 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 4, No. 2, October 2007, pp. 67-72 SAFE-DELIVERY PRACTICES IN RURAL BANGLADESH AND ITS ASSOCIATED FACTORS: EVIDENCE FROM BANGLADESH DEMOGRAPHIC AND HEALTH SURVEY-2004 Mohammad A. Kabir Correspondence to: Mohammad Alamgir Kabir, Assistant Professor, Department of Statistics, Jahangirnagar University, Savar, Dhaka, Bangladesh. E-mail:alamgirfa@gmail.com Received 10 June 2007; revised 15 August 2007; accepted for publication 20 September 2007 Code Number: lp07015 ABSTRACT Objectives: This study examined the safe-delivery practices
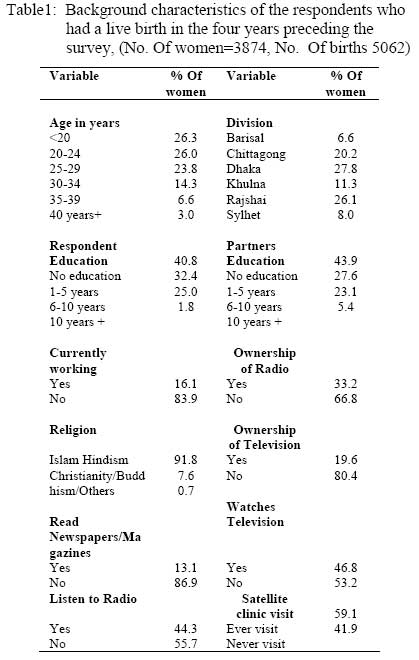
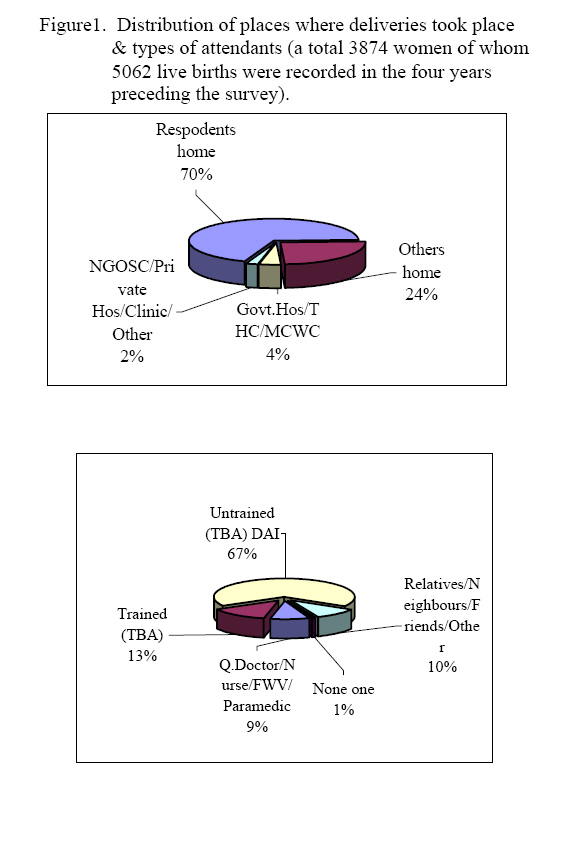
and its associated factors among rural Bangladeshi women. Keywords: Bangladesh, ever-married women, safe-delivery, medically trained persons, logistic regression Introduction Around the world, people celebrate the birth of a new baby. Societies expect women to bear children, and honour women for their role as mothers. Everyday, at least 1,600 women die worldwide from the complications of pregnancy and childbirth, 90% of which occurring in Asia and sub-Saharan Africa. Maternal mortality rate (MMR) was shown to have the largest discrepancy between developed and developing countries (1,2,3). Maternal mortality rates are very high in developing countries, and exceed 1000/100,000 live births in approximately 21 developing countries (4). A lifetime risk of maternal death in developing countries is forty times higher than that of the developed world (1,2). The International Safe Motherhood Initiative made maternal mortality an international priority by way of access to basic maternity care during pregnancy and delivery to all women (5, 6). This unacceptably high MMR directly contributes to the high prenatal (newborn) mortality rate in the country. The situation in South Asia is more precarious, which accounts for about half of the global maternal deaths (7). Despite some improvement, maternal mortality rate in Bangladesh is still very high even by the standards of the other developing countries. Delivery related complication is one of the leading causes of maternal mortality in Bangladesh. Results of a study conducted in rural Bangladesh showed that one-third of the women experienced delivery related complications during their last delivery (8). Pregnancy and childbirth related complications are among the leading causes of maternal mortality in Bangladesh. The estimated lifetime risk of dying from pregnancy and childbirth related causes in Bangladesh is about 100 times higher than in the developed countries. The tragic consequence of these deaths is that about 75% of the babies born to these women also die within the first week of their lives. A study on safe motherhood programs in Bangladesh assessed that women's low status in society, the poor quality of maternity care services, lack of trained providers, low uptake of services by women and infrastructure and interdepartmental difficulties all contribute to the high rate of maternal deaths. Women's lives can be saved and their sufferings reduced if health systems could address serious and life threatening complications of pregnancy and child birth when they occur. One of the best ways to do this is to make sure that women receive skilled care at delivery. Providing skilled care means ensuring that health professionals such as doctors, nurses or midwives can manage normal deliveries and treat the life-threatening complications of pregnancy and child birth. Therefore skilled care at delivery or 'safe delivery' has its greater significance in reducing sufferings of reproductive health system from women. Literally 'safe' means secure or free from danger or harm or injury, and 'delivery' means the actual process of expulsion of the foetus. So, etymologically safe delivery means proper control of the risks to the health and safety of persons. Delivery performed by trained health care providers with proper equipment and correct technique is the safest. So, safe delivery ensures that all deliveries are attended by persons with the right knowledge, skills and equipment and also provide post-partum care to mother and baby. It is safest to have delivery in an institution with appropriate medical facility. Delivery in a hospital also ensures newborn care and therefore can reduce incidence of infant mortality substantially. In institutions, emergency conditions like bleeding, obstructed labour requiring operation can be promptly attended. Such events may not be predicted in advance and also cannot be attended at home. In case delivery in an institution is not possible, the second best optimum is to conduct the delivery in home by a trained health person like an Auxiliary Nurse Midwife (ANM), Lady Health visitor (LHV), or a trained Dai. Improvement of Bangladeshi women's health is not just a social and moral necessity; it is also an economic imperative. In Bangladesh, most mothers do not receive any ANC, and home delivery is almost universal. Ideally, all pregnant women should have regular antenatal checkups either by a paramedic or by a doctor. Findings of several studies indicate that women have limited knowledge of life threatening complications of pregnancy and childbirth. Husbands, the decision-makers for use of obstetric care services, are even less knowledgeable than their wives (9,10). The high rate of maternal mortality in Bangladesh can partially be reduced through safe-delivery practices among rural women. Safe delivery reduces the probability of mortality of mother and her baby (11). Some studies have shown that the probability of survival of the baby declines with the death of a mother. On the other hand, when a baby dies, the mother soon gets pregnant. Such repeated pregnancy taxes the health of the mother and threatens both her life and that of the foetus (12). The government health centres, such as Thana Health Complexes (THCs) and Health and Family Welfare Centres (HFWCs) at the union level, provide maternal health care including delivery services free of charge to the rural population. However, the use rates of delivery services of these health centres are very low (13). Most deliveries take place at homes, and are assisted by untrained traditional birth attendants (UTBAs) and relatives (14). The deliveries which take place at homes and are assisted by untrained birth attendants are very often done in unsafe and unhygienic conditions, resulting in high risk of maternal and neonatal morbidity and mortality (12). The Bangladesh Maternal Health Strategy recommends at least three visits during pregnancy. The first visit is to make soon after the woman realizes she is pregnant. The second visit should be made between the fifth and seventh months of pregnancy. The third visit should be made at the ninth month of pregnancy. Additional visits should be made if any problems or danger signs arise. Delivery performed by traditional birth attendants, friends and relatives without the necessary skills and services have not reduced the risk of maternal deaths as compared with deliveries conducted by doctors, nurses and trained birth attendants. As mentioned above though there are studies on delivery and maternal morbidity but more studies are required on safe delivery attended by trained personnel and its influence on maternal or obstetric morbidity. The present study assessed safe delivery services utilization and associated factors among mothers who gave birth during four years preceding a survey conducted in Bangladesh Demography and Health Survey 2004. The objectives of this study were (1) to investigate the selected demographic, socioeconomic, cultural and programmatic factors associate with safe-delivery practices in rural Bangladesh and (2) assess women's attitudes and practices concerning birth attendants and place of delivery Methodology Data Source The study intends to examine or investigate the selected demographic, socio-economic, cultural and programmatic factors associated with safe-delivery practices in rural Bangladesh. The study was based on the secondary data of the national-level drawn from the Bangladesh Demographic and Health Survey (BDHS) 2004 (10). The sample for this analysis consisted of 3874 ever-married rural women aged 10-49 years, who had at least one delivery four years preceding the survey while women who did not have any delivery before the interview were excluded from the analysis. Analysis Descriptive statistics and multivariate analysis (especially logistic regression model) were employed in analyzing data. In this regard, safe-delivery practices refer to a delivery assisted by a medically trained person (MTPs), such as doctors, nurses, paramedic and trained Traditional Birth Attendants (TBAs). To examine the effects of selected demographic, socioeconomic, cultural and programmatic factors on the safe-delivery practices of rural women, a logistic regression model was used. In this model, the dependent variable is: delivery assisted by a (MTP)during last delivery (dichotomous variable). The independent variables are: age, division, education of respondent, education of the respondent's husband, employment status, religion, prior visit to healthcare facilities such as visit to satellite clinic, and ownership of TV and radio, read newspapers or magazines, listen to radio and TV etc. The statistical package programme SPSS for windows release 11.0 was used for all statistical data analysis. Microsoft Excel programme was used for graphical presentation and Microsoft Word was used for typing literature and formatting tables. Limitations Besides the selected demographic, socioeconomic, cultural and programmatic factors which have been included in this analysis, a host of other programmatic factors such as accessibility, quality and cost of delivery services, cultural factors as well as religiosity, prejudices, women's role in decision making process, subordinate status of women etc. are also likely to influence the delivery practices of rural women. However, due to lack of relevant data the effects of these programmatic and cultural factors on the delivery practices could not be examined in this paper. Also the available data did not permit us to examine all aspects of the delivery practices. Results Sample characteristics The background characteristics of the samples are shown in (Table-1). The majority of the women (about 76%) are less than 30 years of age. More than 40 percent of the women are uneducated. Higher education is very low for both the respondents and their partners. The divisional variation of the number of the women is proportional to their total population, highest the Dhaka and Rajshai and lowest the Barisal and Sylhet. Most of the women were housewives, and 16 percent of them worked for earning. More than one-third (33.2%) of the women reported that they owned a radio while 20 percent reported to have owned a television. More than 90 percent of the women are Muslims. Reading of newspapers and magazines is very low, only 13 percent of respondents read any type of newspapers. Listening to radio and watching television is reasonable accounting for 44 and 47% respectively. Regarding prior exposure to the healthcare centre, over half (59%) of the women visited a satellite clinic (SC) before their last delivery. Delivery practices Almost all the deliveries (Figure-1) 94% took place at homes (it may be respondents own home or her father's or relative's or neighbour's or friend's house). Only 4% of the deliveries took place at the government arrangements, such as hospitals, Thana Health Centres (THCs) and Maternal and Child Welfare Centres (MCWCs). On the other hand about 2% of the deliveries were conducted at the private level, such as NGOs satellite clinic, private hospital/clinics and/or other private places. Most deliveries were assisted by the untrained traditional birth attendants (UTBAs) called Dai, while relatives, neighbours, friends, and others constituted 67% and 10% respectively. The qualified doctors, nurses, family welfare visitors and paramedic assisted 9% of the deliveries while about 13% are by the trained traditional birth attendants (TTBAs). We found that about 1% of deliveries took place without attendants. This observation indicates the alarming situation prevailing in the rural areas where delivery takes place as well as the type of attendants. Logistic regression model and variables used in the model To identify the influencing factors thought to be the cause of safe-delivery practice in rural Bangladesh, logistic regression analysis was used. It is similar to a linear regression model but is suited to models where dependent variable is dichotomous. The data for this study satisfy the conditions of unconditional logistic regression model. Let Yi represent a dichotomous variable that equals 1 if the women's delivery assisted by the (MTPs) during last delivery and 0 if the women's delivery assisted by the others category. The probability of women's delivery assisted by the (MTPs)during last delivery Pr (Yi = 1) , is the cumulative density function F evaluated at Xi β, where Xi is a vector of independent variables and β is a vector of unknown parameters. This kind of probability function has the following form.
The estimation form of the logistic transformation of the probability of women's to assisted by the medically trained persons, Pr (Yi = 1) can be represented as:
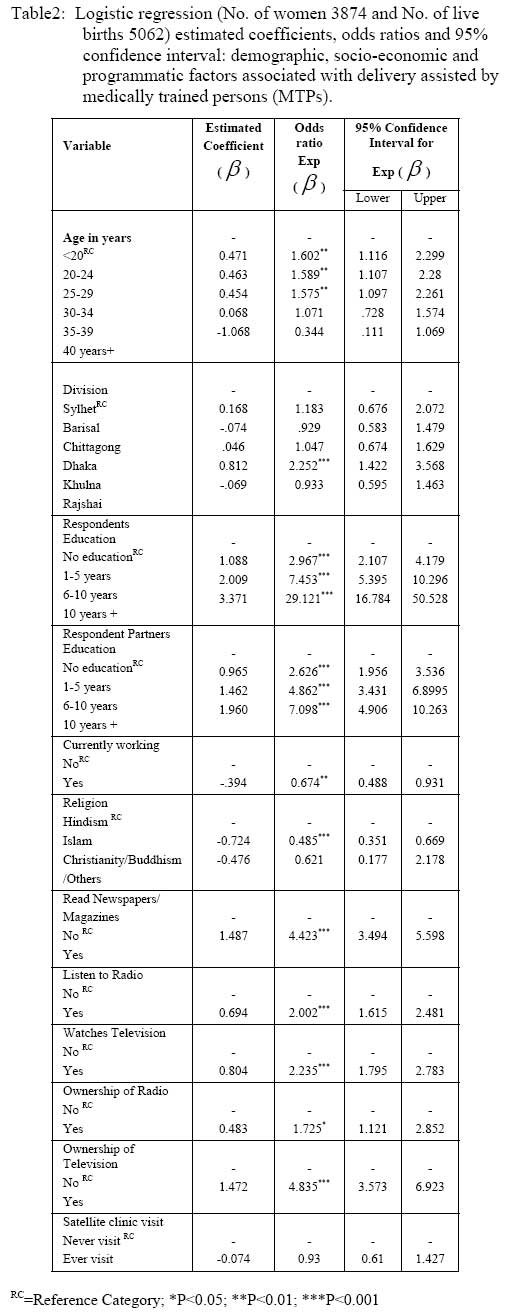
The independent variables are: x1 = Age in years, x2 = division, x3 = Respondents Education x4 = Respondent's Partner Education x5 = Currently Working, x6 = Religion x7 = Read Newspapers/ Magazines x8= Listen to Radio, x9= Watches Television x10= Ownership of Radio x11= Ownership of Televisios x12= Satellite Clinic Visit In rural Bangladesh, most deliveries take place at homes and are assisted by Untrained Traditional Birth Attendants (UTBAs), Dai, relatives or neighbours generally in unsafe and unhygienic conditions. Only a small proportion of the deliveries are assisted by MTPs, such as qualified doctors, nurses, paramedics and Trained Traditional Birth Attendants. To investigate the selected demographic, socioeconomic, cultural and programmatic factors associated with delivery assisted by the MTPs, a logistic regression analysis was done. In this analysis, the dependent variable was: delivery assisted by MTPsduring last delivery (dichotomous variable). The independent variables included a number of selected demographic, socioeconomic, cultural and programmatic variables. (Table-2) presents the results of the logistic regression analysis. The results show that the likelihood of the delivery assisted by the MTPs was higher up to 34 years of age and then declines in the same order. The 20-24 years age-group had the highest probability of having their deliveries assisted by the MTPs. The age categories 20-24, 25-29 and 30-34 are more than double the probability of having their deliveries assisted by the MTPs of the reference category (<20) and 95% confidence intervals are statistically significant. Divisional variation is insignificance except for the khulna division. Khulna division is highly significant of having the delivery assisted by the MTPs as the reference category of the Sylhet division. Barisal and Dhaka had also higher chance of delivery assisted by the MTPs. As expected, education had direct effect on delivery practices. The uneducated women were less likely to have their delivery assisted by the MTPs. All the categories of education except the no education were highly significant with some confidence interval. The women with 10 or more years of schooling had 29 times higher probability of having their deliveries assisted by the MTPsthan the uneducated women. The other categories like 1-5 and 6-10 years of schooling had 3 and 7 times higher probability of having their deliveries assisted by the MTPsthan the uneducated women. Partner's education also directly influenced significantly delivery practices in rural settings. The higher the partner's education the higher the chance of having delivery assisted by the MTPs. From regression analysis it is clear that women married to husbands with education of more than 10 years of schooling had 7 times higher chance having delivery assisted by MTPs. The currently working status significantly influenced delivery assisted by the MTPs. Religion was significantly associated with the safe-delivery practices. The Hindu women had about 50 percent higher probability of having their deliveries assisted by the MTPs. There is a possible explanation of this. The Hindus are less conservative than the Muslims, which lead them to have their deliveries assisted by the medically trained persons in a relatively higher proportion than the Muslims. The reading of news papers/ magazines directly influences the delivery practices in the rural areas. The co-efficient is highly significant. There is a more than 4 times higher chance of probability of delivery assisted by the MTPs than that of women with no reading of newspapers or magazines. Listening to radio and watching television also influences significantly delivery practices in rural areas. The women who listen to radio and watch television had more than 2 times higher probability of having delivery assisted by the MTPs than that of non-users counterpart. Ownership of ratio was significantly associated with the safe-delivery practices in rural Bangladesh. Those women who had radio had 1.7 times higher probability of having their deliveries assisted by the MTPs. Those women who had TV had about 5 times higher probability of having their deliveries assisted by the MTPs. The possession of TV could be interpreted as a property indicator, and as such, the effects of exposure to TV could also be a function of high-economic status. However, due to lack of data on income or economic status, we could not examine the effects of economic status on safe-delivery practices. Results from the satellite clinic visit are insignificant. Discussion The findings of this analysis has shown that almost all the deliveries took place at home, and the medically untrained persons, such as TBAs, relatives, or neighbors, assisted 77 percent of these deliveries and are likely to be done in unsafe and unhygienic conditions, which often result in delivery-related complications leading to maternal and neonatal morbidity and mortality. The results of our analysis show that only 13 percent of the deliveries were assisted by the trained TBAs. This emphasizes the need for linking the trained TBAs with the health services systems to ensure maximum use of the services of the trained TBAs. It appeared from our analysis that, like many developing countries, more than 65 percent of the deliveries were assisted by the untrained TBAs. The results apparently reveal that only 6 percent of deliveries took place in the government hospital and NGOs clinics. It is also an alarming situation that only 9% of the deliveries were assisted by the MTPs. One percent of deliveries had no attendant, this indicates the poor rural infrastructure on medical facilities. The regression results show that the uneducated women and women aged less than 20 years or aged over 34 years are less likely to have their deliveries assisted by a MTP. This underscores the need for appropriate behaviour change communication (BCC) strategies to make the community particularly the uneducated women, and relatively younger or older women aware of the benefits of safe delivery by MTPs. The partner's education also directly affects the safe and hygienic deliveries in rural areas, the lower the education of partner the lower the chance of delivery assisted by MTPs. Religion is also significantly associated with delivery practices. Muslim women are less likely to have their delivery assisted by MTPs probably because of their conservatism and religious taboos (which might be one of the probable reasons). Appropriate BCC activities need to be undertaken to overcome conservatism and religious taboos against delivery. The regression results reveal that reading of newspapers/magazines, listening to radio and ownership of radio directly affects the delivery assisted by the MTPs. Our study also has shown that exposure to television was significantly associated with the safe-delivery practices. However, it could be suggested that BCC activities through electronic media, such as television, should be intensified on the message of the benefits of safe-delivery practices to reach the community. Finally, there is a need for further investigation to examine the effects of some programmatic (e.g. accessibility, quality, and cost of delivery services) and cultural factors (e.g. religiosity, prejudices, women's role in the decision-making process, subordinate status of women, etc.) on the safe-delivery practices of the rural women. Making motherhood a safer time in women's lives requires commitment at all levels, in the home, in the community, in the clinic, in the country, and at the international level. This is a commitment to reducing inequities, improving women's autonomy, and ensuring that motherhood is a safe, joyful, and rewarding experience. The GoB should ensure skilled attendance at birth, identifying appropriate cadres, training the required numbers and ensuring back-up services. Good quality maternal health care is the single most important intervention to prevent maternal and newborn morbidity and mortality. Maternal health services, including essential obstetric care for complications, must be made available to all women during pregnancy and childbirth. Public education programmes, at national and community levels, should focus on the following supportive actions: Improving nutrition for girls and women; facilitating women's access to maternal health care during and after pregnancy and delivery; educating women and families to recognize and respond to emergency situations; and ensuring that women get the rest they need during pregnancy and after delivery. Policy should be made to create awareness regarding safe delivery among people belonging to different social milieu. Mass media particularly print and audio-visual can play a vital role in providing knowledge about the consequences of unsafe delivery. More research should explore reasons for unsafe delivery from the cultural perspectives and also other related health issues to provide better guidelines for planners, administrators and policy makers. Acknowledgements The author is extremely thankful to Dr. Md. Mobarak Hossain Khan, Assistant Professor, Department of Public Health Medicine, Bielefeld University, School of Public Health, Germany for his comments and suggestions on the draft version of the paper. The work of Dr. Khan is ever memorable and the author is grateful to him. Thanks are also due to Professor Dr. Mahmooda Ghani Ahmed, Dean, Faculty of Mathematical & Physical Sciences, Jahangirnagar University, Savar, Dhaka, Bangladesh for giving the permission and funds to conduct the study. References
© Copyright 2007 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp07015t2.jpg] [lp07015f1.jpg] [lp07015t1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}