 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 5, No. 2, August, 2008, pp. 79-85 Status And Visions For The School Health Service As Reported By Local Health Care Workers In Northern Tanzania Astrid Merete Borge1, Rachel N. Manongi2, Melkiory C. Masatu3, Knut-Inge Klepp4 1Bergen University College, Faculty of Health and Social
Sciences, Bergen, Norway, 2Kilimanjaro Christian Medical College
(KCMC), Moshi, Tanzania 3Center for Educational Development
in Health, Arusha (CEDHA), Tanzania, Center for International Health, University
of Bergen, Norway 4Department of Nutrition Research, University
of Oslo, Norway. E-mail:k.i.klepp@medisin.uio.no Received 24th May 2007, Revised 22nd May 2008, Accepted 30th May 2008 Code Number: lp08016 Abstract: Objective: The World Health Organization’s (WHO) Global School Health Initiative provides a strategy to utilize schools to promote health
and reduce the burden of diseases worldwide. The aim of this study was to
investigate local school health work in Tanzania in relation to existing
national guidelines and the WHO initiative. Introduction The World Health Organization’s program “Global School Health Initiative” is designed to improve the health of students, school personnel, families and other members of the community (1). A worldwide effort is evident from the report “Promoting Health through Schools,” which describes intervention programs implemented from 1985 to 1996 (2). However, only one program is reported from the African continent (3). Furthermore, while a large number of studies on the organization and implementation of school health services have been conducted in various countries, few such studies are available from Africa (4,5). No published reports presenting the perspective of health care workers regarding the quality and extent of school health services in an African context has been identified. Tanzania is one of the poorest countries in the world. Infectious diseases, including HIV/AIDS and malnutrition are common health problems (6,7), and non-communicable conditions, such as heart and circulatory diseases, are on the increase in urban areas (8).Officially, Tanzania claims to have a holistic, multidisciplinary and integrated approach to its primary health care, involving intersectoral collaboration and full community involvement (9).In accordance with the Ottawa Charter and other WHO recommendations (10,11,12), the Tanzanian national health policy strongly emphasizes disease prevention and health promotion rather than curative care (13). School health services in Tanzania date back to 1921 (14),while the year 1967 marks the start of the independent Tanzania’s Primary Health Care Strategy, based on WHO’s definition of health, including children’s health (15). Tanzania’s current health system includes school-based health promotion as a part of a decentralized system (14,16). The guidelines for implementing the National School Health Program include an organizational chart at village, district, regional, zonal and national levels, and present job descriptions for school health program coordinators at all levels (14). “Mpango wa Taifa wa Ukusanyaji wa Takwimu za Afya” (MTUHA) (i.e. in English “Health Management Information System”) is a national system for collection of statistical health data that health institutions all over the country have been required to use since 1995 (17). More than half (57%) of the Tanzanian population is under 20 years of age, and 70 to 80% of school-age children are enrolled in primary school (the number of boys and girls is nearly equal) (7). In secondary school, the percentage of children enrolled is reduced to less than 30%, and boys are in the majority (7). Thus, primary schools clearly represent an important arena for health promotion efforts targeting Tanzanian children. Tanzania is one of five participating developing countries in “Partnership for Child Development” (18), but to date, no comprehensive study of the school health service has been conducted in Tanzania. Consistent with previous recommendations, this study aims to investigate local school health services, applying WHO’s School Health Initiative (1,2,3) as a guiding framework. Thus, the objectives are: (a)
To assess local health
workers’ opinions about health, local health problems and risk factors among
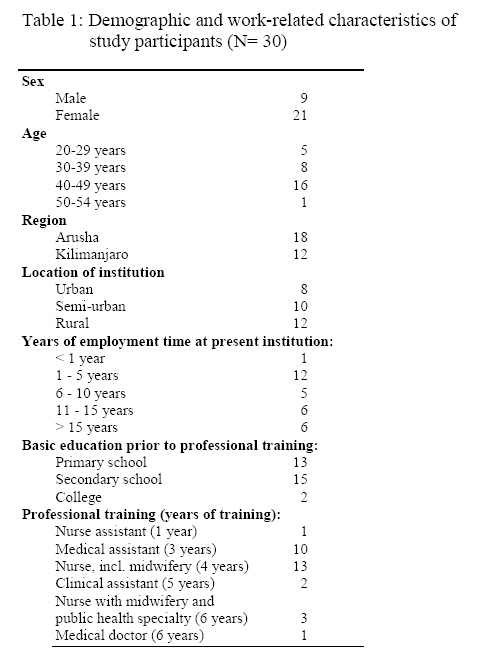
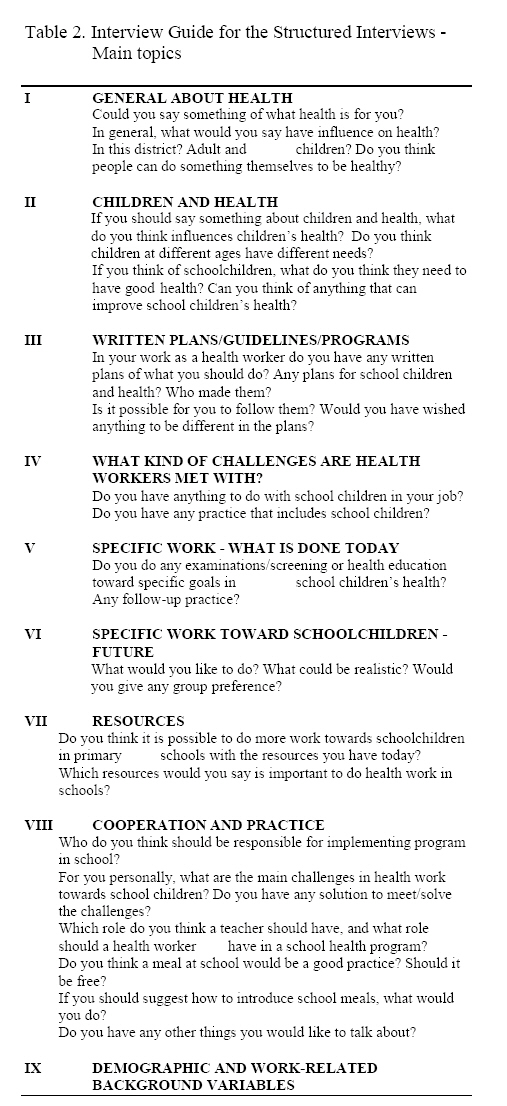
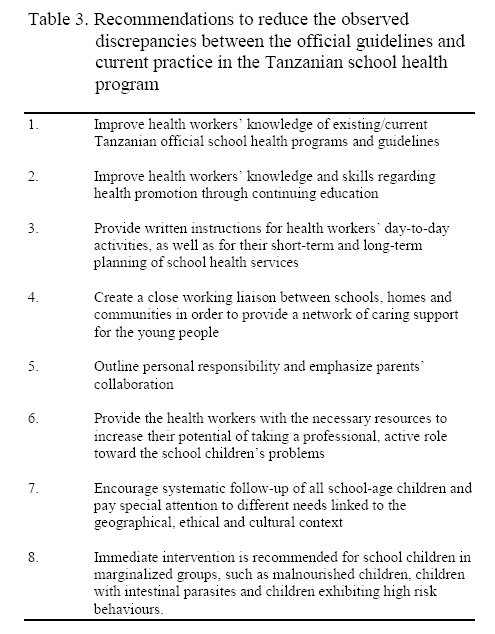
school children. Methods Study Population The study population consisted of health workers located in urban, semi-urban and rural school districts in the Arusha and Kilimanjaro regions of Northern Tanzania. We recruited health institutions (dispensaries, health centres and hospitals) that are geographically linked to 18 schools that previously participated in the Ngao study (19). We interviewed two health workers from each institution (in Tanzania, no health care workers are employed within the schools themselves). The head of each participating health institution chose health workers who carried responsibility or had experience with school health activities to serve as participants in the study. The number of staff at the health institutions varied from two (small dispensary in a rural area) to 42 (regional hospital with a Mother and Child Health Clinic). Several of the health institutions served more than one school. We interviewed a total of 30 health workers — 21 women and 9 men. Demographic and work-related information is presented in Table 1. In Tanzania, a medical assistant has three years of education following secondary school. Assistant medical officers have an additional two years of training, and usually work as medical doctors. A nurse trains for three years following secondary school, with a fourth year in order to obtain a specialty in midwifery or psychiatry. Public health care and health education with practice in urban and rural communities is integrated in the curriculum. It is possible to get a one year advanced diploma in health education and public health in Tanzania. Study Design The study was conducted as a cross-sectional qualitative interview survey of school health personnel with direct observations of the physical environment at participating health institutions. The study was part of a larger comprehensive study, “Healthy Schools: Health System Research Approach to Investigate Health Promotion Among Primary School Children,” which is a follow-up study of teachers and students in the 18 schools that previously participated in the Ngao AIDS education study (20). Research Instrument and Procedures We used a semi-structured interview guide (21,22) and the key topics addressed are outlined in Table 2. We developed the interview guide in collaboration with Tanzanian health workers, revised it in collaboration with Tanzanian health professionals working within community health, and subsequently tested the guide in a pilot exercise. The project staff visited the health institutions some weeks prior to beginning the interviews in order to provide information to participants about the study and to obtain consent for participation. To avoid taking undue advantage of respondents’ time, the duration of the interviews was limited to one hour. However, we always included the culturally important “kuzungumza,” a chat before the formal interview started, as well as a debriefing after the completed interview. The interviewer (A.M. Borge) kept centred on the purpose of the study by using the semi-structured interview guide quite strictly. The respondents all understood English, but in order to allow them to express themselves in their own language (Swahili), an interpreter was used. We informed the respondents at the start of the interview about the main focus of the interview and of the researcher’s need to take notes. We did not tape-record the interviews. The interviewer asked all participants the predetermined questions in the same order and never interrupted or stopped participants during their responses. Every new question was asked in an open-ended format. Thereafter, depending on the respondent’s answer, follow-up questions were asked. Finally, the interviewer read the predetermined response alternatives and asked participants to choose the alternative that most closely corresponded to his or her personal view. The final question in every interview was: “Do you have any other thing you would like to tell about?” Observation of the health institutions’ facilities focused on access to water supply, sanitation, equipment and hygiene. Video recordings were made from the health institutions and the schools linked to them. Observation was not an essential part of the study, but was included as a potential tool for validation of the respondents’ reports. Data Analysis The transcription of the field notes started immediately after every two interviews. This process also included some analysis and interpretation in collaboration with the interpreter. The analyzing and interpreting process went back and forth, emphasizing the importance of presenting the respondents’ understanding in a theoretical context (21,22). By the end of the fieldwork, we transcribed the written notes once more and compared them to the first transcription. First, we analyzed each interview separately. The main categories in the interview guide provided sufficient classification for this phase of the analysis, and no new categories were generated. Second, we sorted the data from all interviews under various categories/topics and interpreted the data with emphasis on possible common patterns, similarities and divergences. Third, we generated the categories seen in the Results section in order to describe some of the main findings from the study. Results Definition of Health and Health Problems When asked about the concept of health, all participants gave definitions consistent with the definition provided by WHO (i.e., including physical and psychosocial well being, and not only absence of disease). In response to follow-up questions concerning factors that influence health, participants described the relevance of poverty, lack of education and lack of food. Concerning local health problems, all participants mentioned infectious diseases. Furthermore, health workers in urban and semi-urban areas mentioned family problems, parents’ neglect of their children, school dropout rates, and teenage pregnancies as serious problems seen locally. In semi-urban and some rural areas, participants mentioned the seasonal lack of water as a threat to all people’s health because the lack of water leads to infections due to intestinal parasites, and skin, eye and respiratory problems. Observational data from both school and health institutions confirmed these statements. Factors that were said to produce serious health problems in the rural parts of Arusha were related to the dry season — shortage of good soil to establish a garden, lack of water — and “the traditional way of living.” Observation of children in this area showed clear clinical symptoms of malnutrition and skin problems. The “traditional way of living” was said to negatively influence the children’s health as eating habits (no meat, mostly maize porridge) cause malnutrition, and risky sexual behaviour results in sexually transmitted diseases at a young age. When asked where people could find help with health-related matters, participants indicated that local leaders play an important role in people’s lives. Participants had low expectations of receiving help from the government: “ The government is poor,” “The country has no money,” were statements given by a majority of the health workers. However, participants indicated that drinking water was one area that is clearly the responsibility of the government. Perceived Needs of School Children The health workers’ initial response when asked about the needs of children was always to refer to children from 0-5 years of age. On the specific question: “If you think of school children, what do you think they need in order to have good health?” several respondents gave statements such as “School children are not bad at all,” “School children usually are healthy,” “They get treatment if they are sick”. On further probing about needs or problems school children might have, the suggestions were similar to those quoted above, referring to factors influencing people’s health in general. Practice towards School Children Twenty-five of the 30 respondents reported not having any written plans to guide their work directed toward the health of school children. The remaining five respondents all referred to the National School Health Program (14) as guiding their work. A few of the respondents were familiar with the national health program from the Ministry of Health and Ministry of Education. These programs have no specific instructions concerning school health services. A majority of the respondents saw MTUHA (17) as the only work plan. This registration system was known and used with satisfaction by all. Seven of the 30 participants reported that they visited one or several schools during a year. None of these participants had systematic cooperation with the schools or visited the schools on a regular basis. Their work in schools included observation of the physical environment, medical examination and observation of the children, checking of BCG scars, vaccination and health education. The 23 respondents who reported not visiting schools at all gave lack of resources (insufficient staff, lack of time, long distances to schools, no transport available, and no money for transport and food) as their main reason for not visiting the schools. Also, a majority of the health workers stated that school visits were not included in their daily timetable. Some of the respondents reported that before MTUHA (17) was introduced, schools were visited regularly. No differences were seen between urban, semi-urban and rural districts with respect to school visits, and health workers employed at the same health institution gave consistent information concerning their contacts with schools. Schools located close to a health institution were not visited more often than schools located farther away. Only one institution used written records to follow-up school children. At two institutions health workers reported that they followed-up children older than 5 years if they knew that the children had specific problems (e.g., malnutrition). Other institutions reported not to follow-up children older than 5 years of age. According to the respondents, disabled or chronically ill children received care from hospitals. Respondents reported that the only specific activity toward physically disabled children was a project in a rural area of Kilimanjaro region. This project was run by a non-governmental organization and aimed to rehabilitate physically disabled children. Respondents considered children with social, learning, or behavioural problems to be problems for teachers, not for health workers. Respondents reported that teachers provide health education for children at school, thus it was not planned on a regular basis by any of the respondents. Some health workers reported to cooperate with teachers and visit schools when they were invited. Many of the health workers reported that they did not know what was included in the health education provided in schools. The following statements are common responses to the question about cooperation with schools: “The teachers want us to help them. I have not done that yet.” “If I’ll be invited, I’ll go to school.” “Children come to the dispensary.” Visions for School Health Medical Examination and Treatment We asked the health workers to give their suggestions for future school health programs. When asked about screening, all interviewees spontaneously gave screening top priority, including physical “top to toe” examinations looking at sight, hearing, height, weight, skin, teeth and nutritional status. Examination of urine, faeces and blood was recommended by the majority of respondents, but was said to be unrealistic due to lack of equipment. With two exceptions, all respondents voiced that medical personnel should perform the physical examinations, and most stated that a group of nurses was necessary. Nearly all respondents expressed that health workers should conduct regular screenings at school for grades 1, 3 and 7. There were no differences in statements among health workers from urban, semi-urban and rural districts. Health workers reported that matters related to psychology, learning, social life and behavior are outside their arena. “Others can take care of this” was indicated by several, and specifically it was suggested: “Teachers know more than me” and “Village leader or social workers can help.” The issue of health education was brought up spontaneously several times during each interview. All respondents expressed the view that health workers should take part in planning and providing health education to the school children in cooperation with the schools. Most of the health workers responded that teachers should be responsible for teaching health issues in general, while health workers should provide health education related to specific diseases. Health workers should visit schools if required, for example if an epidemic should occur. Health workers could even train and educate the teachers. Themes such as nutrition, cleanliness, hygiene and infectious diseases were brought up repeatedly by the participants. When the respondents were specifically asked to offer suggestions on the content of health education, HIV infections were given high priority. Most of the interviewees considered it important to teach about family life and maturity. However, many felt education of this kind should be restricted to students in grade 6 and above, and some participants indicated that they would obtain parents’ consent prior to addressing these issues: “Parents have to agree on things like that.” Several health workers stated: “It is all taught about when they learn about HIV and AIDS.” All respondents indicated that teaching about family planning is important, but some thought only girls should receive such information. No respondent referred to traditional medicine unless specifically asked about it. When asked, the majority revealed a willingness to include matters related to traditional medicine in their efforts; however, they would not promote it, but rather warn against it. A minority of respondents did not want to bring this topic into health education: “They learn from parents. They know it.” Responses differed when questions were raised about the use of alcohol, tobacco and drugs. Health workers in urban and semi-urban districts near towns or main roads considered such information to be important. In rural districts, health workers did not perceive drug problems to exist, and consequently did not find it necessary to include information about them in the health education curriculum. All health workers did, however, consider first aid and measures to prevent accidents to be important issues for inclusion in their programs. No respondent referred to particularly vulnerable groups of children. However, when asked, nearly all of them responded with statements such as: “Teach specifically if necessary” and “Teachers will see the needs.” A few respondents mentioned poor children, and one referred to children with epilepsy and different kinds of disabilities to have special needs for health services. Discussion The main reason for using open interviews in this study was the lack of previous research reports from studies of school health services in sub-Saharan Africa. At the same time, available information from national policy papers and WHO documents allowed for a rather structured interview. This structure was seen as a strength as it helped the interviewer focus on the purpose of the study. Furthermore, the use of an interpreter, and the interviewer’s ability to understand most of the answers given in Swahili, made it relatively easy to take notes. When interpreting the results from this study, one should keep in mind the following potential limitations. The respondents were selected from health institutions that had participated in an AIDS program five years earlier (19, 20). As a result, we could have expected a strong focus on AIDS as a local health problem concerning the health care workers. This was not the case. On the contrary, participants mentioned AIDS as a health problem only after probing from the interviewer. Only a few of the respondents had participated in the AIDS project, some had heard about it, and about half did not know about it or did not remember that specific project. Another potential threat to the validity of this study is the fact that the heads of the health institutions chose the participants, and that some of the heads opted to participate themselves. However, findings within and between the 30 health institutions indicate consistency in the information given independent of job title. The results clearly uncovered a gap between the reported practice and theoretical views held by the respondents, indicating that the respondents spoke openly without giving a too positive or too negative picture. Furthermore, the observation of the health institutions and of the nearby schools and school children, along with official epidemiological data, all helped to verify the respondents’ reports. Written Plans for School Health Services and Current Practice The participating health workers’ descriptions of health activities directed toward school children indicates a wide gap between the official guidelines (14) and the current practice. This gap between theory and practice is clearly seen in a number of areas, including: health workers do not visit schools on a regular basis, there is no systematic collaboration between health workers and school teachers, and children with special needs or at particular risk are not systematically followed. The Tanzanian school health policy, as outlined in the National Guidelines (14), is in accordance with the recommendations from WHO. These guidelines specify that the obligations of the health workers include health promotion and primary prevention in addition to curative efforts. The present study shows that the health workers’ activities toward school children are limited to treatment of children who visit the health institutions for help. The main reasons given by the health workers for not visiting the schools or not doing promotional work toward school children were lack of resources or lack of instructions to do so. The poverty and lack of resources at several levels, obvious from the information provided and the observations made, clearly demonstrate a need for more resources. However, it seems that a widespread misconception exists among health workers that MTUHA (17) is the only valid guidance for health work in Tanzania. Thus, there is a need for reinforcing the official guidelines. The reported and observed activities did not indicate any systematic collaboration with institutions outside respondents own health institutions. In spite of the positive attitudes expressed by respondents during the interviews to collaborate with other groups, no respondent spontaneously suggested future collaboration with parents. Cooperation with parents and the community is recommended by WHO (1,2,10,11,12), emphasized by the official Tanzanian guidelines (13,14), and recommended as part of a comprehensive health promotion strategy (5,6). The participating health workers’ collaboration with parents was limited mostly to informing parents about school health programmes and asking for parents’ consent to teach sensitive topics, such as sexuality and family life. The statement of the importance of parents’ consent can be seen as an obstacle to implementing a program, whether this obstacle is rooted in respect of parents’ rights or the health workers’ own ethical norms. Tanzanian school programmes includes HIV/AIDS education as a result of political will; nevertheless, carrying it out depends on the educators. The respondents’ focus on traditional school health services (23) that are independent of district, gender and education, expresses a role of the health worker who is less involved in the planning and implementation of school health services than is recommended by WHO (1,2,3) and the Tanzanian Ministries of health and education (14,16,17). All participating health workers wanted to improve future school health activities and expressed that some improvements could be made within the current setting. However, the lack of resources was clearly seen as an obstacle not only to an ideal school health service but also to health services in general. In response to questions about an optimal school health program, a view emerged which was very much in concert with the description of traditional health education given by Young (24). Despite the fact that most of the participants had been in their positions for several years, only a few of them had attended courses in health promotion. This observation indicates the necessity of a reorientation of the health workers’ view upon their role in school health work. Focus needs to be transferred from the traditional practice of merely curative work to a more promotional policy and practice in accordance with the Ottawa Charter (11). Are School Children Healthy? The participating health workers seemed to share the expanded concept of health, defined by WHO. However, when asked about the health needs of school children, no references were made to the broader concept of health and the specific needs of school-age children. The present results indicate that the majority of health problems among school children are a consequence of poverty and that improvement of equity in health requires long-term planning, not only at an individual level, but also at a societal level.Furthermore, current gender inequalities need to be addressed, as women play a crucial role in caring for their children’s health (25). The view shared by the health workers in this study, that school children are generally healthy individuals, is inconsistent with their own descriptions of the situation and with the official health statistics from Tanzania. Findings regarding school children’s health in the study area indicate a special need for focusing on nutrition, infectious diseases (including HIV/AIDS), and risk behaviors (such as dropping out of school; teenage pregnancy; alcohol, drug and tobacco use). Other prevalent and preventable health problems were injuries, such as traffic accidents, burn injuries and drowning. Given the prevalence of health problems in the research areas, the proposal made by all respondents of physically screening school children appears to be well founded. However, criteria for designing and carrying out screening programs include appropriate management or effective treatments and readily available resources for necessary treatments (26).These criteria are not fulfilled for a number of conditions in major parts of the study area. According to the results of this investigation, children living in urban and some semi-urban areas face the “modern” risk problems of adolescence (e.g., the hazards of alcohol, tobacco and drug use, promiscuous sexual behavior, teenage pregnancy, and homelessness). Taking traditional habits and beliefs into account demands extra effort when planning efforts that target sensitive topics such as sexuality and other gender-related health problems, compared to less sensitive interventions, i.e. infections, accidents, and school meals. WHO clearly recommends that the schools be an entry point for health promotion by establishing preventive programs to reduce the use of tobacco, alcohol, and illicit drugs, and behaviour that promotes the spread of HIV infection (2). WHO also recommends proper awareness of local culture and traditions (1,2,11). The two regions included in this study are culturally complex, and the increased migration of young people from rural to urban areas requires a strong collaborative effort between the health and educational sectors in order to secure that children in all districts acquire critical health and life skills (2). Conclusion A wide gap between the official school health guidelines in Tanzania and the current practice toward school children was observed in this study. The burden of poverty, as clearly stated by the respondents and observed by the investigators, obviously influences the quality of school health services. However, the health workers’ interpretations and experience of the current school health program and working instructions indicate a need for clarification of the official guidelines. Furthermore, health workers clearly need to be offered courses in health promotion linked to school health activities as part of their continuing education. The health workers are professionally educated resource persons, and their role in school health services should be expected and encouraged to be far more active than this study indicates their current practices to be. To successfully establish an integrated school health service, the working relationship between schools, health centres, and the community, including parents and the traditional health sector clearly needs improvement. A number of recommendations based on the findings from this study are outlined in Table 3. Acknowledgement: We would like to thank Mr. B.A. Lyimo for facilitating the fieldwork as well as the health workers who participated in this study. This work was supported by a grant from NUFU. References
Copyright 2008 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp08016t1.jpg] [lp08016t2.jpg] [lp08016t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}