 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 5, No. 1, April, 2008, pp. 22-25 Prevalence and Correlates of Condom Use at Last Sexual Intercourse Among In-School Adolescents in Urban Areas Of Uganda J.M. Twa-Twa1, S. Oketcho2, S. Siziya3*, A.S. Muula4 1 School Health Section, Ministry of Health, Kampala, Uganda Received 18 August 2007; Revised 23 February 2008; Accepted 28 February 2008 Code Number: lp08006 Abstract Objectives: Correct and consistent condom use remains
an important public health intervention against the spread of Human
Immunodeficiency Virus and other sexually transmitted infections. There is
paucity of information on sexual behaviour of in-school adolescents in Uganda. We, therefore, used secondary data of the Uganda Global School-based Health Survey
(UGSHS) conducted in 2003 to determine the prevalence and correlates of condom
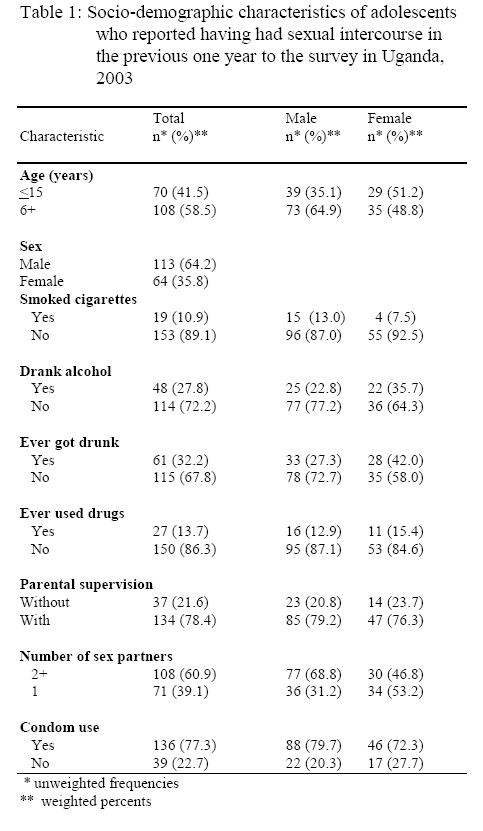
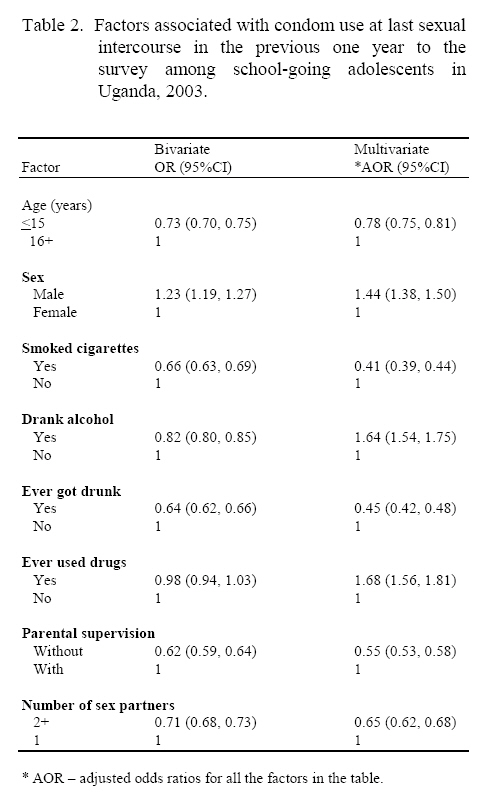
use at last sexual intercourse in urban areas of Uganda. Keywords: Prevalence, Correlates, Condom use, Adolescents, Uganda Introduction Adolescents are a critical target group for sexual behavioural change programs. In eastern and southern Africa Human Immunodeficiency Virus (HIV) transmission is largely spread heterosexually. While sexual abstinence is the preferred method of HIV prevention among adolescents, this is not practicable to many adolescents. Therefore correct and consistent condom use among this age group is a reasonable effective method of preventing the transmission and acquisition of HIV and other sexually transmitted infection. Uganda is among the few African countries that have reported a decline in HIV prevalence (1). Such decline in HIV prevalence may have been due to many reasons including positive change, such as delay in sexual debut, increased condom use and limiting number of sex partners that have potential to limit the occurrence of incident of HIV cases. Some studies however have questioned that delay in sexual debut has occurred to a significant degree. Gersovitz (2) and Zaba et al (3) have reported that misreporting of sexual behaviour may have contributed in part to the reported delay in sexual debut in Uganda (2,3). Despite these differing assertions as to what may have caused the decline in HIV prevalence in Uganda, consistent condom use will continue to be an important public health intervention against the spread of HIV and other sexually transmitted infections. We are however unaware of any published studies that have reported on the prevalence and correlates of condom use among in-school adolescents in Uganda. We therefore carried out this study to assess the prevalence and socio-demographic correlates of reported condom use at last sexual intercourse among sexually active school-going adolescents in urban areas of Uganda. Methods This study is based on the Uganda Global School-based Health Survey (GSHS) conducted in 2003. The GSHS was developed by the World Health Organization (WHO) in collaboration with UNICEF, UNESCO, and UNAIDS with technical assistance from the Centers for Diseases Control and Prevention (CDC), Atlanta, Georgia, United States. The aim of the GSHS is to provide data on health and social behaviours among in-school adolescents aged 13-15 years. In case of Uganda, these adolescents were mostly in senior Grades S1 to S3, and included adolescents of age less than 13 years and more than 15 years. A two-stage cluster sampling technique was used to draw a representative sample of students in senior Grades S1-S3 in government and private secondary schools in Uganda. In the first-stage, the sampling frame consisted of all secondary schools (government and private schools) containing any of S1, S2, S3 grades. The schools which were our primary sampling units were selected with a probability proportional to their enrolment size. In the second step, the sampling frame consisted of all classes in each selected school. A systematic sample of classes in the selected school was obtained. All students in the selected classes were invited to participate. The selection of the schools was done using a standardized method developed by WHO/UNICEF and CDC for all the Global School-based Health Surveys. Uganda has about 3000 secondary schools of which about 1400 are urban based. Students not attending senior secondary 1-3 were excluded from the study. The study included both urban and rural schools. In the study there were 25 rural and 25 urban schools. This paper is about urban schools that included both privately owned and public schools. The response rates were 88% for schools and 80% for adolescents. The 20% of the adolescents who did not respond were either absent from school at the time of the survey or refused to take part in the study, although they were present in school. A standardized GSHS questionnaire was used to collect the information and completion of the questionnaire occurred within one class period. The questionnaire was carefully adapted and piloted in one district. Since in Uganda, English is the language used in schools from Primary 4, the questionnaire was in English. Administration of the questionnaire was done by youth who had completed senior six or were in their first year in university. There were 93 questions in the questionnaire, and all the questions were close-ended. The sections of the questionnaire included: demographics, alcohol, tobacco and drugs, HIV/AIDS, physical activity, violence/physical fights, diet/nutrition, hygiene practice, and protective factors. Data that we used for this study included variables on having had sexual intercourse within the last 12 months, marijuana use, having ever drunk alcohol, cigarette smoking, gender, having ever been drunk and adolescents’ own assessment of parental supervision. Some of the questions asked were: During the past 12 months, have you had sexual intercourse? (Yes/No). During your life, how many times have you used cannabis? Study participants who indicated at least one time of use were re-coded as 1, else 0. Other questions were: During your life, how many times did you drink so much alcohol that you were really drunk? During the past 30 days, on how many days did you have at least one drink containing alcohol? Data analysis Data analysis was restricted to those adolescents who reported having ever had sexual intercourse. Analysis was performed using SPSS version 14.0 software. A weighting factor was used in the analysis to reflect the likelihood of sampling each student and to reduce bias by compensating for differing patterns of non response. We obtained frequencies as estimations of prevalence rates of condom use at last sexual intercourse (outcome variable) as well as selected socio-demographic characteristics. We conducted a backward logistic regression analysis to determine factors independently associated with the outcome. We report both the unadjusted odds ratios from bivariate analyses as well as the adjusted odds ratios from a multivariate analysis. Ethical Considerations The National Council of Science and Technology reviewed and approved the survey protocol. While informed consent was obtained from children of age 18 years or more, assent for children to participate in the survey was given by District Educational Departments and School administration. The research was non-invasive. Questionnaires were anonymously completed by the students. All study participants were informed that they were free not to participate or not to respond to any of the questions if they felt uncomfortable with the questions. Results Description of study participants Out of a total of 1709 students whose data were available, 11.3% (14.9% of male, and 7.9% of female) adolescents had sexual intercourse within 12 months prior to the survey. Table 1 shows the socio-demographic characteristics for the adolescents who had sexual intercourse. Most of these adolescents were males (64.2%), and were of age 16 years or more (58.5%). Female adolescents tended to drink alcohol (35.7% of females, and 22.8% of males), and ever got drunk (42.0% of females, and 27.3% of males) more than males. Overall 13.7% of the adolescents had ever used drugs. About three quarters (77.3%) of the adolescents used a condom at last sexual intercourse. Factors associated with condom use at last sexual intercourse Table 2 shows factors that were associated with condom use at last sexual intercourse. Results of the bivariate analyses and multivariate analysis were similar for all the factors except drank alcohol and ever used drugs. Both variables were risk factors in bivariate analyses and they were protective factors in the multivariate analysis. We highlight the results from the multivariate analysis. The risk factors that were identified were being male, having drank alcohol, and ever used drugs. Male adolescents were 44% (OR=1.44, 95%CI 1.38, 1.50) more likely to have used a condom compared to female adolescents. Adolescents who drank alcohol were 64% (OR=1.64, 95%CI 1.54, 1.75) more likely to have used a condom than adolescents who did not drink alcohol. Compared to adolescents who never used drugs, adolescents who used drugs were 68% (OR=1.68, 95%CI 1.56, 1.81) more likely to have used a condom The following variables were identified as protective factors: being of age less than 16 years, current cigarette smoker, ever got drunk, and lack of parental supervision. Adolescents of age less than 16 years were 22% (OR=0.78, 95%CI 0.75, 0.81) less likely to have used a condom compared to adolescents who were of age 16 years or more. Compared to adolescents who did not smoke cigarettes, adolescents who smoked cigarettes were 59% (OR=0.41, 95%CI 0.39, 0.44) less likely to have used a condom. Adolescents who had ever got drunk were 55% (OR=0.45, 95%CI 0.42, 0.48) less likely to have used a condom compared to adolescents who had never got drunk. Adolescents who did not receive parental supervision were 45% (OR=0.55, 95%CI 0.53, 0.58) less likely to have used a condom compared to adolescents who reported receiving parental supervision. Finally, adolescents who ever had 2 or more sex partners were 35% (OR=0.65, 95%CI 0.62, 0.68) less likely to have used a condom. Discussion This study found that 11.3% of in-school adolescents reported having had sexual intercourse within 12 months prior to the survey. A minority (39.1%) reported having had a single sex partner while 60.9% reported having more than one sex partner. Prevalence of condom use at last sexual intercourse was 77.3%. In bivariate logistic regression analysis, we found that being 15 years or younger, female, being a cigarette smoker, used alcohol or history of having been drunk, lacking parental supervision were associated with not having used condoms at the last sexual intercourse. In multivariate analysis, lack of parental supervision, age 15 years or younger, being a cigarette smoker, having gotten drunk were all associated with non-use of condoms at last sexual intercourse. Use of drug, alcohol and male gender were all associated with greater likelihood of having used condoms at last sexual intercourse. Tho le et al (4) have reported that among Thai young men, alcohol was associated with sexual experience. Also young men who used alcohol were less likely to use condoms compared to those not using alcohol. Bryan et al (5) have reported that the clustering of alcohol use and sexual experiences may be due to that individuals who seek both may be prone to sensation seeking. Abbey et al (6) have reported that college students in the United State s were less likely to use condoms with casual sexual partners when intoxicated with alcohol. In our multivariate analysis however, alcohol use was associated with condom use. Although alcohol has been reported as a social disinhibitor, we suggest that situations where adolescents in Uganda take alcohol may also be associated with condom availability and usage. This may be plausible when we consider that condom messaging has been particularly targeted at drinking places in Uganda and other east and southern African countries. However, although condoms may have been accessible in drinking places, they may not have been used because patrons may have been too drunk to use them. We found that males were more likely to have reported condom use at last sexual intercourse than females. The reasons as to why this may be the case are not precisely known. It is possible that this disparity may be a result of intergenerational sex where adolescent girls are having sex with older males outside their age group. Girls may also not know whether their partners have put on the condom before having sex with them. It is also possible that males may be over-reporting or the females under-reporting actual condom use. Jeannin et al (7) have reported that although the validity and reliability of sexual intercourse and condom use reporting among Swiss study participants was good, over-reporting of condom use was observed. Of particular concern is the finding that adolescents who reported having more than one lifetime sex partner were less likely to have used condoms. Although the survey did not specifically seek information on concurrency (having more than one sex partners within the same period), it is possible that some adolescents in our study may have had concurrent sex partnership. Multiple sex partnerships and concurrency are risk factors for HIV transmission (8,9). It is therefore of concern than having had more than one sex partner was associated with non-use of condoms at last sexual intercourse. Our study found that adolescents who reported receiving parental supervision during their free time were also more likely to use condoms at last sexual intercourse. Cox (10) has reported that African American adolescents were more likely to have used condoms if they had high levels of parental supervision. Parental supervision was however not associated with condom use among White adolescent Americans. Borawski et al (11) also reported that among adolescents in the United States, high parental monitoring was associated with less alcohol use and consistent condom use among males but not among females. This may suggest that parental supervision may be effective in some groups of people but not in others. Conclusions We conclude that parental supervision may be effective in promoting condom use among adolescents in our study population. Furthermore, although drinking alcohol was associated with condom use, probably due to peer pressure and easy access to condoms in drinking places, condoms may not have been used by the patrons because they may have been too drunk to use them. Competing interests The authors declare that they have no competing interests. Acknowledgements We thank the World Health Organization (WHO) [Geneva] and Centers for Disease Control, Atlanta, Georgia, and United States, for financial and technical support. We are also grateful to the WHO country office, Uganda for facilitating the collection of data. To the Ministry of Health, and Ministry of Education and Sports who allowed and supported the study to take place, we say many thanks. Last but not the least we would like to give our thanks to the students for participating in the study without which this study could not have been successfully completed. References
© Copyright 2008 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp08006t2.jpg] [lp08006t1.jpg] |
| |||||||||

{kind=link}
{kind=link}