treatment outside home was made mostly by mothers (55.6%), followed by fathers (35.5%), guardian (7.5%) and others (1.4%). An overview of the health care seeking path of the caretakers is presented in the Figure. The majority of the caretakers 556/561 (99.1%) opted to seek treatment in formal health facilities other than traditional healers (0.5%) and pharmacies (0.4%). Out of 561 caretakers, 60.4% went directly to one of the regional/district hospitals (by-passers), while 39.6% were non by-passers. Choice of health facility by caretakers to seek treatment outside home and their reasons are shown in Table 1 and 2. The main reasons for by-passing the lower level health facilities were lack of faith of treatment given (71.3%) and lack of laboratory services (69.7%) for Mawenzi hospital. For Kibong’to hospital the main reason was that it was the nearest health facility (Table 1). Of those who considered the hospital to be the nearest, the majority took less than half an hour to reach these hospitals in normal walking conditions 75% (9/12) and 42.5% (20/47) (p=0.04) for Mawenzi and Kibong’to respectively). Of those who considered the hospitals not to be the nearest, the majority was from Kibong’to, 81% (39/48) and it took them more than one hour, while at Mawenzi this figure was 32.8% (76/232) (p <0.001). Among the by-passers from both hospitals, caretakers with children older than 1 year were significantly more likely to by-pass (P=0.01) than those with children under one year. Those residing in a town were significantly more likely to by-pass (p =0.001) than residents in a village. Parents’ education, marital status, social-economic status, and number of under-fives in the house were not significantly associated with by-passing. Of non by-passers, 65/222 (29.3%) were referred to one of the two hospitals from a lower level due to seriousness of the illness and lack of laboratory facilities. No faith in treatment given was significantly more frequently given as a reason for self-referral among the caretakers in Kibong’oto as compared to Mawenzi hospital (p=0.005; Table 2). Discussion When caretakers were asked to mention reasons which promoted them to seek treatment outside home, common symptoms of malaria were mentioned. This may be biased as caretakers had already been admitted with malaria as diagnosis, but in other studies general community knowledge on malaria was also found to be high (10-13). In the present study, 79% of the caretakers gave tablets at home and only two percent gave local herbs after perceiving the child as having malaria. Of those who gave tablets, 95% gave first only antipyretics and 99% of them would subsequently go to a formal health facility for further examination. Similar findings were also reported in a study in Kibaha, eastern Tanzania, where 87% of mothers gave antipyretics when the child had symptoms of malaria and 93% of the mothers would take their children to a formal health facility after home remedy (12). In a study from southern Tanzania it was shown that modern care health facilities were used in 90% of fatal malaria cases as a first resort to care (14). This indicates that at household level caretakers do not give their underfives antimalarials before being advised to do so. On the one hand this may help reducing drug resistance but on the other hand, this approach may delay prompt treatment of malaria if it is present. Other studies found that home treatment (15) and self –medication through retail shops were common (16-17). Among the caretakers, mothers were most likely to be the ones who decided to seek treatment outside home unlike other studies where mostly the fathers took such decisions because of their economic power (18). Our finding is not surprising because most caretakers were mothers and the main tribe in our study was Chagga who are known for their economic enterprising and the role of women in this. Further, a larger percentage of Chagga men travel out of the region for work or business purposes leaving wives and children behind (9). In our study, most caretakers by-passed the PHCUs and opted to be treated directly at a regional/district hospital. The reasons given differed from caretakers admitted in a regional hospital situated in town and those in a district hospital situated in a rural district. In town, the main reason given was need for laboratory tests to ascertain the diagnosis and get correct treatment. Lack of laboratory services, and may be bad experiences with ineffective chloroquine treatment among many other reasons, resulted in caretakers having no faith in the “blind” treatment given at the lower level of health care. Laboratory confirmation of malaria is important given the overlap of malaria with other conditions (19-20). In the Kibaha study, 89.4% of caretakers (mothers) mentioned the need for laboratory tests (12). For the reduction of severe morbidity and mortality of childhood malaria PHCUs have to meet the requirements for quality services. Unique to other studies done in Tanzania, we found that caretakers were questioning the qualifications of those who work in these facilities. This can be seen as an indicator for peoples’ need to access to a motivated and skilled health personnel (Manongi, et al., 2005; unpublished observations). For the rural district, the PHCUs were lacking, so majority caretakers had to travel more than one hour to a district hospital which was the nearest to them. If the situation is not urgently addressed, it will cause congestion on second level of care and reduce the quality. In our study we did not come across any referral from a district hospital to a regional hospital. The explanation for this may be that the regional hospital is situated close to a consultant hospital, so, serious cases were referred directly. Our study has some limitations; most notably much malaria morbidity and mortality takes place outside the established health system and selection bias could be significant by interviewing only those who successfully survived and reached the hospitals where caretakers in our study were enrolled. To compliment our study a community-based study identifying caretakers of sick children at home would be needed. Conclusions To get good perceived quality care, most caretakers by-passed PHCUs and went directly to the regional/district hospitals. This could lead to overburdening of hospitals and in the end poor quality of health care. The study has shown that caretakers want higher quality of care. It is high time policy makers ensured that every community member has access to equipped PHCUs which are handled by motivated and skilled health worker in order to meet users’ satisfaction and raise the level of care for under fives with malaria within the nearby PHCUs. Acknowledgement This work was supported by DANIDA/ ENRECA under The Tanzanian –Danish Collaborative Research and Training programme, Phase III 2001-2002 and Phase IV 2003- 2005. The authors would like to thank all caretakers who agreed to participate and research assistants for involved in the study and Tumaini University for providing institutional support. The authors are also grateful to Mr. Cyprian Makwaya, Mr.Gibson Kapanda and others for their critical comments on the earlier draft of this paper. Competing Interests There are no competing interests to declare. References
© Copyright 2005 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp05009t1.jpg] [lp05009f1.jpg] [lp05009t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}