 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 3, No. 2, October 2006, pp. 23-25 MATERNAL MORTALITY AT MUHIMBILI NATIONAL HOSPITAL, TANZANIA, 1999 – 2005: LEVELS, CAUSES AND CHARACTERISTICS Method R. Kazaura1, HL Kidanto2 and Siriel N. Massawe3 Corresponding author: Method R.Kazaura, Department of Epidemiology/ Biostatistics, P. O. Box 65015, Dar es Salaam, Tanzania. Email: mrkazaura@muchs.ac.tz 1Dept of
Epidemiology/Biostatistics, School of Public Health and Social Sciences, Muhimbili
University College of Health Sciences, Dar es Salaam, Tanzania Code Number: lp06012 Abstract Objectives:To determine the
levels, direct causes and characteristics of maternal mortality at Muhimbili
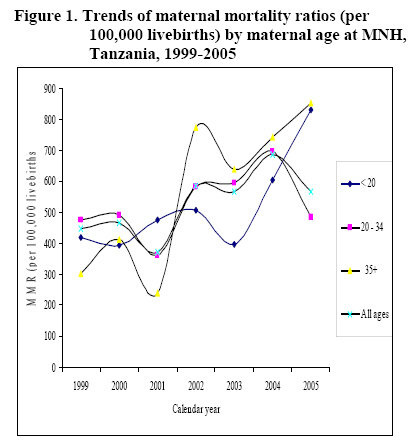
National Hospital in Tanzania. Key words: Direct obstetric causes; Maternal mortality ratio; Tanzania Introduction The International Classification of Diseases (ICD-10) defines a maternal death as death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and the site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accident or incidental causes (1). The global burden of maternal mortality is concentrated in developing countries whereby in the late 1980s it was estimated that 99% of the world maternal deaths are in these countries (2). This figure raised concern that lead to a conference on Safe Motherhood to find ways to reduce this tragedy (3). Furthermore, to recent times, one of the Millennium Development Goals (MDGs) adopted by the United Nations in 2000 aims at reducing the maternal mortality rate by three-quarters between 1990 and 2015 (4). Despite these targets and efforts, the magnitude of maternal mortality estimates in many developing countries is still high and there are no signs of tapering. For example, in 1996 maternal mortality ratio in East Africa was estimated to be 1060 per 100,000 live births (5). Recent maternal mortality ratio estimates for Tanzania range between 529 and 578 per 100,000 live births (6, 7). Between 1993 and 1999, maternal mortality ratio estimate for Dar es Salaam (the commercial and largest city in the country) was 591 per 100,000 live births (8). There are few reproductive age mortality surveys that are considered to produce better estimates for maternal mortality (5). Nevertheless, indirect approaches like the sisterhood method have been used in sub-Saharan countries to estimate maternal mortality rate (9-13). Due to lack of vital registration in these countries, also hospital-based data have been extensively used (14, 15). There are possibilities of underestimation of maternal mortality estimates because poor mothers and those living in remote areas cannot access hospital services, thus, their outcomes not considered. Also, the maternal mortality ratio may be overestimated because high risk pregnancies would tend to go to hospitals than otherwise Various risk factors associated with maternal deaths have been suggested elsewhere (15, 16). They include social and demographic factors such as maternal age at delivery, education, area of residence and some economic factors. Furthermore, maternal mortality has been associated with obstetric risk factors such as parity, number of previous abortions, stillbirths or perinatal deaths (17). On the other hand, cited major direct causes of maternal morality are obstructed labour, sepsis, haemorrhage, eclampsia, uterine rapture and pregnancy-induced hypertension (14, 15, 17-21). In this study, we use the complete and available routine-hospital-based data systematically recorded since January 1999 to December 2005 at The Muhimbili National Hospital (MNH) in Tanzania to estimate the maternal mortality ratio, direct causes and characteristics of maternal mortality during this period. Materials and methods The Muhimbili National Hospital (MNH) is one of the four big consultant hospitals in the United Republic of Tanzania situated in Dar es Salaam which is the country’s largest city. According to the 2002 National Population Census, the city had a total population of about 2.5 million (45.9% females) with annual growth rate of 4.3% (22). The Maternity Unit is affiliated in the Department of Obstetrics and Gynaecology in the MNH structure. The Unit receives referred mothers from nearby regional, district and other several vicinity hospitals in the city. The MNH serves a teaching hospital with a range of qualified personnel, for example in the maternity and delivery, operative services and in handling complicated cases is all available in the Unit. On average, about 40 mothers deliver at this Unit each day. There are early discharges for women who appear well post-natally and especially with babies of normal weight (at least 2500grms). Such women are normally observed for six hours and then discharged. We calculated maternal mortality ratio as the number of maternal deaths per 100,000 live births. Direct causes of maternal deaths defined as all complications of the pregnant state (pregnancy, labour and the puerperium), from interventions, omissions or incorrect treatment, or from a chain of events resulting from any of the above (1). Such causes are normally recorded in the registry by the medical doctor-in-charge of the ward. Although data were entered into the computer using Epi Info, statistical analyses were performed using SPSS for Windows version 11.0. Results The Unit at Muhimbili National Hospital recorded 460 maternal deaths between 1999 and 2005 out of 89,851 livebirths resulting to a maternal mortality ratio of 512 per 100,000 live births (95%CI, 465/100,000 – 559/100,000 livebirths). In figure 1, we present maternal mortality ratios by maternal age groups; categorized into high risk age groups (less than 20 and above 34 years) and low risk (20-34) years, for 1999 through 2005. There are high fluctuations of maternal mortality ratios among high risk maternal age groups over time. Nevertheless, on average maternal mortality ratios have been steadily increasing over time for all age groups, from about 447 to over 560 maternal deaths per 100,000 livebirths between 1990 and 2005. Registered direct causes of maternal mortality account for about 90% of all causes. The three leading registered direct causes of maternal deaths were eclampsia, postpartum hemorrhage and anaemia; claiming 108 (23.5%), 107 (23.3%) and 52 (11.3%) respectively for all registered maternal deaths. Other causes of maternal deaths are shown in table 1. Selected characteristics of maternal deaths are presented in table 2. Although there are variations of maternal mortality ratios between different maternal characteristics, different levels between characteristic do not differ significantly. Significant different maternal mortality ratios were by number of antenatal visits suggesting reduced maternal mortality ratios by increased number of antenatal visits. In addition, women delivering by caesarean section and by means of abstracted delivery have significantly higher chances of ending to maternal deaths than the spontaneous vaginal deliveries. Table 1. Proportionate causes of maternal deaths at MNH, Tanzania, 1999-2005
Table 2. Number and ratios of maternal mortality at MNH by selected characteristics, 1999 – 2005
*
Different sums of maternal deaths due to unrecorded characteristics Discussion Analyses of maternal health data to assess levels, trends and possible causes are some of the best gauges of the quality of health care in a particular health facility, it is also important in shaping heath status specifically to women and may be beneficial in monitoring and evaluation of programs. This study shows that, with the exception of advanced maternal age category (35 years and above) that has high fluctuation of maternal mortality ratios during the past four years, trends of maternal mortality ratios by maternal age have not significantly changed over time. This indicates that efforts to reduce the maternal mortality rate have not been very successful. Furthermore, results do not indicate a definitive liner trend of maternal mortality ratios by time period. The high mortality ratio see in this study does not significantly differ from previous national estimates of 529 per 100,000 livebirths in 1996 and 578 per 100,000 livebirths of 2004 (7, 8). However, there is still a room for underestimate because of a substantial number of mothers dying in other health facilities or at home after discharge but within puerperium period thus, not captured by the registry. The fact that more than 50% of pregnant women in Tanzania deliver at home and mostly by unskilled attendant further indicates that hospital data can greatly underestimate the mortality ratio. Despite this fact high mortality ratio recorded in this study gives a clue to the magnitude of the problem in the study area. Although one of the studies documents postpartum hemorrhage to be leading cause of maternal mortality in sub-Saharan Africa (23), we found eclampsia to be a leading direct cause of maternal mortality in the study area. Nevertheless, the direct obstetric causes of maternal mortality in our study have also been cited to be the most common direct obstetric causes of maternal mortality elsewhere (24). While a review of data of population-based studies suggest a decline in maternal mortality levels for some countries (25), hospital-based data used in this study do not show this. There is a need to make concerted efforts to improve quality of emergency obstetric care, management of pre eclampsia and eclampsia, and prevention of postpartum haemorrhage through management of the third stage. Although the use of tradition birth attendants has not been shown to change the mortality trends in various studies training them to prevent PPH by use of rectal misoprostol was shown to be very successful (9). Community midwifery can greatly reduce maternal mortality ratio by making use of retired midwives to work in the community in a country where more the 50% of deliveries are done by unskilled attendants. Improving child and maternal health are among main international goals. The level of maternal mortality may be considered one of the proxy indicators for health performance in terms of access and quality of health service delivery. Therefore, for example, community, government and non-governmental efforts that will result into a reduction of maternal mortality ratio would reflect and support the above hypothesis. Acknowledgements We are very grateful to Ms Ipyana Miller, Mr. Reid Mchome and staff at the Maternity Unit of MNH for organizing and entering data into the computer. We thank Dr D Simba for his comments and suggestions when he read the first draft of the manuscript. References
© Copyright 2006 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp06012f1.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}