 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 2, No. 2, Oct, 2005, pp. 12-17 Health Risk Related to Chemicals Used in Small Scale Industries in the Informal Sector in Dar Es Salaam, Tanzania LMB Rongo Dept. of Community Health, Muhimbili University College of Health Sciences Code Number: lp05011 Abstract Objective: Small scale industries are growing very
fast employing majority of the urban poor. Mishandling of chemicals is common
in these industries and most of them are toxic. The aim of this study was to
assess the type of chemicals used in small-scale industries (SSI) and factors
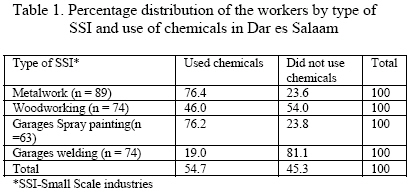
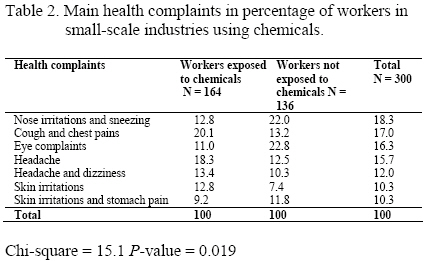
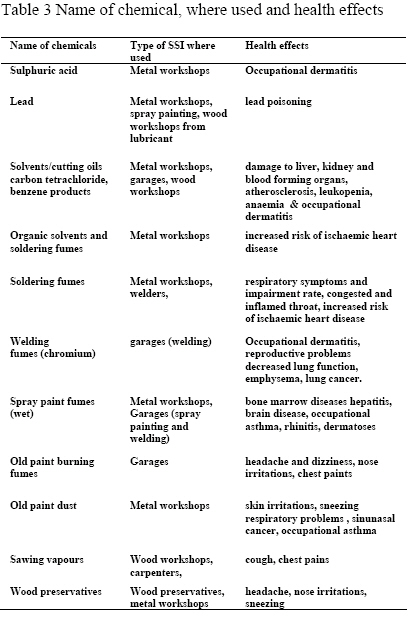
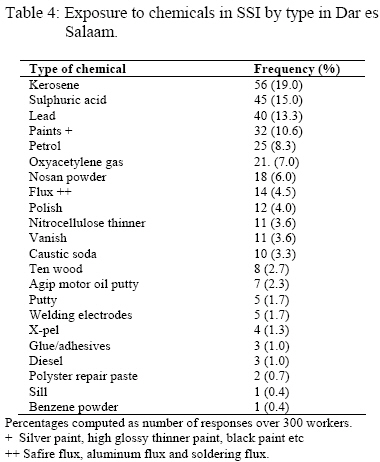
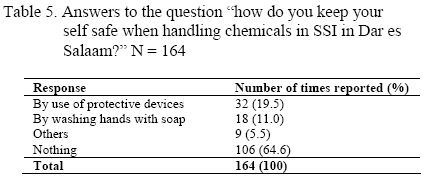
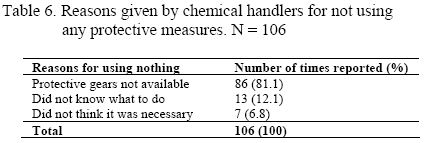
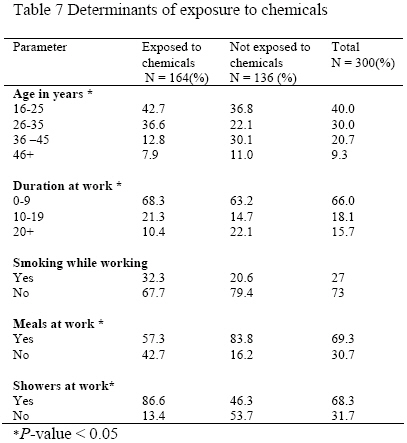
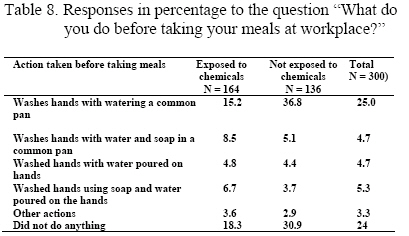
associated with mishandling of chemicals by workers. Key words: Small-scale industries, informal sector, chemicals, awareness, hygienic practices, Tanzania. Introduction Use of chemicals is common in garages, wood workshops and metal workshops. For example in welding/soldering, chemicals like lead, soldering flux, sulfuric acid and benzene are commonly used. Solvents include aliphatic and aromatic hydrocarbons, alcohols, aldehydes, ketones, chlorinated hydrocarbons and carbon disulphide. The vapours of organic solvents may be toxic (1). The health effects due to these chemicals are documented in literature. Workers exposed to paint fumes are likely at risk of bone marrow disease, hepatitis and brain disease (2). Wet paint is also known to cause allergy and other health problems. People exposed to wet paint developed problems such as occupational asthma, rhinitis and dermatoses (3-5). Long term exposure to solvents has been shown to be associated with sinunasal cancer (6-8). Exposure to lead is also common to in spray painting and in storage battery repair (9). In small scale industries workers were also involved in welding and soldering. In welding two methods were commonly used that is arc welding and oxy acetylene gas welding. In metal works soldering was done. Health hazards of these processes were due to inhaling welding and soldering fumes. Edme and colleague (1997) (10) showed that stainless steel and mild steel welders were more exposed to chromium because of inhaling welding fumes and they were likely to have reproductive problems due to weak seamen quality and sex hormones (11), emphysema and lung cancer (12) caused by exposure to welding fumes. Fishwick and colleague (1997) showed decreased lung function in welders exposed to welding fumes (13). Solderers exposed to soldering fumes had higher respiratory symptoms and impairment rates whereas those exposed to metal oxides had congested and inflamed throat (14). Suadicani and colleague study (1995) revealed that combination of exposure to organic solvents and soldering fumes caused an increased risk in ischaemic heart disease (15, 16). They also reported in another study that long term exposure to soldering fumes is associated with risk of ischaemic heart disease (16). A study done by Lucy and colleague showed that exposure to combined affect of wood dust and formaldehyde could cause increased risk in sinunasal cancer (17). Wood workers exposed to wood dust were also exposed to chemicals in a very passive manner. The chemicals in wood dust are in form of its natural substances such as resin acids or monoterpenes and or preservatives. As far as I know there is no any study done in SSI to assess exposure to chemicals among the workers in details. A study published recently only reported that exposure to chemicals is common in SSI without details (4). Methods Study area This study was carried out in low income urban areas of Temeke, Kinondoni and Ilala Municipalities in Dar es Salaam City. One ward with high concentration of SSI in each Municipality was chosen. Sample size and sampling technique A sampling frame of all SSI in the wards was prepared. A total of 500 SSI were recorded; 220 in Gerezani ward in Ilala Municipality, 230 in Temeke 14 ward in Temeke Municipality and 50 in Mwananyamala ward in Kinondoni Municipality. A random sampling technique proportional to size was used to get a total of 90 SSI, 40 from Gerezani ward, 40 from Temeke 14 ward and 10 from Mwananyamala ward. A cross sectional study was done in the chosen industries by interviewing all the workers working in the industries. We also observed and asked about details of chemical names and uses where the generic chemical names were not available. In all industries, 310 workers were eligible for the study. Ten workers refused to be interviewed and the response rate was 97%. Data collection We conducted interviews using a structured questionnaire and a checklist. Research assistants interviewed the workers to obtain information on age, sex, duration of work in SSI, number of years of handling chemicals and use of safety precautions. Additional information focused on uses of chemicals in small-scale industries, sources and perceived health hazards of handling such chemicals. We observed also availability of water supply and sanitation facilities at workplaces. Data analysis Data analysis was performed using EPI-INFO computer software version 6. Qualitative data were analyzed with the use matrix display. We used chi-square test to assess whether observed differences between the exposed and non exposed workers to chemicals were statistically significant. Results A total of 300 workers were interviewed from 90 SSI. The research assistants got support from the workers to obtain the necessary information concerning the various chemicals used in the sampled SSI. The small-scale industries were categorized into four distinct groups. The first groups are those dealing with metal work and manufacturing metal products by cutting/hammering it to the required shape and or without soldering. These workers were mostly exposed to soldering fumes, lead, degreasing solvents like sulphuric acid, ethanol and benzene. They were also exposed to soldering and paint fumes. The second category was wood workers. These were normally exposed to wood dust containing chemicals used to preserve the wood from insecticides. They were also exposed to solvents used to soften vanish and glue in furniture making. The third category was workers in garages specifically welding mild iron and steel. These workers were always exposed to welding fumes containing a mixture of chemicals depending whether they were doing arc welding or flame welding. This group was also exposed to paint fumes/solvents if they happen to weld a surface with traces of paint or degreasing solvents. The last group was painters doing spray painting. It was the most exposed group to multiple health hazards. Before painting was done, the dirty surface has to be cleaned. One way was to use sand paper to remove the old paint from the surface. This process exposed to workers to old paint dust, which is believed to contain lead. On the other hand the old paint was removed by using a flame. Here they were exposed to paint fumes and other volatile gases. They were also using special type of solvent when applied on the surface of the old paint, it swells and it becomes easier to scrap it out easily using a sharp body. Finally while doing spray painting, they were exposed to paint fumes. The fumes may cause borne marrow diseases, brain diseases and hepatitis (2). Assessment of this category of workers as to whether they were using chemicals was subjective. Few members were claimed not be directly exposed although there were counted as welders, woodworkers, metalworkers and spray painters. But strictly speaking, when at the site it is completely impossible not to be exposed to chemicals even if you are not handling or working where they were generated. In this those not exposed they were doing other activities like preparation of work pieces, cutting metal pieces, selling final products, or even supervising other labourers. Table 1 shows that there is significant differences in use of chemicals by type of SSI. About 55% of the workers in the sampled SSI were using chemicals. Type of chemicals, sources, uses and the health hazards. The results showed that SSI workers were heavily exposed to a variety of toxic chemicals, including air dust, welding fumes, spray paint vapors and gases. There were about 22 different chemicals used in SSI and about 60% were potential solvents; benzene and sulfuric acid being among them. Welders, spray painters, wood workers and metal workers were exposed to different types of potentially toxic chemicals. In addition to that, processes like soldering involved chemical reactions in which fumes toxic to the workers were liberated and possibly inhaled. In SSI studied, very few workers were repairing storage batteries. Other sources of lead poisoning observed were from old storage batteries. The lead was used as soldering material and the acid as solvent. In SSI, solvents were used in woodworking as chemicals to soften varnish and glues; in metalwork to remove grease on metal surfaces; while in spray painting were used when mixing paints and cleaning brushes. Solvents were also used for removal of old paint on the bodies of cars, in welding/soldering as cleaning material for surfaces to be soldered and were also used for degreasing oils from their skin and hands. Most of the workers reported complaints such as skin irritations (dermatoses) as a result of handling acids and other chemicals without having protective devices. Among the 300 workers interviewed in SSI, 18% had complaints of nose irritations and sneezing. However, there is significant differences in terms of main complaints when exposed and non exposed were compared. Types of chemicals and personal protective devices. More than twenty different types of chemicals were used in small scale industries in Dar es Salaam. Kerosene, sulphuric acid and lead were the most frequently used chemicals, 43%, 27% and 24% respectively. Gave answers both use of protective devices and wash hands with soap. About 65.0% of the workers handling chemicals in small scale industries in Dar es Salaam did not use protective gears. Only one fifth used protective gears. Of the 106 workers who reported that they did not do any thing to keep themselves safe from chemical exposure, 81% reported that personal protective equipment were not available whereas, 12% did not know what to do. Social demographic characteristics of SSI workers to use of chemicals Tables 7 summarize the social demographic characteristics of the workers. All the workers were males. Women were not at all involved in SSI but they were close to chemical handlers, preparing or serving ready-made foods for the men. The data shows that younger subjects aged between 16-35 years were significantly more likely to use chemicals compared with older age of 36 years or more Table 7.The observed difference is statistically significant, (Chi-square = 17.6; p value = 0.0005 ). There was a significant difference of 11.7% between those who had worked for 0 – 19 years and those who have worked for twenty or more years in terms of handling and not handling of chemicals ( Chi-square = 7.7; p value = 0.0005; df = 1). Hygienic practices in workers handling chemicals in SSI In order to get picture of the different types of exposures to hazardous toxic chemicals and hygienic practices of workers handling chemicals the investigators asked the workers in SSI about various behaviours while at workplace. The investigators asked the workers in SSI whether they smoked cigarettes while at their workplaces, took their meals at workplaces, changed clothes after work and whether they took at bath before going home as a safety precaution taken. Tables 7 summarize the findings. Among the 300 workers interviewed, 45% (135/300) reported that they were cigarette smokers and 54.7% (164/300) handled chemicals. Cigarette smoking behaviour was much more common among chemical handlers compared to non-chemical users, the percentages were 54.3 and 33.9 respectively. The difference was 20.5% (Chi-square test = 12.51; p value = 0.0004). Sixty nine percent of the workers in small scale industries got their meals at work place. More non chemicals users took their meals at workplace compared with chemical users. The observed difference of 26.5% was statistically significant (Chi-square = 24.5; p value < 0.05 and df = 1). About 15 % of the workers handling chemicals washed their hands in a common pan compared with 36% not handling chemicals. It was noted that 18% of chemical handlers reported that they did not do anything before taking their meals compared to 31% not handling chemicals. Further investigation was done to determine what happened to those who did not do anything. Discussion This study was carried out in low income urban areas of Dar es Salaam where majority of the urban poor are found. Most of the urban poor are working in SSI located in those areas. Toxic chemicals, which are auxiliary and by products of other industries, were some of the raw materials used in those industries. Workers in these industries, therefore, fall victims of exposure to toxic chemicals when handling them. Although the workers showed good cooperation during data collection, the research assistants got problems in identifying chemical names of some of the chemicals used at workplaces. Most of the chemicals had trade names only. Effort to see sellers was not very successful because some of chemicals were imported bearing the trade names only. Some of the materials like polish were manufactured at workplace using discarded raw materials like acids from old storage car batteries and polythene papers. The study revealed that handling of chemicals was more common among those in the age below 36 years (62% against 38%). This is the group mostly working in SSI. When the duration of work of the workers in SSI was compared among those who had worked for less or more than 10 years, it was found that there was no difference in handling chemicals. It is documented that the more the duration of exposure, the more the workers were likely to feel the symptoms of occupation diseases (4-5). The results of this study seem not support findings in literature. This could be explained different level of vulnerability of the workers and therefore there are equal number of workers not handling chemicals any more because of health problems in the specified duration of work. In addition to the above explanation, the type of chemicals used like acids and solvents are volatile and vaporize causing acute respiratory inflammation, irritation and sometimes-occupational allergy. Awareness on hazards related to handling of toxic chemicals among the workers was low. They were not able to report long term effects due to handling of toxic chemicals. They reported only the immediate hazards that they felt right on the spot like burning or causing nose irritations. Some effects of handling chemicals without protective devices like skin irritations were not felt as related to handling of chemicals. Although in a different study done by Rongo et al 2004 on focus group discussions, revealed that the level of awareness of occupational health hazards by the workers in SSI was high, this study could not reveal the same results (4). First, the difference perhaps could be explained by the different sampling techniques used to get the samples. Second, might be the workers could not be in position to declare openly that the kind of work they were doing was hazardous. Third, it could be that the workers had not opportunity to do something about the exposures. In Focus Group discussions, the workers who were involved in the discussions were special groups selected by the owners of the SSI or heads of cooperative unions in SSI and could not necessary be reflecting the general awareness on occupational and environmental health hazards among majority of the workers. The study also revealed poor hygienic practices among workers handling chemicals. The poor practices were supported by the following results: personal protective measures were not used, most of the chemical handlers were smoking cigarettes at work place, took their meals with bare hands and few did take showers or change their clothes at workplaces before going home. Non used of protective devices and change of work clothes could be explained by low social economic status of the workers but taking meals by using bare hands after handling chemicals could be due the poor hygienic practices common in workers compounded by ignorance. Some of the workers had exposure to the chemicals orally when taking their meals. A good proportion of the workers were not changing their clothes before going home. There was a possibility of some of the workers transporting the hazards on their clothes and shoes to their families or even to other people because of sharing the same means of transport. The same problems were reported happening in SSI elsewhere in developing countries (4-5). Awkward sources of raw materials like scavenging have been reported as common means of exposing the workers to toxic substances (18). This problem was also common in workers who were extracting the lead from the car battery without facemasks and protective masking (18). Children below the age of 18 years were also employed in SSI. They were seen scraping old paint from bodies of cars using sand paper. Since they were not using any protective devices most of them were exposed to dust containing lead particles. This group at risk was completely not aware of the occupational health hazards they were exposed to. Smoking cigarettes while handling toxic chemicals like sulphuric acid or solvents could be explained as an addiction. Experience has shown that smokers of cigarettes were also fond of smoking cigarettes near urinals. Further research is, therefore, recommended to reveal the hidden behavioural motives and mechanisms common in those workers before one would think of any intervention. Behavioural change should always be planned in relation to circumstantial change and should go in stages. Conclusion This paper concludes that workers handling chemicals in small scale industries in the informal sector are in danger of compromising their health while struggling for survival by working in SSI. Mishandling of toxic chemicals can not be prevented in workers and employers in those SSI unless the level of awareness of health hazards related to handling of chemicals is increased. In addition to increase in awareness, improvement of the working conditions in terms of water supply and sanitation is important. Provision of water supply and excreta disposal facilities will improve personal hygiene as well as preventing the transfer of the hazards to the community nearby. Some of the preventive measures could only be possible if there is a policy addressing SSI in the informal sector. This policy will allocate work plots to the workers and additional support in terms of loans and occupational health services for the workers and employers. Acknowledgement The author is indebted to the management and workers of the small-scale wood for their participation. The authors thank the Research Assistants for their assistance in data collection. This study was supported by WOTRO Dissemination grant in Capacity Building Grants programme File Nr. WCD 96-216. References
© Copyright 2005 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp05011t5.jpg] [lp05011t3.jpg] [lp05011t7.jpg] [lp05011t8.jpg] [lp05011t4.jpg] [lp05011t1.jpg] [lp05011t6.jpg] [lp05011t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}