 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
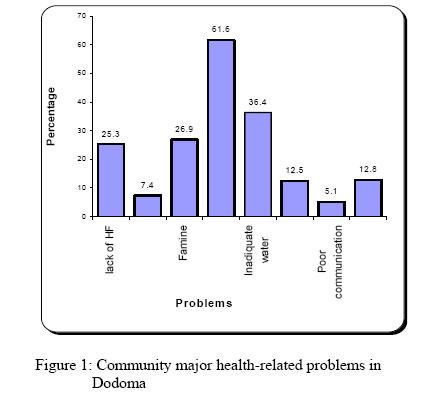
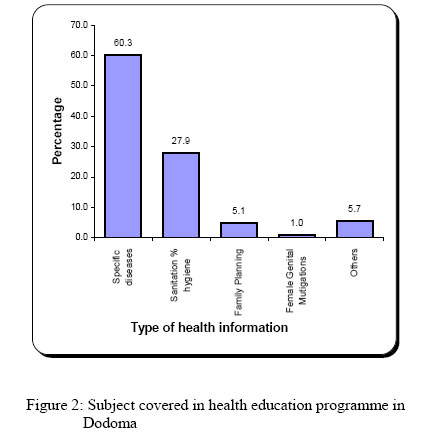
East African Journal of Public Heath, Vol. 4, No. 1, April 2007, pp. 33-39 KNOWLEDGE AND HEALTH INFORMATION COMMUNICATION IN TANZANIA Leonard E.G. Mboera1, Susan. F. Rumisha, Kesheni P. Senkoro, Benjamin K. Mayala, Elizabeth H. Shayo and WN. Kisinza 1The National Institute for Medical Resarch, Dar es Salaam, Tanzania Received 6 October 2006; revised 19 March 2007; accepted for publication 20 March 2007 Code Number: lp07007Abstract Objective: To explore and identify gaps in knowledge and information communication at all levels of health delivery system in Tanzania. Key words: health, education, messages, education, communication, gaps, Tanzania Conflict of interest There is no conflict of interest Introduction Although support for control of diseases in Tanzania has increased considerably over the past few years, an impact on the disease burdens has not yet been achieved. Serious obstacles in the control of these diseases include: poor access to health care, poor performance of health service delivery, poor availability of proper diagnosis and treatment, increased drug resistance, high costs of health services, under-utilisation of health facilities, weak disease surveillance systems as well as lack of effective health information, education and communication programmes. Health communication is a fundamental component in virtually every form of public health (1). To manage diseases in an effective and sustainable manner, the community need to have a certain set of knowledge and information on disease transmission, signs and symptoms and control and preventive measures. In most cases, the community is likely to be aware of far less than this. The difference between the knowledge that the community has and that which it should have, to make good decisions is referred to as knowledge gap (2). In any disease control programme, a good health education and information communication system is very crucial. An effective health education programme requires an appropriate communication. That is, the dissemination of understandable and useable information that concerns itself with health is critical. For individuals, effective health communication can help raise awareness of health risks and solutions, provide motivation and skill needed to reduce these risks, help them find support from other people in similar situation, and affect or reinforce attitudes. There are evidences that health communication has contributed to health promotion and disease prevention in several areas (3). Usually, in any disease control programme, health education aims at presentation of specific facts that people should know about the programme. These facts include programme objectives and the procedure and solutions. The broad programme oriented objectives are to convert public apathy into useful action, to agree on technical facts and to reconcile in understanding terms, different local beliefs and facts. Therefore, an appropriate health education strategy is expected to increase the knowledge of both the provider and the receiver, and hence change in behaviour. Such knowledge should always be able to empower the receiver to solve his/her problems in a sustainable manner. Tanzania faces serious challenges to improving the health and well-being of its people. It is the country’s aim to provide health education to the community through a number of strategies and approaches. However, available information indicate that community health education and information communication has had limited impact on behavioural changes and hence disease prevention and control (4). The healthcare delivery system is fraught with barriers to health communication at all levels, partly due to the paternalistic use of scientific and medical terminology to communicate between systems and between systems and providers, which trickles down to communication between providers and patients or communities (5). This study, therefore, aimed to explore and identify gaps in knowledge and information communication at all levels of health delivery system in Tanzania. Methodology Study area This study was carried out in Dodoma Rural District (latitudes 60, 30’ to 800’S, longitudes 350, 30’ to 3700’E), located in the central plateaus of Tanzania. The district lies at an elevation of about 800-1200m above sea level. It consists of a number of mountain chains, between which are low-lying flat areas. The areas is characterised by a dry Savannah type of climate with a long dry season lasting between April and November. The average annual rainfall is 500-800mm, which is normally a short single wet season. The main occupation of the population is crop and livestock farming. Dodoma district experiences frequent drought associated with severe famine in some years (6) In-depth interviews Six villages were selected for household in-depth interviews. A random selection of villages was done to include three strata with 2 villages each within 50km, 100 and >100km from the district capital. In each stratum, two villages, one village with, and another village without a health facility were selected. On average the average distance between the villages was 15km. The interview was carried out at household level where an adult member of the family was interviewed. An attempt was made to have a female interviewee after every other household. Interviews of healthcare workers were conducted in the three villages with health care facilities using semi-structured questionnaires. This aimed at getting information on their relationship with the communities as regards to health education and promotion and health information communication. At the district level, key informants interviews including members of the district Council Health Management Team (CHMT) were conducted. The exercise aimed at getting information on the wider issues of policy and regulatory environment in which providers work, identify different roles played by different health stakeholders regarding types of health information, approaches used to disseminate it, to different levels and factors that hinder the appropriate use of health information among the community members. Group discussions Twelve Focus Group Discussions were conducted, two in each village, involving men and women separately in groups of 8-12 individuals each. The aim of the discussions was to capture information on the knowledge of different health problems and the health education that is provided to the community. The information sharing between community and health care facility staff as well as factors influencing appropriate use of health information were explored during the discussion. In each village, discussions were also held with primary schoolchildren. Six groups (each with 12 children) were selected, one from each school involving both girls and boys of standards five to seven. The aim of the discussions was to explore the knowledge about the major health problems in their communities and their experiences in health education communication. The children were also asked to rank prevalent diseases in their communities on the basis of their importance. In each village, similar discussions were held with traditional healers. Documentary review at facility and district levels An inventory was made of the type of health information, education and communication (IEC) materials available at health care facilities and district office, as well as in public places. Documentation was made as of the subject matter, type and clarity of the health messages contained in the IEC materials. Ethical consideration All questionnaires were administered with individual’s verbal informed consent. All individual and household data were confidential. At community, facility and district levels, the information were based on summary data that cannot be linked to individuals or individual households. The Medical Research Coordinating Committee of the National Institute for Medical Research approved the research protocol. The information collected was fed back to the district and health facility level workers. Data analysis The questions were coded before data entry. All data (quantitative and qualitative) were entered into a computer using Epi-Info version 6. Statistical analysis was performed using STATA statistical analysis software package version 7 (7). Results Community A total of 297 individuals participated in the in-depth interview at community level. Most (53.5%) of them were females and the majority were of the age group 25-44 years old. Over 78% were married, and Christians formed the largest proportion (94.3%) of the respondents. Over 50% of the respondents were heads of household. Most (78.5%) of the respondents had primary school education. Subsistence farming was the main income (94.6%) generating activity of the communities in the district. Diseases were mentioned by the largest (61.6%) proportion respondents as the most important community health problem. Others included lack of safe water (36.5%) and frequent famine (26.9%) (Figure 1). Communicable diseases such as malaria, Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome (HIV/AIDS) and cholera were the leading cause of morbidity and mortality (Figure 2). Most community members were knowledgeable of the symptoms and control measures for malaria, cholera, eye infections, HIV/AIDS, diarrhoea and tick-borne relapsing fever (TBRF). Similar findings were obtained from focus group discussions. A health facility was considered by the majority (91.6%) of the respondents as the most important and reliable source of health information (Table 1). Religious leaders and radio were ranked second (mean=72.1%) and third (mean=70.7%) as the best sources, respectively. Newspapers were considered as important source of information in one village only (50%). In all six villages, research or development projects (19.5%) and traditional healers (14.8%) were the poorest source of health information. In terms of easy of access of health information, health facilities (77.4%), religious leaders (65.7%) and village health workers (53.9%) were ranked high by most of the respondents. Table 1: Source of health information according to the number (%) of respondents
Public meetings, church congregations, seminars and social gatherings were the most preferred venues for health education communication. This was said to be a place where people would meet health experts and usually given an opportunity to air their views on health matters. However, most respondents said that meetings where health was the main agenda were rare. One had this to say, “health education is just provided when the District Commissioner pays us a visit. Otherwise, most meetings are for political agenda or community sensitisation on tax collection.” Obstacles in accessing health information by the community included long distances to health facility, illiteracy among community members, lack of adequate health educators and gender barriers. Women had better opportunities to attend health education sessions (at the Maternal and Child Health clinics) than men. It was pointed out that only a few men would always attend any health education session through public meetings. House visits were described to be not effective in health education communication, as they were not synchronized with the time most people were at home. Moreover, community health education was reported to be provided irregularly. On average, 66.3% (range= 43.5-78.9%) of the people found health education easy to understand. However, 28.3% of the respondents admitted to face some difficulties in adopting and utilizing health messages due to poverty, ignorance and the inappropriateness of some of the health education messages. Others reasons included lack of safe water, beliefs and traditions. Similarly, group discussants considered local beliefs, difficult language, inappropriate venues, gender barriers and ignorance as the major constraining factors in utilising health messages. There were no specific persons responsible for providing health education communication at community level. Village health workers and health officers were available in some villages but were reported to carry out health inspection rather than health education. One had this to say “there is no health officer assigned to conduct health education sessions except during a special event such as the visit of our District Commissioner.” Subjects most frequently covered in community health education packages included hygiene and environmental sanitation (e.g. construction and use of latrines) and communicable disease prevention and control (HIV/AIDS, malaria and cholera). Disease prevention and control formed the largest proportion of the contents of health education packages (Figure 2). Findings from focus group discussions also showed that sanitation and hygiene, nutrition, immunisation, family planning and disease control were the most common subjects covered in health education programmes. Traditional healers Nine traditional healers (40-79 years old) were interviewed. Among these five were females and four were males. According to traditional healers, major problems in their communities were diseases, shortage of safe water supply, frequent famine, witchcraft and cattle rustling. Disease conditions attended by the traditional healers included gynaecological problems, seizures, headache, abdominal pains, abscesses, back-pains, malaria, tick-borne relapsing fever, anaemia, eye diseases, HIV/AIDS, cholera, tuberculosis, meningitis, schistosomiasis and diarrhoea. Traditional healers were obtaining health information from health facilities, radio, village health committee, relatives and religious leaders. All of them admitted to rarely provide health education to their clients. Schoolchildren According to schoolchildren, the major health and health-related problems were lack of safe water, famine, poor communication infrastructure and lack of health facilities. Malaria, cholera, trachoma, sexually transmitted infections and HIV/AIDS were the major specific disease problems in the district (Table 2). The source of health information included teachers, public meetings, health facilities, radio, television, drama and newsprints, as well as IEC materials displayed in various public areas including, health facilities and village offices. Health officials were said to rarely visit schools to provide health education to the children. Subjects on diarrhoea, HIV/AIDS, measles, sexually transmitted infections, neonatal tetanus, polio, cholera and malnutrition were taught at school. Posters were the only IEC materials available at the six schools visited. The health-care messages covered in the posters included family planning, sanitation and hygiene, sexually transmitted diseases, HIV/AIDS, malaria and trachoma. None of the schoolchildren groups was aware of any school health programme run by the Ministry of Health through the district CHMT. However, schoolchildren were participating in school run health programmes involving environmental sanitation, personal hygiene, safe water and prevention of communicable diseases. Schoolchildren considered themselves as an important group that could be used to disseminate health information to their family members. Most schoolchildren reported to have frequently discussed health issues with their family members. At schools, pupils were given opportunity to discuss health matters. Health education was reported by all groups of schoolchildren to be an effective means of changing behaviour. For example, the health education messages given at school have helped in promoting use of pit latrines, use of safe water and environmental cleanliness. Health Facility Workers Three health facilities were involved in the study. These were Mvumi Hospital, Mundemu Health Centre and Huzi Dispensary. A total of 14 health workers were interviewed, and they included a Laboratory technician, Nurse Midwives (3), Maternal and Child Health Aides (2) Hospital Matron (1), Public Health Nurse (1), Laboratory Assistant (1), Nurse Auxillary (2), Assistant Clinical Officer (1) and Clinical Officers (2). The major problems as identified by health workers included ignorance, poverty and poor utilisation of health services among women. It was observed that most of the time only serious cases were sent to the hospital (usually after consulting traditional healers). Delay in seeking health care was also associated with poor communication infrastructure. According to health workers, lack of safe water, drought and famine were among the major public health-related problems in the community. Health workers were providing health education to patients in the process of attending them, mainly through outpatient and ante-natal clinics. The major diseases attended at the three health facilities included malaria, acute respiratory infections (including pneumonia), diarroeal diseases, sexually transmitted infections, anaemia, meningitis, reproductive health problems (e.g. maternal eclampsia, post delivery infections, abortions), TBRF, eye infections (including trachoma), malnutrition, skin diseases, intestinal worms and urinary tract infection. Health information provided at health facilities targeted cholera, rabies, meningitis, STIs, HIV/AIDS and malaria. Others subjects included reproductive health, family planning, immunization, safe water, nutrition, female genital mutilation (FGM), personal hygiene and environmental sanitation. Health education and promotion materials were available at health facility and were obtained from the district health office and Community-based and non-governmental organizations. Most of the IEC materials at the three health facilities were posters. Six posters covering subjects on malaria, diarrhoea, family planning, safe motherhood, and nutrition, were displayed at the hospital. At the health centre, four posters were available, however, only two were displayed. The posters carried messages on HIV/AIDS, family planning, tuberculosis, and STIs. One of the posters had messages in English. Ten posters were found at the dispensary, with messages on malaria, family planning, nutrition/malnutrition, intestinal worms, measles, polio, STIs and vitamin A supplementation. All posters (except that on nutrition) were displayed and accessible to dispensary clients. Banners on HIV/AIDS and trachoma were also found at the dispensary. A large number of brochures, leaflets, and magazines covering subjects on malaria, polio, measles and family planning were found at the health centre. However, they were not made available to the clients. Health workers were providing community health education through public meetings/ seminars, during clinics, through IEC materials, house to house visits and through village leaders. The health staffs felt that the communities were often utilising health messages provided exemplified by an increase in coverage in the use of mosquito nets, use of latrines, immunisation and family planning. Health education and information was also provided by health staff at outpatient units and Maternal and Child Health clinics and at treatment camps during outbreaks. Video shows, posters, pamphlets, brochures, leaflets (distributed during community meetings) and radio were commonly used to disseminate health information. Mobile clinics, public meetings, use of drama groups, school teachers, village health workers, traditional birth attendants and Community-based development groups were also involved in providing health education and information to the communities. According to health facility workers, major factors that facilitated easy information communication included good cooperation with various stakeholders, language and commitment of health workers. However, lack of funds, inadequate qualified health educators, lack of financial and material resources for outreach services, lack of refresher trainings and poor supportive supervision from the district were the main constraints in health information communication. Health workers identified alcoholism, famine, local beliefs, non-compliance and ignorance as major hindrance factors in the utilisation of health information by the community. Monitoring and evaluation of health education programmes was not done in all the three health facilities. According to CHMT, malaria, acute respiratory infections (including pneumonia), diarrhoea, eye infections, STIs (including HIV/AIDS), skin infections, intestinal worms, TBRF and malnutrition were the most important health problems in the district. Subjects covered under the district health education programmes were categorised into disease prevention and control (including immunisation); reproductive and child health; environmental sanitation and hygiene; and nutrition and malnutrition. According to the CHMT, health education was provided to the community through formal or informal face-to-face meetings with community leaders; seminars/workshops and EIC materials (including video shows). More IEC materials were found at the district office than in any of the three health facilities, and most of them were posters on communicable diseases, environmental sanitation and hygiene. Unlike in the health facilities videocassettes were also available at the district office. Most health education materials found at the district office were obtained from the Ministry of Health in Dar es Salaam or the Regional Medical Office in Dodoma. Some health education materials were obtained from other sectors including Water, Agriculture, Livestock Development, Community Development and Non-Governmental Organizations. Members of the CHMT admitted that some of the health information was neither clear nor relevant to the community. Some would require further interpretation, which was difficult; and sometimes would be misinterpreted by the community. Despite the fact that all members of the CHMT were involved in providing health education, only one of them had received formal training on health education and communication. It was observed that some disease control programmes at the district level had health education component in their strategic plans. These included programme on Immunisation, Reproductive and Child Health, Tuberculosis and Leprosy, and Malaria. There were no specific mechanisms for monitoring the acceptability and utilisation of education/information among the community. An increase in immunisation coverage, use of insecticide treated nets, improved sanitation (e.g. use of latrines), high demand for family planning, were usually employed as indicators of success in health education programme. Ignorance among community members; inadequate resources, poor feedback and lack of supervision from higher levels and poor communication infrastructure were identified by the district team as the major constraining factors in health education provision. Gender was also identified as a barrier in providing information. In some instances (e.g. when providing education on the use of condoms) it was required to separate males from women. Poor attendance of women during meetings was another constraint. Women would need to ask for permission to be allowed by their husbands to attend such sessions. Discussion Health facilities are among the most reliable sources of health education in Tanzania. However, health services are often not accessed by many people particularly in rural areas because of health care charges, long distances, inadequate and unaffordable transport systems, poor quality of care, equity, and poor governance. In areas where the services are poor, few communities will seek care from such facilities, as observed in one of the villages in our study. Equitable and universal access to health-care information is recognised as an important aspect in health provision as reported recently (8). Religious leaders, schoolteachers and influential persons were identified as among the most reliable providers of health information. However, health education has to do with health, correct knowledge about various aspects of health and disease is highly essential for communicating ideas for the purpose of producing necessary attitude and behaviour. It is therefore important that people who have been trained for providing health care are much better fitted to give health education in the community than lay persons. This, however, does not rule out the role of non-medical and non-health personnel as health education providers but it only emphasizes the importance of acquisition of correct and complete information and knowledge on relevant health problems and their application (9) and the need to involve various stakeholders to enhance health education programmes as identified in this study. Partnership between such lay persons and health professionals is critical in promoting effective health education communication. Media through which health communication was effected in the district were of mainly four categories: local media, mass media, print materials and interpersonal contact. Our findings have shown that the most commonly used channels belonged to the first three categories. Public meetings, radio and print materials, mainly posters were the mostly used channels of communication. The correct choice of information channels depends on relative impact and cost and hence cost effectiveness. Impact is a function of the proportion of the target audience reached by the channel, the frequency with which the audience can be exposed to messages, the channel’s credibility, and the quality of the production (10). Although local media including public meetings and religious congregations were preferred by the majority of the respondents, their potential is restricted by the possibly limited exposure of audiences to them and the fact that they are non-medical sources. They can, however, be used to convey only simple, easily understood messages. Mass media such as radio and newspapers are popular but not accessible by many, especially in remote rural areas. A survey carried out in Tanzania indicates fairly high radio ownership in urban (62.5%) than in rural (29.8%) areas. On the other hand, television ownership in Tanzania stands at 3.4% and 0.1%, in urban and rural areas, respectively. It is true that radio/televisions programmes are more effective in communication of new information. The major advantages of mass media are the consistency of the message and the potentially high frequency of exposure. However, they do not reach all target audiences because of the community affordability and proprietors conflicting interest in the use of broadcast time schedules (11). Like in our study, other researchers have also found that the main reasons for not listening to radio or television, is the ability to afford them (12). Print is a less expensive channel, but its reach is limited by illiteracy, poverty and isolation. In our study, only one of the six villages, the community had daily access to newspapers. Posters must be displayed where people would see them often. Interestingly, most of the posters in our study were found placed at the district office and health facilities, where a small proportion of the population visit health facilities, either as patients or with sick relatives. Rarely, people visit district health offices, hence are unlikely to have access to the IEC materials that are available and or displayed. Leaflets are useful for complicated messages, such as mixing instructions on how to treat bednets with insecticides, because they can be given away for people to keep for reference. Of the major constraints to extensive use of print materials in Tanzania is the high illiteracy rate, especially among women. The visual components of print materials are particularly important and must also be assessed for comprehension and carefully tested (13). Posters and other visual IEC materials which are developed without the community input and which are never pre-tested may misinform the community instead of educating them. Interpersonal contact including face-to-face and house-to-house visit, is the channel with greatest impact. However, it is also the most difficult to manage on a large scale because of the relatively low number of people any health educator can reach implies either a large number of trained individuals or a long timeframe. From the health provider perspective, seminars, workshops, visual IEC materials were the most utilised venues in the health communication strategies, because of lack of critical resource. Poorly structured home visits by the same health workers who are too overworked and demotivated are the common phenomena in Tanzania. Such visits need to be properly planned and integrated into routine programmes and synchronized with the community activities (4). Several factors have been identified as bottlenecks in the implementation of health education communication programmes in the country. These include inadequate funds, poor infrastructures, language barriers, inadequate health education communication materials, inappropriate health education messages, local beliefs, poverty and ignorance. Lack of health providers trained specifically in health education was common at the facility and district levels. The shortage of skilled manpower, while a serious concern to all actors in the health sector including government, continues to persist and is affecting the delivery of social services in the country. Our findings have shown from both the community and provider perspective, socio-economic and cultural factors hinder the utilisation of health education messages and hence behavioural changes. It has been identified that not all information are understood and utilised by the community. Ignorance and poverty have been described by many communities as the most challenging factors in getting and utilising proper health education messages. Many poor households have fallen deeper into poverty as they end up using their limited and critical assets to pay for treatment and care of patients. Some of the health problems interventions require financial inputs. Thus interventions that require financial inputs by the households are likely to drive poor people deeper into poverty and increase their vulnerability significantly. In such situation, prompt behavioural changes may not be realised in the pace expected by health providers. Lack of community participation and decision making in the type of health education to be provided was expressed by respondents from all villages. Community participation is very limited as regards to determining health care priorities and the knowledge they need (14). More importantly though, reliable mechanisms are not in place for discussing issues of concern at the community or village level and then raising these concerns to the district and national levels for action. In order to improve the effectiveness of the implementation of health education communication strategies, monitoring and evaluation of the performance of the programmes is important to ensure that the programme is accomplishing its goals. Monitoring and evaluation was lacking in health education communication programmes at district and facility levels. Monitoring and evaluation of the health education communication programmes may be done in a participatory way, based on which the programme may be re-designed periodically. A monitoring and evaluation, done in a participatory mechanism may help to detect flaws and oversights must be built into all health education communication programmes. Conclusion This research has identified gaps in health knowledge and information communication in Tanzania. These gaps are related to type of information communicated to the community, capacity of the health care providers in communicating health information, poverty, ignorance, gender, and inability to put into practices the health education messages. This implies that the health system service needs to be improved or that the form in which information is relayed to the community needs to be changed. Although the information gets to the community, people are not able to utilize it properly because they lack the necessary background knowledge and resources. In this case more effort devoted to community sensitisation and education is implicated. AcknowledgementsWe would like to thank Samuel Likindikoki, Loi Mwaipiana, Wende Luvinga, Prince Mutalemwa, William Kisoka, Michael Munga, Oforo Kimambo, Flaviana Paul, Editha Didas and Emmanuel Mmbega for their excellent technical and field assistance. This study received financial assistance from the International Development Research Centre of Canada. References
© Copyright 2007 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp07007f2.jpg] [lp07007f1.jpg] |
| |||||||||

{kind=link}
{kind=link}