 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
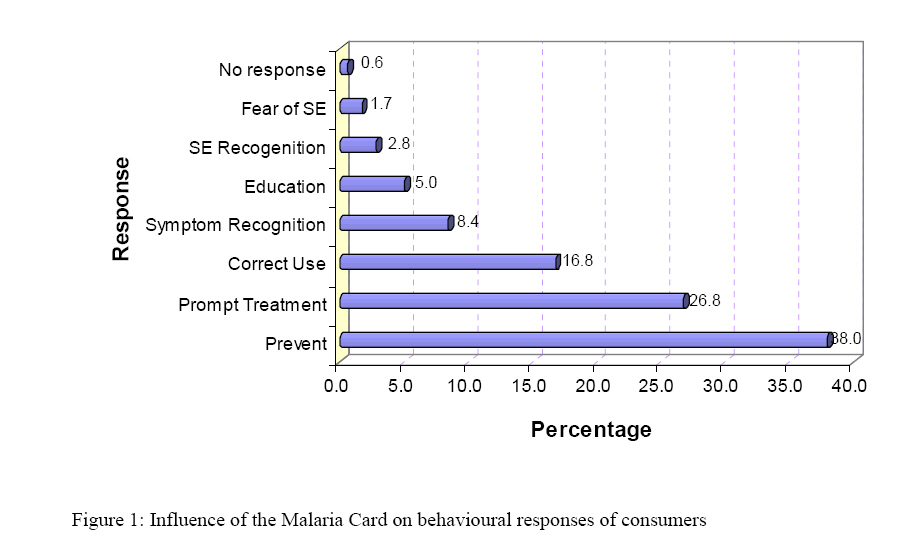
East African Journal of Public Heath, Vol. 4, No. 2, October 2007, pp. 59-63 CONSUMER SURVEY OF MALARIA FACT CARD:AN EDUCATIONAL AND COMMUNICATION TOOL IN TANZANIA M. Chambuso, V. Mugoyela , W. Kalala1 Correspondence to: Dr. M. Chambuso, School of Pharmacy, Muhimbili University of & Allied Health Sciences, P.O Box 65013, Dar Es Salaam, Tanzania. E-Mail: mchambuso@muchs.ac.tz Received 15 December 2006; revised 25 March 2007; accepted for publication 10 April 2007 Code Number: lp07013 Abstract Objective: To determine the usefulness of the malaria fact card as a health educational and communication tool in Dare s Salaam. Key words: Consumer survey, Malaria Fact Card, community pharmacy, pharmacist. Introduction: The Malaria Fact Card is a printed health educational and communication tool and could be widely promoted by pharmacists in their community pharmacies. The Fact Card is designed to work at public health level to educate consumers and at community pharmacy level for profiling pharmacists as health educators. At the community pharmacy, the Fact Card serves as a useful communication tool linking patients, pharmacists and products (1). Other types of Fact cards such as flow charts and diagnostic cards have been applied in some countries elsewhere. Studies in Benin and Kenya showed that involvement of health workers in the development of flow charts increased their use, and in Indonesia diagnostic cards distributed among primary health care workers showed a significant improvement in diagnosis performance (2-4). As it appears, Fact Cards are valuable educational tools acting as a source of reliable health information for staff training. Drug treatment and prevention strategies for malaria may need to change from time to time within a country due to emergence of drug resistance. The Commonwealth Pharmaceutical Association (CPA), Pharmaceutical International Federation (FIP) and the World Health Organization (WHO) Malaria Task Group recognized the underlying benefit of using Malaria Fact Cards in the fight against malaria. Community pharmacies and other retail drug stores in the community are placed in strategic areas and therefore provide the best opportunities for distributing these cards thus improving malaria treatment and prevention (3). In Africa the Malaria Fact Cards have already been introduced in Zimbabwe and Ghana for distribution through community pharmacies (1). In Tanzania, the Pharmaceutical Society (PST) in collaboration with the CPA introduced Malaria Fact Cards in community pharmacies in Dar es Salaam during 2003. The objective of introducing Malaria Fact Cards in Tanzania was to disseminate information to the community on malaria transmission, symptoms, treatment and prevention to enhance consumer awareness of the new first line antimalarial introduced at that time (5-6). The change brought in a Sulfadoxine-Pyrimethamine (SP) combination to replace chloroquine against which the malaria causing organism (Plasmodium species) had developed widespread resistance necessitating a change in the national malaria treatment policy. This paper reports on the impact of the intervention that was carried out among consumers of the Malaria Fact Cards in Dar es Salaam one year after their introduction in pharmacies. Materials and Methods Study design The study was exploratory to find out whether the Malaria Fact Card had enhanced the dissemination of information on malaria and increased awareness on the changes made in the treatment guidelines from chloroquine to a combination of SP in Dar es Salaam. Study areaThe study was carried out in community pharmacies that were involved in the distribution of the Malaria Fact Cards since 2003. The pharmacies were located in the three municipalities of Dar es Salaam city namely, Ilala, Kinondoni and Temeke. Dar es Salaam was chosen because it is a capital city and has got a large number of community pharmacies served by full time pharmacists. It was anticipated that once the cards establish themselves in the capital city they could be easily rolled out to other regions. Study populationThe study population consisted of 74 male and 57 female adult patients who visited the pharmacy to purchase antimalarial medicines. The research assistants were final year undergraduate students of the School of Pharmacy at the Muhimbili University of Health and Allied Sciences. Only adult patients above 18 years of age were included in the study due to their ability to understand and respond well to the questions posed by the interviewers. Methods of data collection Data were collected between January and February 2004 through semi-structured questionnaires. The questionnaires consisted of open and close-ended questions written in English. The interview was conducted in Swahili but the responses were translated into English by the interviewer before filling in the questionnaire. Prior to interviews, informed consent from each interviewee was sought. Only those who consented to participate in the study continued with the interview. The questions sought information about sex, age and residence of the respondent. Further questions were directed towards information on frequency of visits to the pharmacy and whether the pharmacist was requested for health information/advice. The set of questions regarding the card presentation and content required respondents to mention if the card were easy to read and understand and how much information on the card was new to them. Other questions sought information on increase in knowledge of malaria prevention and treatment. In these questions consumers were asked what new information they had learnt from the Card. Another set of questions was geared to study consumers' behavioral response. In this case consumers were asked how they would use the information on the card. ResultsOf the 131 consumers covered in this study, 69% were regular residents of Dar es Salaam while 29% came from outside the city and 2% came from outside the country. The majority of respondents (80%) were aged between 20-50 years. Genderwise, 57% were male and 43% female. Further, results indicated that 33% of consumers visited the pharmacy on regular basis, 52% visited occasionally and for 15% this was their first visit. Eighty-four percent of the respondents stated that they normally asked the pharmacists for health information/advice and 16% never asked. Results also indicated that 77% of respondents said they would return to the pharmacy to obtain health information/advice when needed by the family. Regarding the Fact Card presentation and content, 95% of consumers reported that the Card was easy to read and understand. On new knowledge gained from the card, 66% of respondents stated that they had learnt some new facts about prevention and treatment of malaria. The most important category of new information the respondents gained from the card was on correct treatment of malaria (64.6%, n=127) (Table 1, Figure 1). Within this category, the most important sub component was information on how to take the medication correctly (38.6%) followed by the side effects to be expected from the medication (22%). The other sub components of new information on how to treat malaria, the importance of prompt treatment and how to give a correct dose to a child received low scores (2.4%, 0.8% and 0.8% respectively). The second most important category of new information the respondents gained from the card was on general information about malaria 17.3% (n=127) (Table 1). In this case the respondents found information on the different brands of SP to be most useful (14.2%) while information on malaria as a cause of morbidity and mortality received less scores (1.6%). The category on information on recognition of symptoms was ranked third attaining a total score of 9.4%. Within this category the early malaria symptoms in the general population were considered to be more important (8.7%) than those specifically related to children (0.8%). Information on prevention of malaria was ranked fourth (8.7%), with prevention strategies being considered more useful in the category compared to method of transmission (1.6%) and prevention strategies during pregnancy (0.8%). Assessment of the impact of the Fact Card on respondents' behaviour indicated that the card was successful in reinforcing their practices in the prevention of malaria (38%) followed by seeking prompt treatment (26.8%) and using SP correctly (16.8%, Table 2). However, the card had lesser influence in enabling consumers to educate their families on the use of SP (5%), recognition of side effects of SP (2.8%) and refusing to use SP for fear of side effects (1.7%). Table 1: Responses on new information learned by respondents from the Cards (N = 127)
Table 2: Consumer behavioural response (N= 179)
Discussion The consumer survey was conducted to assess the impact of the Malaria Fact Card distributed by the Pharmaceutical Society of Tanzania through community pharmacies. The target population was low-income urban dwellers. It was felt that this particular group was 'high risk' and would benefit from information on malaria prevention so as to reduce their expenditure on treatment. The results showed that more male (57%) than females (43%) consumers visited the pharmaceutical outlets. It may thus be inferred that gender has an influence on health seeking behaviour as has been reported in other studies (7). Survey results indicated that 68% of consumers lived within the area where the community pharmacies were located and most of them were of income earning age. Results from this survey indicate that at least a third of the consumers interviewed were regular customers of a given pharmaceutical outlet. This lends support to the assumption of the Malaria Fact Card campaign that community pharmacies are very suitable locations for interventions aiming to improve patient compliance. A related intervention conducted at Keele to reduce risk behaviours and risk factors for coronary heart disease demonstrated the valuable contribution of community pharmacy-based services (8). The high percentage of patients that expressed readiness to come back to the pharmacy to receive advice when needed indicates the confidence they had in the services they received from the pharmaceutical personnel. Furthermore, the survey confirmed that the contents of fact card had been carefully formulated presenting little difficult for the majority of the consumers to read and understand acting as a source of new knowledge for two thirds of the interviewed consumers. In terms of effectiveness of the messages on the card, information on correct treatment of malaria, how to take the medication correctly and the side effects to be expected from the medication were well received. However information on how to treat malaria, the importance of prompt treatment and how to give a correct dose to a child need to be improved in the next revision of the card as these areas did not make as great an impact. The second most important category of information the respondents gained from the card was on general information about malaria 17.3% (n=127). In this case the respondents found information on the different brands of SP to be most useful (14.2%) while information on malaria as a cause of morbidity and mortality received less scores (1.6%). From the results it was observed that there are promising indicators of awareness of pharmacists as information providers as well as medication suppliers. Of all consumers interviewed 50% stated to have asked the pharmacists for health information/advice. Providing health information to and/or counseling patients on how to use their medications are one of the requirements of good pharmacy practice (8-9). In the past the majority of pharmacies in Tanzania were designed specifically for dispensing medicines only as evidenced by the small dispensing window. As it appears now, the roles of pharmacists are changing and more space is needed for patient counseling and confidentiality. Also gathered from the survey is the fact that 77% of respondents said they would return to the pharmacy to obtain health information when needed by the family. This shows awareness among consumers of the pharmacist as a source of health information. Pharmacists in the line of health care delivery are strategically placed and may play a very big role in implementing rational use of medicines (10). This study has revealed that 95% of respondents reported the malaria fact card was easy to read and understand. This would indicate that consumers had no difficulty in processing the information and understanding its intent and, therefore, information on the Card was pitched at a level well suited to the target group. Sixty percent of respondents admitted to learn some new facts and information about malaria from the Cards. These statistics would suggest a significant role played by the Cards by imparting consumers with knowledge of malaria prevention and treatment and also in 'reinforcing ' this knowledge in one third (30%) of the respondents who knew only a little bit of information about malaria prior to reading the card. The Malaria Fact card was introduced shortly after the change in the national treatment guidelines replacing chloroquine with SP medication in Tanzania. Results of the survey (Table1) show that 64.6% of consumers accepted that they learned from the cards information about malaria treatment using SP. Of the things they learned included, prompt treatment of malaria is essential, how to take medication in adults, how to give correct doses to children and awareness of the side effects. In Tanzania introduction of SP to the community as first line treatment had a negative impact due to the known side effects (11). From the cards 14.2% of respondents benefited from learning different brand names of SP. Prior to the distribution of the cards, SP was an ambiguous term standing for an antimalarial medicine. The issue of public education is very important especially during policy change of any medication (12,13). It has also been revealed that 8.6% of consumers learned new methods of transmission, prevention strategies in general and specifically during pregnancy. The rest of the information on the Cards reinforced their knowledge on prevention strategies. They already knew different strategies of preventive measures such as use of insecticide treated nets (ITN), mosquito repellants at night and fumigation. The use of bed nets reduces the degree of human-vector contact and malaria transmission and the prevalence of malaria infection can be significantly reduced through use of insecticide impregnated bed nets (14). In Tanzania and other countries where malaria is endemic chloroquine was routinely given to pregnant women until when SP was introduced a first line treatment for malaria (15,16). The survey questions that were investigating consumer's behavioral change aimed to find out how the respondents would use the information on the cards afterwards. Results showed that out of all responses given, 68% related to the prevention strategies and 27.4% related to the correct use of SP medications. The response relating to the use of malaria prevention strategies is especially encouraging as it is a positive indication that the type of information regarded by the Pharmaceutical Society of Tanzania as important to the target group could have significant impact within that group. In relation to the correct use of SP medications, it is important to note that only 1 (0.6%) response denied to take SP because of potential side effects while 48 (26.8%) concurred and admitted that the information on the Malaria Fact card had promoted their confidence in the use of SP medication. Proper labeling with information on how to take medicines during dispensing is important because it reinforces the verbal information provided by the dispenser (17). In this study, 8.4% of responses indicated that the information provided on a Card can be referred to the family members and friends and this was also an important result from the survey. A concern from this study may be that only 2.8% responses referred to 'prompt treatment'. Early commencement of medication is an integral part of the successful treatment of malaria. Erhun W.O et al in his study on malaria prevention (KAP) results indicated that convenience and severity of the disease were the major indicators in over 50% of respondents' choice of treatment and 19.9% would first resort to spiritual means as a treatment method during a malaria incident (14). In this study the low levels of response on 'prompt treatment' would suggest that respondents seek other means before they opt for treatment. Hence this is a message that may need further reinforcement, either more prominently on the Fact Card or through public awareness campaigns, or both. Conclusion and RecommendationsThe results of this study showed that respondents in Dar Es Salaam city through a Malaria fact card as tool of communication see the pharmacists as a source of relevant health information and advice. This is a sound foundation for continuing, and expanding, the Malaria Fact Card project in Tanzania as an educational and communication tool. However to maintain the consumer confidence pharmacists must continue to provide quality service and in relation to this Card, by regularly revising and up-dating it; ensuring always that the Card does not loose its 'consumer focus'. As appears in this study the community needs and wants health information hence Malaria Fact Card could be the first of many Fact Cards to be formulated in Tanzania. Acknowledgements: We appreciate the cooperation showed to us by the retail pharmacy owners during data collection. We acknowledge for the financial assistance by the Commonwealth Pharmaceutical Association extended to us through the Pharmaceutical Society of Tanzania. Finally we thank the PST for entrusting us to conduct the survey. References:
© Copyright 2007 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp07013f1.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}