 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 3, No. 2, October 2006, pp. 14-18 ASYMPTOMATIC PARASITAEMIA AND PLACENTAL MALARIA INFECTION AMONG PREGNANT WOMEN IN KIGOMA URBAN DISTRICT, WESTERN TANZANIA Kagoma S. Mnyika1, Titus K. Kabalimu2 and Godfrey Mbaruku3 Correspondence to: Kagoma S. Mnyika, P.O.Box 65015, Muhimbili University College of Health Sciences, Dar es Salaam, Tanzania E-mail: kmnyika@muchs.ac.tz 1Dept. of Epidemiology and Biostatistics, School
of Public Health & Social Sciences Code Number: lp06010 Abstract Objective: To determine the
magnitude of malaria infection and anaemia among pregnant women in Kigoma
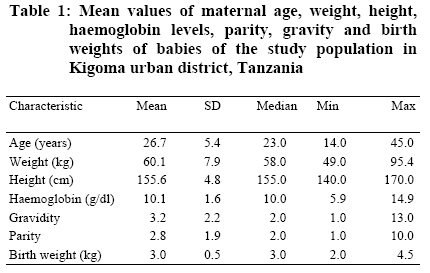
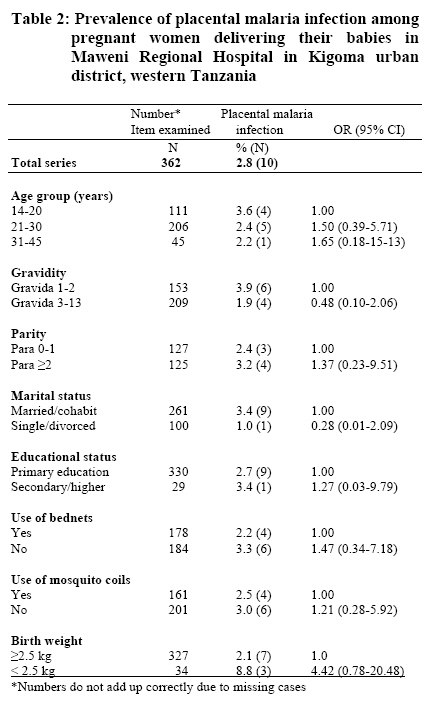
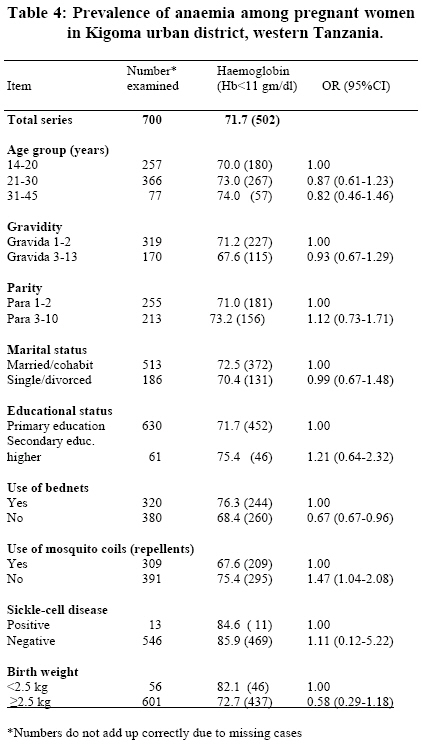
Municipality, western Tanzania. Introduction Malaria continues to be an important cause of morbidity and mortality in sub-Saharan Africa particularly among young children and pregnant women. Malaria in pregnancy is a common cause of maternal anaemia, low birth weight, abortion and still births (1-4). Recent data from the Gambia indicate that malaria alone may account for up to 93 maternal deaths per 100,000 live births in that country and the majority of the deaths are due to anaemia caused by malaria (5). It has also been suggested that anaemia might be associated with low birth weight (6). However low birth weight might be due to malaria-induced pathological lesions that occur in the placenta leading to intrauterine growth retardation (7). This may occur following placental malaria parasitisation which is common in P.falciparum infection in pregnant women who live in malaria endemic countries (8). Placental malaria poses a great challenge in malaria control strategies in that it may occur in asymptomatic parasitaemic as well as aparasitaemic pregnant women (9). Studies have shown that parasitized erythrocytes tend to sequester in the placental capillaries leading to hypoxia, inflammatory reactions and chronic intervellitis (10). Therefore, while the placentae of infected pregnant women may be full of parasitised erythrocytes, with parasite densities sometimes in excess of 50% of the total placental erythrocyte count, the peripheral blood may remain free of parasites (11). Consequently, interventions directed towards symptomatic parasitaemic pregnant women may leave out those who are equally at risk of anaemia and low birth weight. Information on anaemia in pregnancy and its impact on infant mortality in Tanzania has recently been documented (12). On the other hand, the effect of anaemia in pregnancy, asymptomatic malaria as well as malaria infection of the placenta on pregnancy outcome have not been well documented in Tanzania particularly in the wake of malaria drug resistance (13). Kigoma region situated in western Tanzania is among the hard-to-reach regions with huge health problems including maternal health services. Owing to the logistical issues inherent in conducting studies in western Tanzania, little is known about the magnitude of health problems in that part of the country. The present study was part of a larger study that aimed at determining the effectiveness of alternative malaria chemoprophylaxis in pregnancy. In this paper we present data obtained from one component that aimed at measuring the magnitude of asymptomatic malaria in pregnancy, placental malaria parasitisation and anaemia in an area of perennial malaria transmission in western Tanzania. Participants and Methods Study site and population The study was conducted in Kigoma urban district in a maternal and child health care clinic (MCH) located in the centre of Kigoma municipality approximately 100 metres from the Kigoma railway station. Owing to its central location in the town, the Kigoma MCH clinic handles approximately 1,350 pregnant women per year. Kigoma municipality is a port on the shores of Lake Tanganyika in western Tanzania and has a population of 144,850 inhabitants (14). The port handles passengers and cargo vessels to Burundi and the Democratic Republic of Congo. Malaria transmission in Kigoma municipality is perennial with peak transmission between November and April which is the rainy season with optimal temperatures for mosquito vector breeding. Ethical clearance and data collection The study was reviewed and cleared by the Ethical Clearance Committee of the Muhimhili University College of Health Sciences. Following ethical clearance of the project, investigators went to start preparatory work with the Kigoma regional health authorities in September 1992. The project was accepted and the work began in October 1992. Research assistants were recruited from Maweni Regional Hospital and comprised of two senior nursing officers and one senior laboratory technologist. The field team was fully trained on all procedures that were used to solicit for valid informed consent including correct enrolment procedures of the pregnant women as well as on questionnaire administration using standard operating procedures (SOPs) that were developed for the study. The questionnaire consisted of items focusing on socio-demographic characteristics (i.e. age, marital status, and educational level) of the pregnant women as well as parity, gravidity and use of malaria preventive measures (bednets and mosquito coils). After completion of the questionnaire, the women were then randomised to different malaria chemoprophylaxis regimens as described in detail in our earlier communication (15). Laboratory methods All the laboratory investigations needed for the study were undertaken in accordance with the standard operating procedures that were developed and agreed upon by senior medical laboratory technologist at Maweni Regional hospital in Kigoma and the principal investigators. The senior medical laboratory technologist was responsible for taking thick and thin blood slides for malaria parasites at recruitment and subsequent follow up visits. The slides were prepared using the standard Giemsa staining procedures and microscopic examination was done counting malaria parasites per 200 white blood cells (including species identification). One hundred high power fields were read to confirm a negative film. In addition, blood samples were taken for full blood picture including haemoglobin (Hb) levels (in grams/dl), haematocrit and sickling test for sickle-cell disease. Other specimens taken from the pregnant mothers were stool and urine for detection of blood depleting parasitic infections including hookworm, Ascaris lumbricoides, Schistosoma haematobium, Schistosoma mansoni, Strongyloides stercoralis, Trichura trichuris, and so on. At the time of delivery in the labour ward, thick blood films were prepared also using the standard Giemsa staining procedures and examined microscopically for evidence of placental malaria infection (parasite count per 200 WBC). Newborn babies were also weighed immediately after delivery in labour room by two nurses and weights were recorded to the nearest 10 grams. Informed consent and enrolment procedures Before enrolment into the study all potential participants were given complete information on the purpose and expected procedures involved in the study. Technical information was given using simplified language that could be easily comprehended by the pregnant women. The women were also given chance to ask questions in areas that they did not understand. The women were also told that participation was voluntary and that refusal to participate in the study would not have any effect on the quality of health care offered to them at the clinic. Moreover, the women were informed that they were at liberty to withdraw from the study at any time if they wished to do so. Those who agreed to participate were then registered and asked to proceed to the antenatal clinic where a questionnaire was administered and the investigations taken as part of the routine antenatal care services provided at the clinic. All consenting pregnant women who were under 18 years of age were requested to have their informed consents ratified by their parents, guardians, neighbour or husband (if the husband was 18 years and above). At the time of delivery, informed consent was also sought to take blood films from the placentae for microscopic malaria examination and once again the women had the liberty to refuse taking blood slides from their placentae. Data management & analysis Data entry and cleaning was performed at the Muhimbili University College of Health Sciences and was completed in November 1995 using the Statistical Package for Social Sciences (SPSS/ PC+). Data analysis was conducted using SPSS for windows version 12.0 (16). Prevalence of placental malaria infection by socio-demographic characteristics was analysed using binary logistic regression analysis and differences were tested using odds ratios (OR) and 95% confidence intervals (95% CI). Birth weights of babies were categorised into two groups namely low birth weight babies defined as newborn babies weighing less than 2.5 kg and normal newborn babies weighing 2.5 kg or more. Associations of asymptomatic malaria parasitaemia with other maternal characteristics were analysed using logistic regression and differences were tested using OR and 95% CI. As the majority of the women were recruited at 21 weeks of gestation which is the critical period for foetal growth (13), the analysis of the association between asymptomatic malaria parasitaemia with other maternal characteristics is based on results obtained at recruitment. As the World Health Organisation defines anaemia in pregnancy as haemoglobin levels of 11 g/dl or less (17), the cut-off point used for anaemia was haemoglobin (Hb) level below 11 grams per decilitre. Results A total of 729 pregnant women were recruited into the study and participated into the interview and of these 705 (96.7%) agreed to participate in the follow up study. Of the 705 who agreed to participate in the followed up study, 33 (4.8%) dropped out of the study because they had to move to other regions for various reasons including joining their husbands. At the time of delivery, only 54% (N = 672) of the women agreed to have their placentae examined for malaria parasites. Table 1 summarises descriptive data relating to the study population. As can be seen in the table, mean age of the women was 26.7 years with the youngest pregnant woman being 14 years while the oldest was 45 years of age. The mean birth weights and maternal heights are also presented. Table 2, presents prevalence proportions of placental malaria by various socio-demographic characteristics among the pregnant women studied. The overall prevalence proportion of malaria infection of the placenta in the study population was 2.8%. Although not statistically significant, placental malaria infection was more common among women in the age group 14-20 years. Similarly, placental malaria infection was common among women carrying their first or second pregnancy. However, the opposite relationship was observed between malaria infection of the placenta and parity whereby placental infection was higher among para 2 or higher. Women with placental malaria were more likely to deliver low birth weight babies than those without placental infection (OR = 4.42, 95% CI 0.70, 20.48). Table 3 summaries the association between asymptomatic malaria with socio-demographic characteristics of the pregnant women. As can be seen in the table, the overall prevalence proportion of asymptomatic malaria parasitaemia was 8.4% (N = 705). There was no association observed between the prevalence of asymptomatic malaria with age, gravidity, parity and marital status. Although not statistically significant, pregnant women with secondary education or higher were less likely to have asymptomatic malaria than those with low education (OR = 0.34, 95% CI 0.04, 1.36). Women who reported not having used mosquito bednets and mosquito coils were more likely to have asymptomatic malaria parasitaemia compared to those who reported using bednets and mosquito coils. Table 4 presents prevalence proportions of anaemia by age, gravidity, parity and other socio-demographic characteristics of the study population. The prevalence of anaemia in this population was 71.7% using the World Health Organisation cut-off point for anaemia i.e. haemoglobin level of less than 11 grams per decilitre (17). However, when the threshold for anaemia was lowered to that defined as severe anaemia in pregnancy (Hb < 7.0 grams/decilitre), only 2.6% of the pregnant women were severely anaemic. There was no association observed between the prevalence of anaemia with age, gravidity, parity and marital status. Pregnant women who reported not using bednets were significantly less likely to be anaemic than others (OR = 0.67, 95% CI 0.48, 0.96) while those who reported not using mosquito coils were significantly more likely to be anaemic than others (OR = 1.47, 95% CI 1.04, 2.08). Although not statistically significant, women with anaemia were more likely to give birth to low birth weight babies than those who were not anaemic (82.1% versus 72.7%). Discussion The results of the present study suggest that the prevalence of placental malaria infection observed in this population was lower than those reported from elsewhere in Africa (18). The prevalence of placental malaria parasitisation reported in the Gambia, Burkina Faso and Kenya were 18.5%, 19.0% and 27% (18-20) respectively as compared to 2.8% in Kigoma, western Tanzania. The difference might be due to the fact that the women in the present study were also receiving supervised malaria chemoprophylaxis from the project staff. Furthermore, comparison between our findings indicate that the prevalence of placental malaria infection was less than half (2.8% versus 19.0%) compared to the prevalence reported from Burkina Faso among pregnant women receiving chemoprophylaxis in a randomised clinical trial (19). Nonetheless the results from the present study appear to indicate that placental malaria parasitisation was associated with low birth weight which was in keeping with findings from other studies conducted in malaria endemic areas (3, 18,20,21). The implication of our findings is that malaria chemoprophylaxis strategies provided by our project seemed to help in ameliorating the occurrence of placental malaria infection in this population. The prevalence of asymptomatic malaria parasitaemia observed in our study population was again lower than those reported from other studies. For example the prevalence of asymptomatic malaria reported recently from Nigeria was 74% and 80% during dry and rainy season respectively (22) while in the present study the prevalence of asymptomatic malaria parasitaemia was 8.4% which was nearly 10-fold lower than those observed in Nigeria. These findings are from the women who were examined for malaria parasites at the beginning of the study, suggesting that the prevalence of malaria was probably low in this population even before they started malaria chemoprophylaxis regimens. The women who reported to be regular users of bednets were less likely to have malaria parasitaemia than those who reported not using bednets. This observation was expected as use of bednets is clearly a good preventive strategy against malaria. The data suggest also that women who reported using bednets were more likely to be anaemic as compared with those who reported not using mosquito bednets. This observation was somewhat surprising as use of mosquito bednets may confer protection against malaria parasitaemia which is a common cause of anaemia in pregnancy (1,23). We feel that anaemia observed in our study population may have been due to many factors including intestinal helminths as well as nutritional problems. On the other hand, the association of anaemia with low birth weight was not statistically significant but it appears that women who were anaemic were more likely to deliver low birth weight babies than non-anaemic women which was in keeping with observations reported elsewhere (9, 23). Clearly the underlying cause of low birth weight is malaria which causes anaemia in the pregnant women and in the process damaging the placenta which leads to intrauterine foetal growth retardation (11, 22). Therefore intervention strategies aimed at prevention of malaria in pregnancy may improve the health of pregnant women and also pregnancy outcome in Tanzania. Acknowledgement: We wish to thank Mrs Rachel Masisila and Mrs Anna Fute for their tireless data collection. We are also grateful to Mr. Rukinisha Kondo for handling laboratory work and the late Mr. J. Mtui for computer data entry as well as the District Medical Officer for allowing us to carry out the study in Kigoma. Our thanks are also due to the women who agreed to participate in the study. The project was financed by the Commonwealth Regional Health Community Secretariat for East, Central and Southern Africa, Arusha, Tanzania. References
© Copyright 2006 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp06010t3.jpg] [lp06010t2.jpg] [lp06010t1.jpg] [lp06010t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}