 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
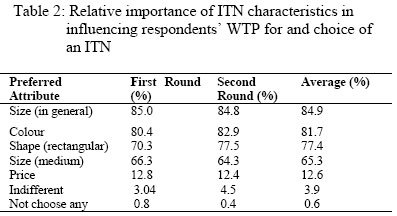
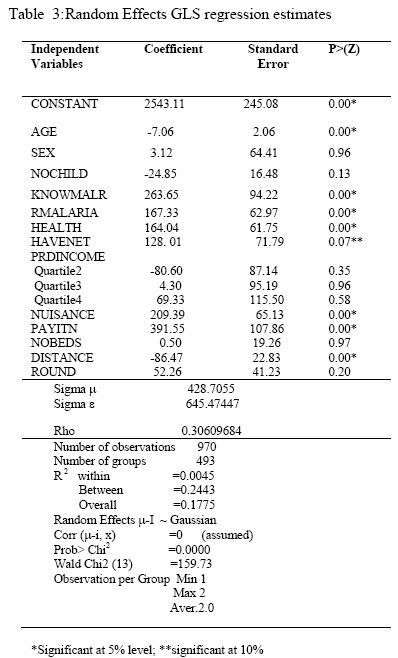
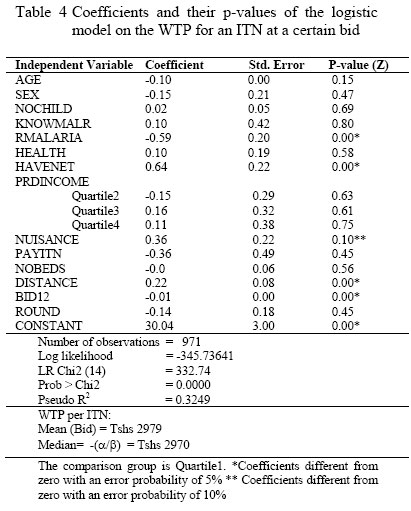
East African Journal of Public Heath, Vol. 3, No. 1, April 2006, pp. 17-23 EXPLORING DETERMINANTS OF CONSUMER PREFERENCES AND WILLINGNESS-TO-PAY FOR INSECTICIDES TREATED BEDNETS BEFORE INTERVENTION IN A POOR RURAL TANZANIA Phare GM Mujinja Corresponding author: Phare G.M. Mujinja, P O Box 65015, Muhimbili Health College of Health Sciences Dar es Salaam, Tanzania Dept. of Public Health and Social Sciences Code Number: lp06004 Abstract Objective: To explore commodity and human factors associated with willingness to pay (WTP) and consumer preferences for insecticides treated bed nets (ITNs) prior an intervention Key Words:Contingent valuation, willingness to pay, insecticide treated bed nets, malaria, rural poor, Tanzania Introduction One of the recommended key malaria control measures is the use of bed nets, especially the treated ones. It is undoubted that the untreated mosquito bed nets are widely available in Tanzania; and it is estimated that 40% of all Tanzanians use some kind of a mosquito net (1-2). On the contrary, even with the fact that Insecticide Treated Nets (ITNs) have been shown to be clinically efficacious in significantly reducing malaria mortality and morbidity (3-5), are 'a rare commodity' (6), and not necessarily affordable to most people in the rural areas despite the introduction of the voucher system (7-8); and it is currently estimated that only 11% of pregnant mothers and 8% of children under five years of age use ITNs (2,8). Although promotion of demand for ITNs is a key component of malaria control strategy in Tanzania (8), the possession of ITNs, even in some areas where they have been socially marketed, remains very low (1-2,6-7). Affordability is mentioned to be one of the main reasons for the low possession (6, 7, 9-10). The introduction of the voucher system, which targets pregnant women and children under five years of age as vulnerable groups, aims at promoting the potential demand of ITNs (8). However, the demand and eventually the possession of ITNs does not only depend on the aggressiveness of the promotion messages, but also, among other things, the willingness to pay (WTP), which also depends on ability to pay and the characteristics of both the individual and the commodity to be demanded, ITN (6, 9-13). Since the distribution of the WTP for ITNs is relatively unknown in most areas in Tanzania, the analysis of the willingness to pay for ITNs, therefore, becomes an important ingredient in promoting demand for ITNs, especially in areas where the people are relatively poor and the commodity is relatively ‘new’. Most of the ITNs trials and projects undertaken in Tanzania have either supplied free nets or sold nets and insecticides at subsidised prices and some have distributed ITNs, using the private sector where nets and insecticides are sold at subsidised prices to stimulate demand (5, 7). The voucher system sells subsidised ITNs to vulnerable groups through private agents, and some projects have also given special vouchers to vulnerable groups (2,7). However, even with provision of targeted subsidised vouchers, due to economic factors such as willingness and ability to pay for an ITN, there is evidence that some individuals cannot take advantage of such subsidies (7), some places the targeted populations buy the subsidised nets and re-sell them for more money and the coverage of ITNs drops after the trial teams have left the field (10). Previous studies in other countries have explored ability to purchase nets and factors that would hinder the actual use of ITNs, but only a few studies have examined individual and net characteristics that would influence willingness to pay (WTP) before the intervention is underway (13, 10). Most studies in Tanzania have looked at willingness to pay for ITNs when the interventions are underway (7) and, and sometimes these studies have been triggered by the slowing down of the demand (1, 7). Such studies suggest that WTP for, and factors associated with ITNs, need to be assessed and understood before interventions are implemented. They also indicate a gap between the understanding of local people and the scientific explanation of the success stories of ITNs: that, ITNs reduce mortality and morbidity of mosquito related diseases. The fact that ITNs are relatively “new” commodities to people outside the trials and projects communities means that scaling up the ITN interventions requires district specific information about market structure and conditions that affect ITN purchase (11), especially when people have to pay for ITNs. WTP values are elicited using a contingent valuation (CV) technique, where a hypothetical scenario of the intended commodity is presented to the respondent who thereafter responds to the questions related to valuation of the commodity. Discrete (take-it-leave-it and bidding game) and continuous (open-ended and payment card) methods are used to elicit the values-maximum amount of money (WTP) that an individual would be willing to part with to obtain a commodity. Although the CV method sets out to find the theoretically correct measures of economic benefit, some economists doubt if the measures obtained actually correspond to the individuals true WTP (14). However, more rigorous studies show that many of the alleged problems of CV studies (for instance, presenting a realistic scenario, clear demonstration of the good, conducting focus group discussions and pilot surveys before the main survey), can be resolved by careful study design and implementation, by using recently developed guidelines that have greatly improved the design, analysis and interpretation of surveys (6, 13, 15-16). CV studies have been found to be potential and valid in predicting the direction of actual WTP for the ITNs, where stated WTP was found to be translated into actual WTP (17), for exploring affordable ITN prices (6,11-13,18), and also reported to be useful in providing important information for health programme planning before scaling-up an intervention (6,17). Since ITNs are an important part of the Tanzanian malaria control strategy it is imperative that specific district information on the factors that may affect their demand be explored a priori. In the present study we explored factors that would influence WTP for an ITN, before the intervention to generate information that could be used for establishing prices that would not discourage demand, designing district-specific social marketing messages and sustainability of ITN interventions. We explore individual and household characteristics that are likely to determine the willingness to pay and consumer preferences and mean and median WTP prices for an ITN. The gap of understanding of factors that would limit WTP for ITNs in a poor rural area explored using both an open-ended (OE) and discrete choice formats. The OE and discrete choice methods were used to elicit WTP because they were easily followed by the respondents who more than 30% could not read and write. Materials and Methods Study site: Two rounds of data collection study (test-retest), of two weeks interval, were conducted in Kisarawe District in Tanzania between September and November 2001. The district was chosen because ITNs had not been introduced in the district, as it was done elsewhere (17, 19). Residents of Kisarawe district with a per capita income of about $ 150 depend mainly on subsistence farming for their living. The District, which is divided in four Divisions, has two main rainfall seasons, the short rains (between October and January) and the long rains (between March and June). Kisarawe district with a population of around 130,000 people has an average household size of 5.4 people with a literacy rate of less than 65%. Malaria is the main cause of outpatient and inpatient attendance. It is also the major cause of mortality (20). Sample According to Lwanga and Lameshow (21) a minimum of 474 respondents were to be included in the study. A multi-stage cluster sampling technique was used to select respondents. From the four divisions, one village was randomly selected, and 120 - 126 households were randomly selected from each village’s list of households. The household head was asked to participate in the study, and in the event that he or she was not available during the period of interview, another adult household representative was asked to participate in the survey. A total of 501 respondents were selected from the four villages. The survey instruments were administered over two rounds of two weeks interval to the same respondent. A total of 491 (98%) respondents were available to respond to questionnaires in the second round, and there was no replacement in the second round Instruments design and Data Collection Twelve Focus Group Discussions (FGDs) were conducted in villages, which were not among those selected for the main survey. Three groups from each village: youths (18-25) women of childbearing age (15-49 years) heads of households (26 years and above). The major topics discussed included major health problems in the village, knowledge on malaria transmission, prices of nets, knowledge of on ITNs and use of bed nets. The results of FGDs were used for revising the questionnaires before the pre-test survey was conducted. All research instruments were pre-tested before the main survey was undertaken to validate the content and logic of the questionnaires. Results from pre-test and observed normal net market prices from the local shops were used to adjust all section of the questionnaire and the amounts of money that were to be presented to the respondent. FGDs results showed that Tshs 2900 (USD 3.20) would be the average amount considered affordable by most residents and Tshs 3500 (USD 3.90) as the maximum amount. The CV instrument had three parts. The first part, of the instrument was administered only once, in the first round, with the assumption that such characteristics would not significantly change in two weeks interval. This part asked about the socio-economic characteristics of the respondent and other household members’ health status, knowledge on malaria transmission, and current and past expenditures on malaria treatment and prevention, use of untreated bed nets and ITNs, and household wealth. The second part of the instrument presented the contingent valuation hypothetical ITN scenario and, in addition, an ITN and an insecticide sachet were physically presented to the respondent as done in Nigeria and Ethiopia (17, 19), before the related questions were asked. The third section of the instrument, referring to the second part scenario, presented the different attributes of ITNs, including shape, prices, colours, size and make. The respondents were asked, after giving a verbal consent, whether they would purchase an ITN at one of the three randomly assigned prices. The lowest price was Tshs 2900 and highest price Tshs 3500, based on the FGD results. All respondents, regardless of their answer to the discrete choice question, were there after asked follow-up questions: “why” they answered the way they did, how many ITNs for themselves and if they would be willing to purchase one for any other household member. The two methods were chosen because more than 30% of the people in the district were illiterate: the inclusion of the why question was important to understand the reasons behind the willingness or unwillingness to pay for an ITN. Thereafter, another follow-up open-ended (OE) question was asked, regarding the maximum amount the respondent would be willing to pay. It is assumed that a respondent would not be willing to pay for an ITN if he/she had had a disutility for it, hence zero would be the maximum WTP allowed. The follow-up and the maximum amount questions were also used to differentiate “true” and “protest” zeros. If the responded answered “no” or “I don’t know/uncertain” to the question and gave zero as the maximum WTP, then the “why” was used to analyse the zeros. Two possible zero responses were regarded as “true” zeros, if the response to the why question was: “I do not need a mosquito net”, “I have a mosquito net” and /or “I cannot afford a mosquito net”. The disadvantage of this method is that the respondent’s response on the OE question was likely to be influenced by the response given in the discrete choice questions. However, it was found that, if a respondent has already responded “yes” to a discrete choice question was not likely to mention a maximum amount lower than the amount presented in a discrete choice question. Respondents were further asked to make a choice (preferences) among different combinations of characteristics of mosquito nets that they would be willing to pay for at one of the above prices. Thereafter, they were asked to give the reason of their choice. Data Analysis: We used two regression models on the pooled data to estimate coefficients and analyse factors that influence WTP for an ITN: The generalised least squares random effects model (REM) for quantitative dependent variable and the logistic regression model (LM) for the discrete choice question, both estimated using the maximum likelihood procedures (22-23). Both models were estimated using STATA 7 programme, which was also used to check for heteroscedasticity and multicollinearity: highly correlated variables were dropped from the models to arrive at specific (reduced) models. Observations that influenced the models were isolated by Cook’s method (23) Multicollinearity was checked using the Variance Inflation Factors (VIF). The mean VIF was 1.1 suggesting that multicollinearity was not a serious problem (22). A few outliers were identified and isolated using the scatter-plot matrix and box-plot (23, 24). Finally, a total of 971 observations are used for estimating the regressions. Results Descriptive Statistics A total of 501 and 491 (98%) respondents were interviewed in the first and second rounds respectively. Full information of 485 (96.8%) respondents was available, for both rounds of interview. About 51% and 49% of the respondents were male and female respectively. The household size was about 5.3 people with an average of one under five in each household. More than 85% were subsistence farmers. About 67% had at least a primary school education. Malaria was reported by about 90% of the respondents as the most prevalent disease in their communities. Only about 19% of the respondents owned a mosquito net, however, about 95.7% reported to regularly using different types of mosquito repellents. Table 1 gives an overview on the variables used in estimating the models. The majority of the respondents (86%) knew how malaria was transmitted. Thirty two percent reported to have had suffered from malaria in the three months prior to the interview. About 40% rated their health as good compared to other people in their communities. The average weekly per capita expenditure of food and other consumption goods was about Tshs 900 (about 1 USD). Sixty seven percent found mosquito bites to be a nuisance and 92% rated themselves as able to buy a net (at undisclosed price) if made available. The average number of beds used by household members was 3.7. Many of the respondents lived closer to a health facility. The net prices ranged from Tshs 2900 to Tshs 3500. Relative Importance of Mosquito nets attributes on Consumer Preferences: Table 2 shows the relative importance of mosquito net attributes in influencing WTP for an ITN as mentioned by respondents by rounds of the survey. The size of a mosquito net was frequently mentioned (85%). Different sizes were presented and the most preferred size of a net was the `medium size, a 4-feet-net mentioned by 65% of respondents. The second most important attribute was the colour (82%), and the most preferred colour was blue (52%) and least preferred were white (7.7%) and red (6.6%). Only two shapes of nets were presented, the rectangular and round shapes. The most preferred shape was the rectangular and was mentioned by 77% of all respondents. The price of the net, as a factor that would motivate them to be willing to buy a net was only mentioned by approximately 13% of all respondents. A majority (80%) of those who mentioned the price mentioned Tshs 2900 and Tshs 3000 and the rest where respondents who said would not afford to buy a net at any of the prices presented. Regression estimations: Table 3 presents the estimates of the Random Effect Model coefficients applying the Generalized Least Squares (GLS), random effects estimator. The Table shows that age of the respondent (AGE) and coefficient on DISTANCE had a statistically significant negative impact on respondents mentioning a higher maximum WTP (P<0.05). A recent experience with a malaria episode (RMALARIA), being aware of how malaria is transmitted (KNOWMALR), self reported health status coefficient (HEALTH) and self assessment of being able to buy an ITN (PAYITN) and perceiving mosquito bites as a nuisance, (NUISANCE), were positively statistically significantly associated with mentioning a higher maximum WTP (P<0.05). Having an untreated bed net (HAVENET) had a positive marginal impact on both mentioning the maximum WTP (P=0.07). Table 4 presents the estimates from the logistic model, the probability of giving an affirmative response. The Table shows that the coefficient on a recent experience with a malaria episode (RMALARIA) had a statistically significant negative impact on the likelihood of a “yes” response to the discrete choice question (P<0.05). This could be due to lack of experience of using a bed net or because of they had suffered repeated episodes that have been successfully cured and no need to worry about the disease. Having an untreated bed net (HAVENET) and distance to the nearest health facility (DISTANCE) had a positive statistically significant impact (P<0.05). Perceiving mosquito bites as nuisance, (NUISANCE), marginally predicted the probability of giving an affirmative response to a WTP question (P=0.1). A negative and highly statistically significant value (P<0.05) for the coefficient on the price of an ITN variable (BID12) indicate that the probability of giving an affirmative response (“yes”) to the requested bid falls as the bid rises, as expected. This is inline with economic theory of consumer behaviour. Mean and Median WTP Estimates: The mean and median distributions for both rounds were estimated by a simple calculation, nonparametric method and from the logistic bid function. The mean from the maximum WTP was Tshs 2829 and 2802 for the first and second round respectively, while the median was Tshs 2900 for both rounds respectively. The mean estimated using the nonparametric method was Tshs 2945 and 2968 for the first and second rounds respectively, while the median was Tshs 2934 and 2957 for the first and second rounds respectively. The mean and median from the logistic bid function were estimated as Tshs 2979 and 2970 respectively. Discussion The new consumer theory (25) advocates the importance of commodity characteristics in determining demand for a commodity. The results of our study support this new theory by suggesting that even with ITNs, commodity characteristics or attributes are important factors in determining the respondent’s WTP. Apart from mere characteristics which have also been reported in different studies (6, 25, 26, 27, 28), in our study we explored more the relative importance of these attributes when analysed together. Some ITN attributes (colour, shape, size and price) dominated other attributes for choices that were made. Even within one attribute, say colour, blue and green colours of a mosquito net were relatively more important in determining the choices than other colours. Individual tastes for a commodity that influence choice for a commodity may be different in different communities (25), even in the same country depending on, among other things, differences in socio-cultural and economic contexts. In this study, reasons for choice of different attributes were mainly environmental and economical: the colour of an ITN does not easily show dirtiness; matches the land physical environment and cannot afford to wash the ITN regularly; and soaps are expensive. This indicates that in communities where ITNs are “new” commodities, before the intervention is underway, information on consumers’ tastes for the commodity have to be explored to maximise future potential demand. Lancaster (25) in his new approach to consumer theory observed that consumers are not only interested in goods as such, but greatly in their attributes, suggesting that the most preferred ITN attribute would be of more relative importance than others in determining individuals’ WTP for an ITN. In north-western Burkina Faso, prior to the establishment of local ITN programme, respondents reported to be willing to pay for an ITN if the prices offered, as an attribute of an ITN, would be reduced (26), Furthermore, the success of the Kilombero Valley project (7), although the project did not investigate WTP before the intervention started, was largely explained by the use of social marketing research surveys that helped to identify the most suitable brand attributes preferred by potential consumers. In addition our results show that among other factors, nuisance due to mosquito bites, not necessarily that of malaria, significantly influenced WTP. Existence of mosquito nuisance, other things being equal, signals for an existence of a potential market for ITNs, which could be probably limited by the ability to pay as found in Kenya (11). However, the most important part in malaria control is to get people to sleep under an ITN. The expression of the individuals’ utility function is the most important issue, how it is expressed is upon the individual consumer. Understanding what individuals value as the most important attributes of a bed net, like avoid mosquito nuisance, which would influence willingness to pay for a bed net, and using such information to create social marketing messages, creates favourable grounds for attracting consumers to accept the intervention than using what scientists value most, like reduction of malaria cases. Besides, in the process what the community values most results in reduction of malaria cases, which is the scientifically expected end outcome. Apart from the commodity attributes, the individual consumer’s perception of risk on use and effect of the commodity on the expected outcome compared to other alternatives has an implication on WTP. Our proxy measures of risk, a recent experience with a malaria episode and self rating health status, had a great impact on WTP. Onwujekwe et al (12) when evaluating who buys ITNs in Nigeria found that respondents who had a recent attack of malaria were also more likely to have had bought nets, when nets were sold. This would imply that the WTP and use of ITNs, among other factors, is also based on the on the uncertain hazard outcome (malaria) and not only perceived known hazard (the mosquito bite). Most of individual and household factors that were found to be associated with WTP like, knowledge on malaria, nuisance, price and age, have been reported by other studies in Africa to be associated with use or non-use of ITNs (25, 26). The fact that these studies looked at the use, after an ITN has been purchased, implies that such local information was not used in planning before the implementation of the intervention, but probably in adjusting it, and also did not take into account people who did not buy an ITN. Conducting the study prior the intervention does not suffer from such disadvantages of uncovering unmet needs after the intervention is underway. Both having an untreated net and self-assessment of individuals ability to pay for an ITN if made available, as proxy measures of ability to pay, were statistically significantly associated with WTP. These findings suggest that “well-off” households are more likely to be able to buy an ITN, if made available. Higher socio-economic group was also a significant positive factor in predicting willingness to pay for an ITN in Nigeria (12). However, on the other hand, it is argued that ITN demand is not highly responsive to lower prices if household preferences are held constant (11), and this could be explained by the inability to pay and less access to cash among most poor rural African communities (11, 28,29). In this study we find the mean and median WTP prices, for both elicitation methods, to be lower than the average of the prices presented to the respondent. Such results imply that although people would be willing to pay, only few would be able to pay at the market price. It could also be due the methods used, however, the discrete choice method have also been found elsewhere to be easily used in poor areas with low literacy rate and income instability (30). Our results also imply that different consumer’s preferences and opportunities may be influencing WTP differently depending on the approach used to present the scenario and elicit WTP values. The results in this study indicate that using more than elicitation format gives more valuable information on factors that would affect WTP. However, they may also reflect a complexity in interpreting the results. Thus, results that are obtained from different contingent valuation approaches in the same survey, even from different samples, should be compared with caution as we might be comparing two different cognitive processes that are affected by different factors.. This study interviewed the respondent twice, with an interval of two weeks. The responses between rounds of interview were not statistically different implying that the information on WTP more “reliable”, and indicate that first interview rarely, influenced the second one. In the literature, we did not come across a WTP study that has re-tested individuals WTP responses without selling ITNs. However, the validity of our measurements and the level of influence of the factors on WTP from our study would have been proved further if ITNs were to be sold after the WTP survey. But, in a separate analysis (9), we show that about 75% of the respondents were able to reproduce the same responses in the second round of the survey. Also, it has been found that hypothetical WTP studies are highly valid in predicting more than 75% of the actual sales of ITNs in Nigeria (12), and also respondents that stated higher WTP amounts before the intervention were more likely to purchase nets (17). Conclusion Individual, household and commodity related characteristics are likely to be important in influencing WTP, and consumer preferences for ITNs. The ITN characteristics have different relative importance in influencing WTP, and such information would help planners to understand the type of ITNs people would like buy and at what prices. The average prices found in this study were a bit on the lower side compared to the average of prices presented to the respondent, suggesting that if ITNs are sold at the market price only few people would afford them. Subsidies, that are compared to the mean or median prices, should be considered as a way to stimulate demand of ITNs in such poor areas. Factors that are associated with WTP and consumer preferences need to be known before the intervention is underway, for designing strategic social marketing messages for marketing ITNs, Furthermore, for a successful implementation of ITN interventions, community specific information on the market structure has to be explored We found reliable results by test-re-test design we used, however, further operational studies are required in the study area to corroborate stated preference (hypothetical market) results and the revealed preference (actual sale), as soon as ITNs are introduced in the study area. Acknowledgements The research underlying this manuscript was sponsored by Muhimbili University College, University of Dar es Salaam in the framework of collaborative graduate research grant from SAREC, Sweden. We thank David Dunlop, Lilani Kumaranayake, Rainer Sauerborn, Wilson Bhukoli and Hengjin Dong for their insightful and constructive suggestions on earlier drafts of this manuscript. References
© Copyright 2006 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp06004t4.jpg] [lp06004t3.jpg] [lp06004t1.jpg] [lp06004t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}