 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 2, No. 2, Oct, 2005, pp. 24-27 Epidemiology of Measles in Tanzania: A Hospital-Based Survey of Measles Morbidity and Mortality Kagoma S Mnyika1 and Caroline Akim2 1Dept. of Epidemiology and Biostatistics School of Public Health &
Social Sciences, 2Expanded Programme on Immunization Ministry of
Health Dar es Salaam, Tanzania Code Number: lp05014 Abstract Objective: To estimate measles morbidity and mortality in
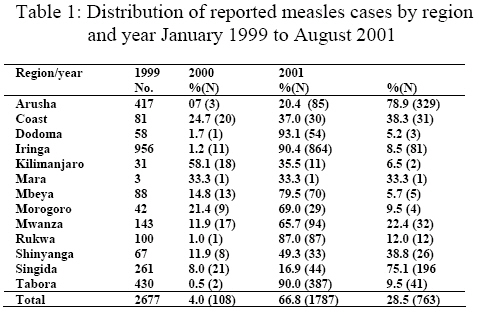
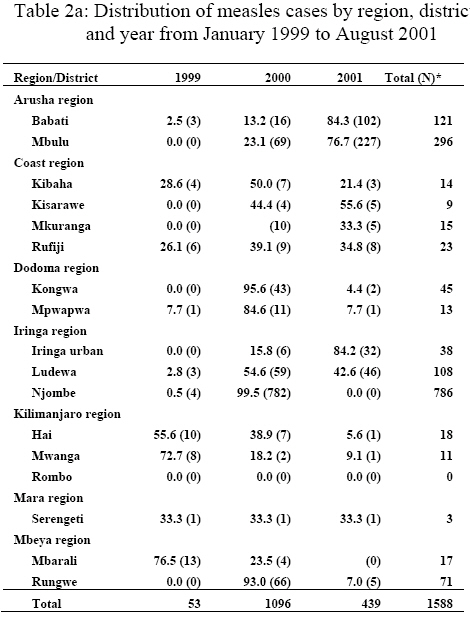
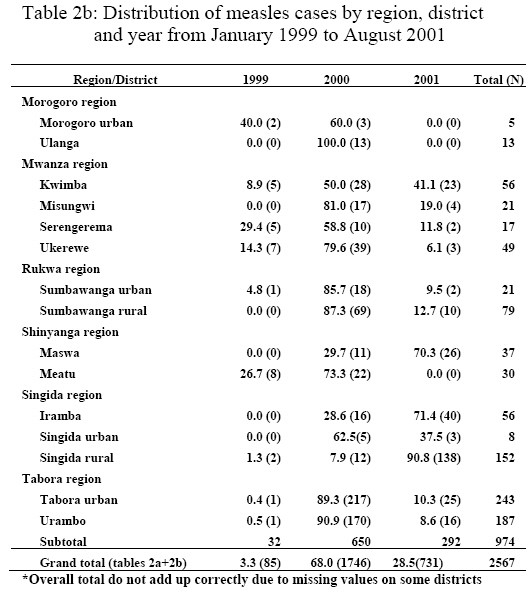
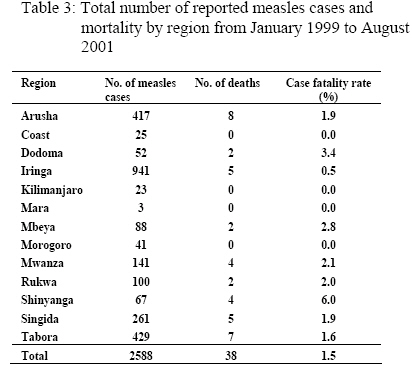
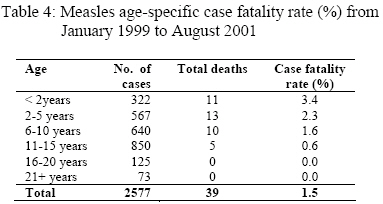
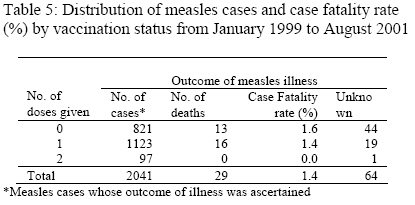
selected regions on mainland Tanzania Introduction Measles is an immunisable viral disease that affects mainly young children not only in Tanzania but also worldwide. The Ministry of Health in Tanzania has been offering vaccinations against measles to all underfive children at maternal and child health clinics for many years (1). However, during the past ten years, the Ministry of Health has been running annual mass immunisation week campaigns involving all underfive children against all major childhood immunisable diseases including measles and poliomyelitis. During the 2001 mass immunisation week, the age group eligible for measles vaccination was extended to include children up to 15 years of age. The vaccinations were implemented in 13 pilot regions on mainland Tanzania i.e. Arusha, Coast Region, Dodoma, Iringa, Kilimanjaro, Mara, Mbeya, Morogoro, Mwanza, Rukwa, Shinyanga, Singida and Tabora. The impact of this extended age eligibility for measles vaccination on measles morbidity and mortality in Tanzania had not been evaluated. It is in the light of this expanded age eligibility for measles vaccination that prompted the present study geared towards establishing baseline data for possible future measles vaccination impact evaluation among the vaccinated children up to the age of 15 years. The study covered the 13 pilot regions that participated in the campaign in September 2001. This report presents results of the survey conducted to assess the situation of measles morbidity and mortality in the said regions from January 1999 to August 2001. Methods The survey was conducted in 13 regions that participated in the pilot testing of measles vaccination up to the age of 15 years. The pilot districts were selected based on the existing information on measles epidemiology in Tanzania. The study design was a hospital-based cross-sectional study involving review of hospital records in the selected districts preferably district hospitals where records were available and also where record keeping was expected to be reliable. Information was collected using the standard questionnaire adopted from the expanded programme on immunisation unit of the Ministry of Health in Tanzania. The questionnaire consisted of 12 items namely, (1) name of region, (2) district, (3) village or town, (4) sentinel site (name of health facility), (5) month (under review) (6) year (under review) (7) in-patient/out-patient number (8) name of patient, (9) date of birth or age (if date of birth was unknown), (10) date of onset of measles rash (11) number of valid measles doses ranging from 0 to 2 and (12) outcome of measles disease (ranging from 1=died, 2=alive, 9 = unknown). Sufficient number of the questionnaire forms for 32 districts was photocopied at Muhimbili University College of Health Sciences. The project was reviewed and ethical clearance was obtained from the Ministry of Health in Dar es Salaam. Twelve (12) experienced researchers were recruited from Muhimbili University College of Health Sciences and were trained on how to fill out the forms during data collection in the study districts. Upon arrival in the respective regions each researcher recruited one member of the regional health management team (RHMT) with whom they worked together during data collection in the regions. The researchers also recruited one member of the district health management team (DHMT) in each of the districts they surveyed to assist in records retrieval during data collection. Data collection Data collection involved reviewing records in the health facilities (sentinel sites) including case notes, in-patient and out-patient registers as well as records at maternal and child health clinics. Some researchers encountered some problems when they were reviewing the records in particular information relating to number of vaccinations and date of onset of measles rash. Most doctors did not include the number of doses the patient had received before developing measles disease. The case definition of measles was taken as found in the hospital records and it was difficult to ascertain if there were any misdiagnoses. Likewise the definite date of onset of measles rashes was difficult to establish in many health facilities. Data management The completed questionnaire forms were checked and subsequently entered into a computer at the Muhimbili University College of Health Sciences. Data cleaning was carried out prior to data analysis. Descriptive data analysis was performed using statistical package for social sciences (SPSS/PC+) for windows version 12.0 (2). Of the 13 variables included in the questionnaire, only 7 variables with meaningful interpretable data were analysed i.e. (1) region, (2) district, (3) sentinel sites, (4) year under review, (5) age of patient, (6) number of valid doses of measles vaccination and (7) outcome of measles disease. The rest of the variables were not analysed either because there were too many missing data or it was unnecessary to analyse the variables. For example linking the name of patient with some other variables was considered not informative and therefore unnecessary. Results Measles cases were reviewed in 32 pilot districts selected from 13 regions on mainland Tanzania. The review process covered the period from January 1999 to August 2001. Information was available on 2677 measles cases that received treatment in the health facilities located in the study sites (Table 1). The mean age of the measles cases was 8.8 years with standard deviation (SD) of 6.0 while the median age was 9.0 years and mode 13 years. The age of the measles cases varied widely ranging from those in the age group of one year or less (≤ 1 year) to 59 years of age. The distribution of reported measles cases by region and year are shown in Table 1. As can be seen in the Table, there were more measles cases reported during the year 2000 as compared to the year 1999 and 2001. Mara region reported the lowest number of measles cases while Iringa region had the highest number of measles cases. Overall, of the 2677 cases reported in the 13 regions on mainland Tanzania during the period under review (January 1999 to August 2001), 35.7% were from Iringa region whereas only 0.1% were from Mara region in north-eastern Tanzania. In order to get an in-depth view of the pattern of occurrence of measles cases, analysis of the distribution of the measles cases by district and year was done and results are presented in Table 2a and Table 2b. Some districts appear to have experienced epidemics of measles cases over a period of three years under review while others did not. Table 2a suggests that Babati, Mbulu, Ludewa, and Njombe districts may have experienced some form of measles epidemic as compared to other districts while Table 2b shows that Singida rural, Tabora urban and Urambo districts reported a large number of measles cases compared to other districts. On the other hand, some districts during the same time period had no cases of measles reported in the health facilities. As can be seen in Table 2a and Table 2b, overall Njombe district contributed 30.6% of all measles cases reported in the 32 districts. The top ten districts in the reported number of measles cases were Njombe, Mbulu, Tabora urban, Urambo, Singida rural, Babati, Ludewa, Rungwe, Sumbawanga rural, and Kwimba districts. Table 3 shows estimates of case fatality rate by region from January 1999 to August 2001. As can be seen in the table, there were no deaths due to measles reported in the Coast Region, Kilimanjaro, Mara, and Morogoro regions. However, in the regions where measles disease mortality occurred, Shinyanga region experienced the highest case fatality rate followed by Dodoma region. Case fatality rate ranged from 0 to 6% in Shinyanga region. Table 4 presents results of analysis of case fatality rate by age. The table shows that case fatality rate was highest (3.4%) among young children aged less that 2 years of age and decreased with increasing age of the measles cases. There were no deaths reported among patients older than 15 years of age. Table 5 shows the summary distribution of reported measles cases, case fatality rate and vaccination status in the 13 regions on mainland Tanzania from January 1999 to August 2001. As can be seen in the table, case fatality rate was highest among patients with history of not being vaccinated against measles as compared to others. There was no death recorded among patients who had received two doses of measles vaccine. The outcome of sixty four patients could not be established. Although not shown in the table, the distribution of measles case fatality rates in districts ranged from 0 to 11.8%. Of the 32 districts surveyed, Mbarali district recorded the highest measles case fatality rate (11.8%) followed by Sumbawanga urban (9.5%), Maswa (8.1%), Mpwapwa (7.7%) and Iramba (5.4%) district in that order. Discussion The data presented in this communication were collected from health facilities in 32 districts of mainland Tanzania. The data are hospital-based and may not reflect the actual measles epidemiology on mainland Tanzania. Studies have shown that hospital-based measles case fatality rates are not representative of measles mortality in the community (3). However, since the number of districts surveyed was fairly large (from 13 regions out of a total of 20 regions), we believe that the data presented in this paper are the best estimates of measles morbidity and mortality on mainland Tanzania. The results indicate that although measles is mainly a disease of childhood, there were some individuals who suffered from measles beyond 15 years of age and others up to the age of 59 years which was consistent with findings reported from elsewhere (4-6). This observation suggests changing pattern in the epidemiology of measles in Tanzania. According to our data, measles appear to affect people in the adolescent age and beyond suggesting the need to re-examine the current immunisation schedules in Tanzania. Therefore the Ministry of Health decision to extend the age for immunisation up to 15 years in 2001 was justified. However, there is need to carry out a follow up evaluation survey to assess the impact of the measles vaccination conducted in 2001 on measles morbidity and mortality in the pilot sites before contemplating on changing the current immunisation schedules in Tanzania. The reason for this viewpoint is that the optimal age for measles vaccination has been a subject for debate among vaccine experts for many years (1,7-13). The recommended optimal age for measles vaccination in Tanzania has been 9 months for many years (1). This recommendation was based on the decline of maternal measles antibodies in the babies to a level that measles vaccination produces protective antibodies in the children. A large proportion of children tend to suffer from measles if vaccination is delayed beyond 9 months. On the other hand measles vaccination administered before this age did not offer protection as maternal antibodies have not disappeared or declined significantly. Therefore the trade-off between age at immunisation and persistence of maternal antibodies in children needs to be considered carefully. The occurrence of measles cases seems to suggest an increasing trend over time in Arusha, Coast and Singida regions while in other regions there was no definite trend in the number of measles cases over the three year period. The occurrence of measles cases in Arusha, Dodoma, Iringa, Singida and Tabora regions during 2001 seemed to have reached epidemic proportions in populations believed to have high measles immunisation coverage. Nonetheless the occurrence of measles cases in populations with high immunisation coverage was consistent with findings reported from other studies (5). The findings suggest that immunity following measles vaccination may have waned to the extent that the heard immunity of the population was very low and therefore rendered the populations susceptible to measles outbreak (14-16). Concerning mortality, some regions experienced high mortality due to measles compared to other regions. The highest measles case fatality rate was observed in Shinyanga region followed by Dodoma region (6.0% and 3.4% respectively). Age-specific case fatality rate was highest among young children below 2 years of age while no mortality occurred among patients aged 15 years and above. This finding was expected as young children have immature immune system compared to older population and are therefore susceptible to severe form of measles disease. Further exploration of measles-related mortality indicated that case fatality rate was highest among patients who were not vaccinated compared to those vaccinated. This observation was expected and was consistent with findings reported from elsewhere (17-20). Unvaccinated individuals tend to develop severe form of measles and are more likely to succumb to the illness compared with vaccinated individuals. Indeed none of the patients who had received two doses of measles vaccination died from measles disease. Conclusion We conclude that despite high vaccination coverage, measles is still occurring in all regions and poses a great challenge to public health in Tanzania. Measles occurs in previously vaccinated populations and also among persons above 15 years and beyond. This calls for re-examination of the current vaccination schedules in order to cater for the changing pattern in the epidemiology of measles in Tanzania. Acknowledgements We wish to convey our gratitudes to the research team that participated in data collection from 13 regions on mainland Tanzania. This project was supported by a research grant from the Expanded Programme on Immunisation of the Ministry of Health, Tanzania. References
© Copyright 2005 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp05014t5.jpg] [lp05014t1.jpg] [lp05014t2b.jpg] [lp05014t3.jpg] [lp05014t2a.jpg] [lp05014t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}