 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 2, No. 2, Oct, 2005, pp. 6-11 Knowledge, Attitudes and Practices Regrading Cholera Outbreaks in Ilala Municipality of Dar Es Salaam Region, Tanznia Veronicaa M. Mpazi1 and Kagoma S. Mnyika2 1Dept. Of School of Nurse Teachers, 2Epidemiology
& Biostatistics, School of Public Health and Social Sciences,
Dar-es-Salaam, Tanzania. Code Number: lp05010 Abstract Objective: The aim of the study was to determine
knowledge, attitudes and practices regarding cholera outbreaks and measure
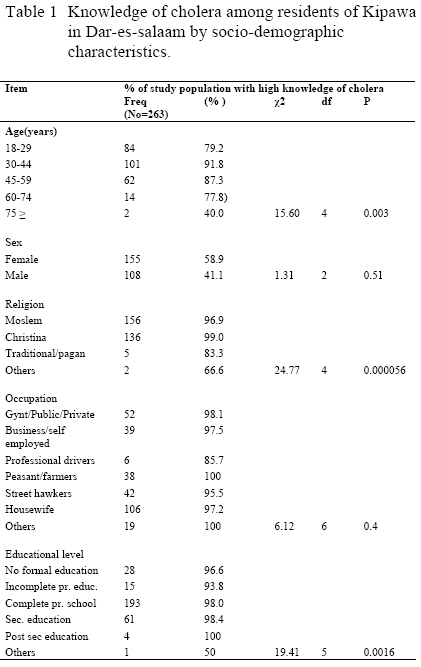
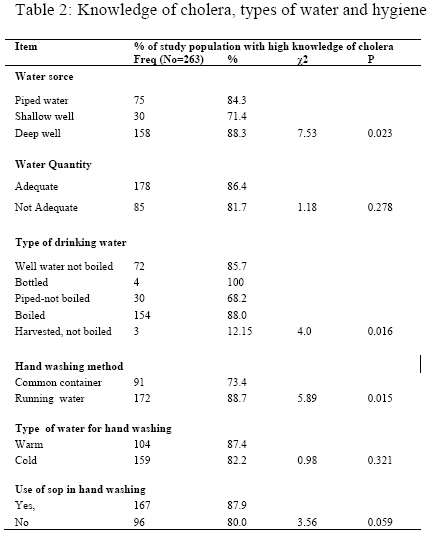
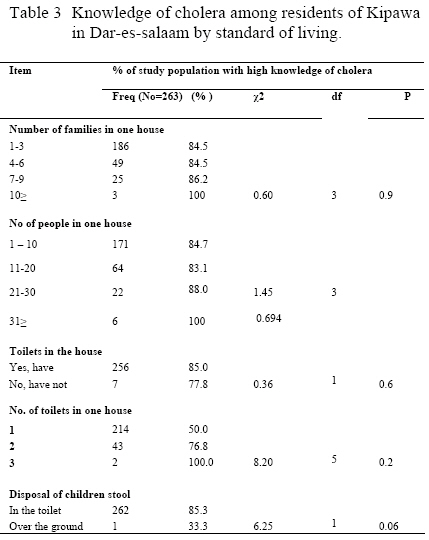
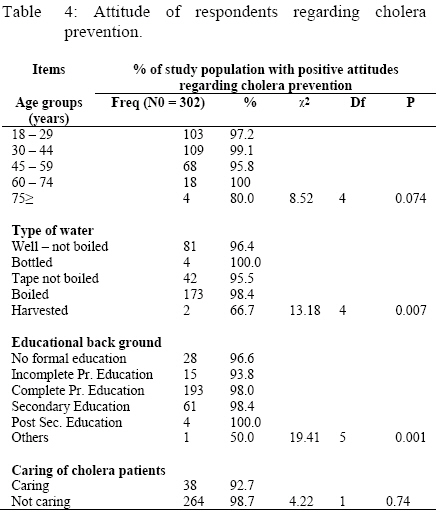
socio cultural practices that influence cholera outbreaks in Ilala Municipality in Dar es Salaam city, Tanzania. Key words: Cholera, Epidemics, Knowledge, Dar es Salaam, Tanzania Introduction Cholera is still a problem in Tanzania. In Tanzania Mainland about 48% of all admissions in the country due to notifiable diseases among patients aged 5 years and above were due to cholera cases in the year 1997. About 57% of deaths due to notifiable diseases for 5 years old and above patients were cholera cases (1). Dar-es-Salaam region is one of the areas mostly hit by cholera outbreaks in the country. Cholera outbreaks have been occurring every year in Dar-es-Salaam city. Many factors such as improper waste disposal, food handling, processing, and preservation, poor housing, improper and inadequate sewerage systems place people at a greater risk of being infected with cholera and other diarrhoeal diseases (2-3). Geographical, socio-economic and socio cultural backgrounds of people in the affected area which influence practices may also contribute to spread of cholera. These include low educational level, unhygienic food handling practices and proximity to surface water (4-5). This is because the bacteria (Vibrio cholerae) that cause cholera are known to be normal inhabitants of surface water (4). In Tanzania, cholera outbreaks have been occurring every year since 1977, when the first person believed to have been affected by the disease was first reported (6). Tanzania was found to have the highest number of cases in Africa in 1997 (40,249) and 1998 (43,000) compared to Guinea Bissau (20,555), Kenya (17,200), Chad (8,801) and Mozambique (8,708) in 1997 and Kenya (18,000), Uganda (18,000) and Somalia (14,708) in 1998 (7). Tanzania had one of the highest case fatality rates in East Africa (5.6) with 2,268 deaths out of 40,226 cases (7). Almost every developing country is facing either a cholera outbreak or the threat of an epidemic. However, with the added burden of water shortages,there was growing concern that cholera could become more difficult to control (8). Furthermore with increased urbanization, cholera will be an increasing problem in future where sanitation and water safety are not adequate. Knowledge attitudes and practice about the awareness of the people to cholera outbreaks is important for planning preventive health education programmes. Cholera control is far cheaper and effective by means of a preventive strategy than a curative one.This study intended to assess the knowledge, attitudes and practice that influence cholera outbreaks in Dar-es-salaam city. If suitable health care policies, plans and programs are to be utilized, greater formative information is needed. Methods Study area This study was conducted in Ilala Municipality in Dar es Salaam region. Dar-es-Salaam region has an average rainfall of 1146 millimeters per annum. There is a constant shortage of water due to unreliable power supply and breakage of water pipes in densely populated areas. The water table is high which cause permanent water bodies to exist. The district borders the Indian Ocean to the east, the Coast region to the west, Kinondoni Municipality to the north and Temeke Municipality to the south. The district covers an area of 210 sq. km with population of 637,573 people. Males are 321,903 and females 315,670. The average number of people in the household is 4.3 (9). The major health problems are malaria, diarrhoeal diseases including cholera, HIV/AIDS and motor accidents. The study concentrated in Ilala municipality in peri-urban areas due to the fact that Ilala has been mostly hit by cholera.Between September 2003 and March 2004, Ilala Municipality was reported to have the highest number of cholera cases (2508) compared to Kinondoni (983) and (415) Temeke Municipality. Kipawa Ward was randomly selected to be our study site. This Ward has a total population of 47,817 people (9). Study design and population The study design was a cross-sectional study. Data was collected using a structured questionnaire with open and closed-ended questions. The study population consisted of household members aged 18 years and above, both males and females. Regardless of whether they knew how to read and write. A multistage random sampling method was employed. In the first stage a list of all wards (N=22) in Ilala District was obtained, one ward (Kipawa) was randomly selected. In the second stage a list of all villages (N=4) was obtained and two villages were randomly selected. In the third stage a list of all hamlets (N=154) was obtained and from which 10 hamlets were randomly selected. All households in the selected hamlets were included in the study. House to house interviews of household members aged 18 years and above was done until the required sample was attained. Information gathered included socio-demographic data and information on knowledge, attitudes as well as socio cultural practices regarding cholera. Data management and analysis Quantitative data analysis All questionnaires were checked daily for completeness after the interview. At the end of interviews, open-ended questions were coded for appropriate computer entry. Quantitative data were entered into Epi- info version 6 computer programme on a weekly basis. Once data entry was completed data were cleaned and validated. Data analysis was conducted using Epi-Info software version 6.0. Chi-squared statistics for contingency tables were used to assess the association between knowledge of cholera, practice and demographic variables. Statistical significance was assessed using p-values and all results were considered significant if P ≤ 0.05. Measurement of knowledge Knowledge scale was used in measuring knowledge, whereby each item was scored correct or wrong and awarded a point then scores were added. A frequency distribution was obtained clearly indicating the lowest and highest point score. A cut off point for no knowledge, low, and high level of knowledge was obtained. There were 11 multiple answers, for each correct answer a score of one point was given, a score of zero point for incorrect answer. A cut off point for low knowledge was 1-6 score and a score of 7 points or more was given for higher knowledge. Questions included were about transmissibility of cholera through eating contaminated food, drinking water and sharing of toilets and shaking hands with infected persons. Others were signs and symptoms of cholera and if cholera can be transmitted through contaminated children stool, chicken feaces and cow’s dung. Measurement of attitudes Direct procedure was employed to measure attitudes. Respondents were asked to provide a self-report on their attitudes towards opinion statements regarding cholera. Likert scale was used in measuring attitudes. About eight opinion statements relevant to the attitude included were, if cholera is a problem, if people are at risk of cholera and also about transmission of cholera. Respondents were then requested to indicate the extent to which they agree or disagree with the statement. Variables were defined and agree and disagree responses were expected whereby each response was given a score. A score of plus one (+1) was given for a correct response and minus one (-1) for an incorrect response. Cut off points were defined where by a score of 4 or more ( ≥ 4) was for positive attitudes and a score or 3 or less (≤ 3) for negative attitudes. The scores were then added. Determining socio-cultural practices The focus was how much of the expected practice was performed; whereby 22 answers were obtained and entered in the Epi Info software version 6. Quantitative data included knowledge of people regarding cholera and attitude statements regarding cholera. Others were types of water source and quality, water treatment and hygiene as well as standard of living. RESULTS Knowledge concerning cholera A total of 310 respondents were included in the study of whom 186 (59.9%) were females and 124 (40.1%) were males. The proportion of respondents with good knowledge of cholera in this study was 84.8%. Table 1 presents knowledge of cholera by socio-demographic characteristics among respondents (N=310) interviewed. The majority of respondents with high knowledge regarding cholera were found between the age groups of 18-29 (79.2%), 30-44 (91.8%) and 45-59 (87.3%). About fifteen percent (47) of all respondents had low level of knowledge concerning cholera. Items contributing to low level of cholera knowledge included issues which need priority attention, if cholera cannot be transmitted by sharing of toilet facilities, improper hand washing techniques and acquiring cholera through shaking hands with a contaminated person. Others thought that cholera could not be transmitted through contaminated young children stools, contaminated chicken faeces, and cow’s dung. Regarding religion, the proportion of respondents with good knowledge of cholera were Christians (99.9%) and Moslems (96.9%). The difference was statistically significant (P<0.01). Housewives were found to have good knowledge of cholera 106 (97.2%) as compared to other groups. Significantly more respondents who completed primary school education 193 (98%) had good knowledge of cholera compared to other educational backgrounds (P= 0.001). Relationship between knowledge of cholera and water source and hygiene The distribution of respondents with high level of knowledge by water source was: piped water 84.3%, shallow well 71.4% and deep well 88.3%. The difference was statistically significant (P < 0.05). The majority of the respondents conceded having access to adequate water supply (86.4%). However the distribution of respondents by water quantity and low level of knowledge was: adequacy of water 13.6% and inadequate water supply 18.3% (Table 2). The distribution of respondents by type of drinking water in both levels of knowledge was: well water not boiled 85.7%, piped not boiled 68.2% and boiled water 88%. A minimum number of respondents reported using bottled water and drinking unboiled harvested roof water (P < 0.05). Furthermore the study revealed that the distribution of respondents with high level of knowledge by hand washing practice was: in a common container 78.4% and running water 88.7% (P < 0.05). Other reported social cultural practices related to water use included type of water used for hand washing: warm water 87.4%, cold water 83.2%, habits of using soap for hand washing 87.8% and not using soap 80.0%. However none of these findings were statistically significant. Overall there was a strong relationship between knowledge on cholera and types of drinking water as well as knowledge and methods of hand washing. Knowledge of cholera by socio-economic status The proportion of respondents by number of families in one house was found to be high between 1 – 3 families with high level of knowledge (84.5%) (Table 3). The distribution of respondents with levels of knowledge by living in one house between 1 – 10 persons was: low knowledge of cholera 15.3% as compared with 84.7% among residents with high knowledge of cholera. About 256 (85.0%) of respondents who reported having toilets in their houses had high level of knowledge on cholera. Furthermore a good number of respondents 214 (87.0%) with one toilet in the house were those with high level of knowledge on cholera. However the differences observed were not statistically significant. The disposal of young children stools over the ground by knowledge level was found to be statistically significant (P < 0.05). Attitude of respondents regarding cholera prevention The proportion of respondents with positive attitudes towards cholera prevention was 97.4%. No significant differences were observed between females (97.3%) and males (97.6%) (Table 4). Furthermore the proportion of respondent with positive attitudes was higher (99.1%) from the age group of 30 to 44 years than other groups. No significant differences were observed between age groups. The proportion of respondents who reported using boiled water for drinking was 56.5%. This includes positive and negative attitudes towards cholera prevention. This was followed by use of well water without boiling (27.1%) and use of tape water without boiling (14.2%). The lowest proportion was use of bottled water and harvested roof water. These findings were statistically significant (P < 0.05). Respondents who had completed primary education had the highest proportion with positive attitudes (Table 4). This was followed by respondents with secondary school education. The proportion of respondents with experience of caring a cholera patient in the family was 13.2%. The proportion of respondents with negative attitudes among those who had cared for a cholera patient in the family was 7.3%. Discussion The proportion of respondents with good knowledge of cholera was high nearly 85%. As expected, analysis of knowledge levels compared to socio-cultural practices and environmental practices showed that practice was lagging behind knowledge and attitudes in this population. These findings are consistent with published data from Peru (10) which showed that practices concerning cholera lagged behind knowledge and attitudes. However, in a cross sectional survey done to assess knowledge, attitudes and practice in Central Africa it was found that the level of knowledge concerning cholera was very low. About 20 percent of people interviewed had negative beliefs towards a disease, 35 percent using unsafe water, 20 percent of households did not have toilets and 4.5 percent to 7.7 percent of the available toilets were not being used (11). Other findings in the present study include inadequacy of water supply by high level of knowledge whereby respondents drink water from wells without boiling. This finding is similar to observations reported from elsewhere (2-3), which have demonstrated that recurrences of cholera outbreaks in Tanzania are due to the use of inadequate and contaminated water. Results of this study show that there is a need of additional information regarding the transmissibility of cholera to correct misconceptions regarding cholera such as cholera cannot be transmitted through contaminated chicken faeces, young children stools and contaminated cow’s dung. Such misconceptions need to be addressed in order to improve cholera control in Ilala Municipality of Dar es Salaam City. In addition, the results of this study show that most of respondents use water from deep wells, piped water and shallow wells. Dar es Salaam is one of the most frequently hit region by cholera outbreaks almost every year. The analysis of socio cultural practices regarding cholera show that cholera outbreaks in Dar es Salaam city might be associated with the use of domestic water from shallow wells and deep wells which is not treated accompanied by the behaviuor of people drinking unboiled water from wells. Furthermore, the statistical association existing between habits of washing hands in a common container for respondents with low and high knowledge, washing hands with cold water and washing hands without soap were noted. These results were consistent with findings reported from Malaysia (5) which showed that food handling practices followed by inadequate safe water and unhygienic environment appeared to contribute to the spread of cholera infection. Khan and colleagues (1981) (12) had previously suggested that the only effective means to control cholera is protecting water supply and the prevention of using contaminated water. Control measures in African settings in Guinea Bissau recommend that in densely populated areas such Dar es Salaam chlorination of water is extremely useful (13). In the present study, the high level of knowledge goes hand in hand with habits which favour the growth and multiplication of Vibrio cholerae. People use pit latrines without lids, solid waste containers without lids and about half of the population studied had no connection to the sewerage system (central liquid waste disposal system). Socio-cultural and socio-economic factors most commonly contribute to the use of contaminated water, environment as well as risk behaviour of individuals (2), which favour the reproduction rate of Vibrio cholerae organisms (14). The proportion of respondents with good knowledge (84.8%) went hand in hand with the proportion of respondents with positive attitudes (97.4%). Our results were not consistent with other studies done to assess knowledge, attitudes and practice in Central Africa which had revealed that people had poor knowledge and negative believes towards cholera (11). Furthermore people have strong misconceptions that young children stools, cow’s dung and chicken faeces cannot be a source of cholera infection. These few observations may contribute to the spread of cholera in this population and are consistent with published reports from Central Africa (11). Generally our findings suggest that knowledge of people, attitudes and practice appear to contribute to the spread of cholera and that practice is lagging behind knowledge and attitudes towards cholera outbreaks in Ilala municipality. Conclusion It is evident from this study that practice is lagging behind knowledge and attitudes in Dar es Salaam. A number of risky socio-cultural practices associated with cholera have been found. The study suggests specific socio-cultural, socio- economic and environmental practices, which should receive priority attention. These include sources and quality of water, types of toilet facilities, access to general sewerage system, management of solid and liquid wastes and other hygienic habits. Findings of this study show that environmental and socio cultural practices may strongly influence recurrence of cholera outbreaks. The above findings together with those of other scientists (14) suggest that socio cultural and environmental factors if not managed well may favour the reproduction rate of Vibrio cholera organisms. In a cross sectional survey done to assess knowledge, attitudes and practice about cholera, the level of knowledge was poor (11). This was not the case in Ilala municipality whereby the proportions of knowledge and attitudes are good. These findings need further investigations to find out why the practice is lagging behind knowledge and attitudes. Drinking unboiled water and use of cold water for hand washing despite the high level of knowledge might be reinforced by socio-cultural factors and educational level. The proper utilization of water should be well informed through mass media and health education programmes. Every household member should learn the proper use of water and other hygienic practices. On the other side, the proportion of respondents who boil drinking water is good; use running water for hand washing and those who wash hands with soap is good. These notable habits might be influenced by low and high level of knowledge. Due to recurrence of cholera outbreaks people might have acquired this knowledge through media and health educational messages since cholera is a long standing health problem in Ilala municipality in Dar-es-salaam. Recommendations Control of cholera can only be effective if people will change their behaviour and no longer practice risk behaviors regarding cholera. The following are recommendations that may be made based on the findings of this study: (i)
Shallow well water
should be treated regularly. Acknowledgement: Authors are grateful to the support received from Dr. D. Mtasiwa (the Dar es Salaam City Medical Officer of Health) and the Ilala District Executive Director as well as the Kipawa Ward Executive Officer for granting us permit to carry out the study in the Ilala Municipality. We are also grateful to Mrs. R. Mpembeni, Mr. C. Makwaya for statistical assistance and Mr. F. Mayunga for assistance in computer data entry and management. The co-opeartion received from Mrs Rose Kasulwa, Mr. Michael Mpanzi, Mrs K. Lidenge and the village community is also highly acknowledged. This project was funded by the Tanzania Ministry of Health and the World Health Organisation. References
© Copyright 2005 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp05010t1.jpg] [lp05010t2.jpg] [lp05010t4.jpg] [lp05010t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}