 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 5, No. 2, August, 2008, pp. 94-102 Management And Organization Reforms At The Muhimbili National Hospital: Challenges And Prospects M.A. Mwangu1, N.A.A. Mbembati2, E.P.Y. Muhondwa3 & M.T. Leshabari3 1 Department of Development Studies, School of Public Health and Social
Sciences Received 20th February 2008, Revised 25th May 2008, Accepted 12th June 2008 Code Number: lp08019 Abstract Objective: To establish the state of organization
structures and management situation existing at the Muhimbili National
Hospital (MNH) and Muhimbili University College of Health Sciences (MUCHS)
prior to the start of the MNH reforms and physical infrastructure
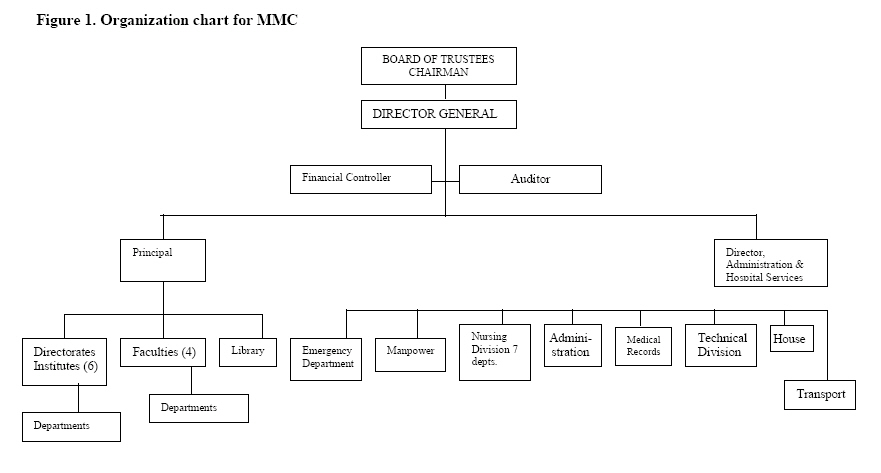
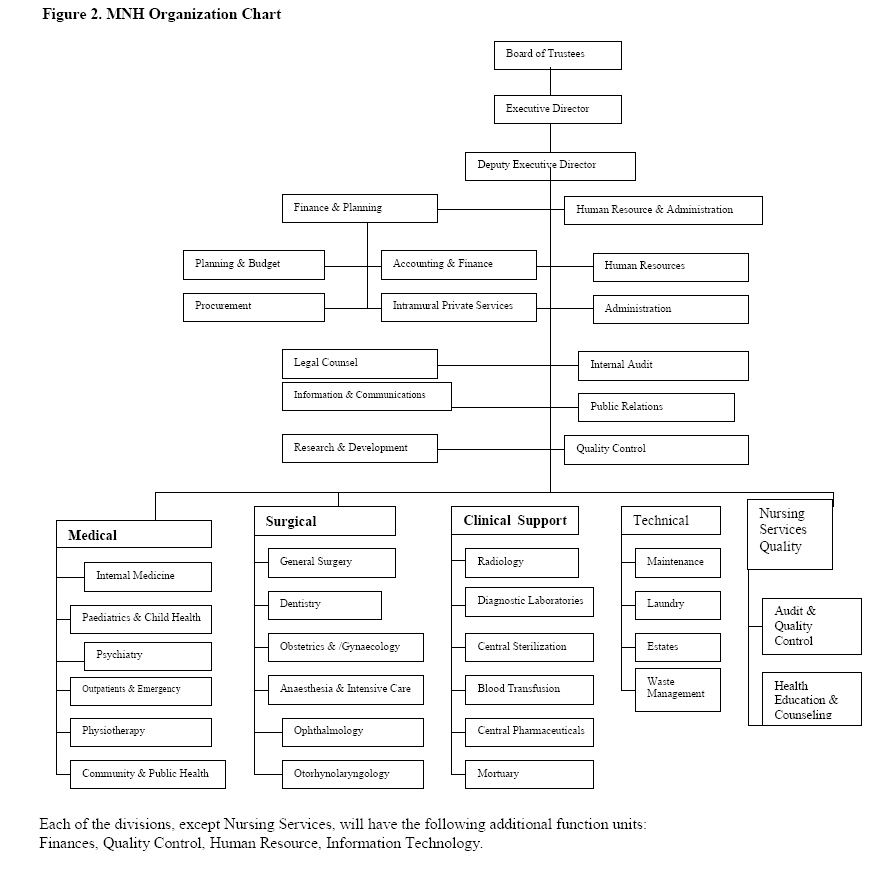
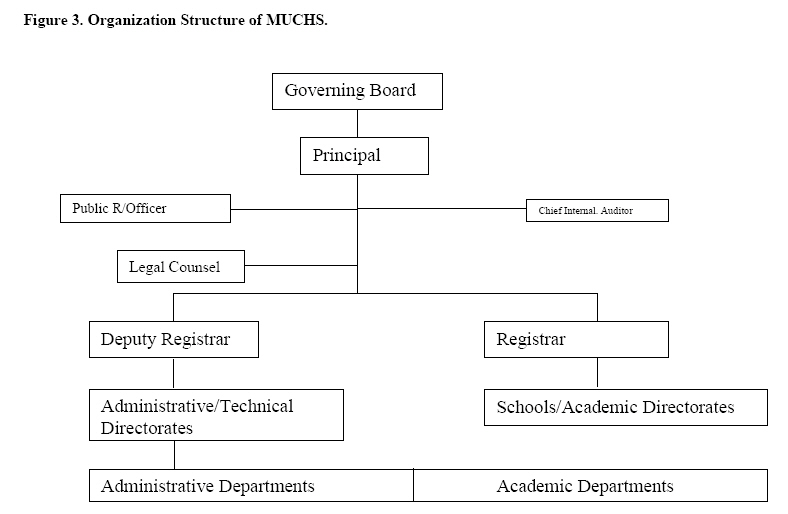
rehabilitations. Key words: Management, Organization structures, Muhimbili National Hospital and Muhimbili University College of health Sciences Introduction: The history of the current MNH located in Dares salaam city, Tanzania, goes way back to 1897 when an Indian businessman established what came to be known as Sewa Haji Hospital (1). Later on when the British came in as new rulers after the Germans, the hospital was renamed Princess Margareth Hospital. It was after a few years after independence in 1961 that the name of the Hospital was changed to Muhimbili Hospital with one of its Ward blocks retaining the name of Sewa Haji in memory of the founder of the hospital. The MUCHS on the other hand started as the Dar es Salaam School of Medicine in 1963 within the premises of the Muhimbili Hospital. Later on in 1966 the school became a Faculty of Medicine of the University College of Dar es Salaam. In 1976 an Act of Parliament created the Muhimbili Medical Centre that incorporated the then Faculty of Medicine of the University of Dar es Salaam. In 1991 the faculty of medicine was upgraded to a College level and a new Act of parliament created the Muhimbili University College of Health Sciences of the University of Dar es Salaam. Thus until the year 2000, the Muhimbili National Hospital and the Muhimbili University College of Health Sciences were one institution under the name of Muhimbili Medical Centre Incorporating the Muhimbili University College of Health Sciences of the University of Dar es Salaam. The detailed structure of the MMC is presented as Figure 1. However in the year 2000, the government dis-established the MMC by repealing the 1976 Act and at the same time amended the 1991 MUCHS Act (2). This move effectively separated the two institutions administratively and in terms of reporting and accountability. While the MNH is now reporting and accountable to the Ministry of Health through its Board of Trustees, the MUCHS reports and is responsible to the Ministry of Science, Technology and Higher Education through its Governing Board. On academic matters the college reports to the University of Dar es Salaam Senate. The main reason for separating the two institutions was to bring about efficiency and effectiveness in the operations of both institutions by clearly defining the roles and mandate of each institution. The changes were also meant to streamline the management of the two institutions by removing dual accountability and confusing lines of communication. For three years between 2001 and 2004 the MNH has been undergoing major reforms aimed at making the hospital a modern entity in the sub region. These reforms are part of a wider scale government led reforms aimed at improving efficiency and increasing autonomy (3,4).The rehabilitations and organizational reforms are aimed at transforming the MNH into a “well run, efficient organization that provides effective, affordable and accessible quality services in support of primary health care, within a caring, patient centred environment that also supports teaching and research, through committed and satisfied staff” (5). The Muhimbili University College of Health Sciences on the other hand was (until January 2007) a college of the University of Dar es salaam specializing in training medical and other health professionals. The college offers undergraduate and postgraduate programmes in medicine, pharmacy, dentistry, nursing and environmental health sciences. The college also offers a variety of advanced and ordinary diploma programmes in allied health sciences such as radiography, laboratory technology, pharmacy, and others. The total student intake is about 1400 undergraduate students and about 80 post graduate students (2003/04 figures) with a total teaching staff of about 200 people ranging from the rank of professors to assistant lecturers (6). The objective of the survey was to collect baseline information before the start of reforms and physical rehabilitations on the current management structure of the MNH and MUCHS and at the same time collect some data on selected indicators that would be monitored on a regular interval as the implementation of the reforms continue. This paper discusses findings of the baseline survey as far as the management situation is concerned. Methods: In-depth semi structured interviews with senior hospital and college management officials were done to gain insights into some of the management issues concerning the two institutions. Issues related to the content of reforms, modes of collaboration between the two institutions, training programmes, human resource profiles and organization structures of the two institutions were also explored. An interview guideline was used for this purpose. Documentation of available hospital and college records was done to elicit data on various management issues such as inpatient services, training programmes, organization structures, human resource profile and other related issues. Registers, reports, official circulars and other written sources of information were consulted to get the required data. A checklist of key information items was used to elicit such information. Ethical clearance for the study was sought and granted by the college ethical clearance committee, while permission to collect data was secured from hospital and college authorities. Data were collected by the principal investigator assisted by three research assistants who were conversant with the clinical and administrative structures of the hospital. The study was done in 2004. Study site The study site essentially constituted of key management offices of the hospital and college. Specifically the offices of the chief executive officers of both the hospital and college, directorates and heads of departments particularly of clinical services were covered during this survey. Data Analysis Because the number of respondents were few and the issues investigated were specific and mostly of descriptive nature, most of the data was descriptively analysed. However for quantitative data simple tables were used to present facts, figures and trends. Structures have been constructed to show organogram of both institutions. To ensure quality control, data from secondary sources was thoroughly counterchecked with the sources to ensure correctness. Data from semi structured interviews was discussed jointly between research assistants and the principal investigator everyday it was collected to ensure its authenticity. Limitations of the study. The first major limitation was the fact that because of the ongoing reforms, there were frequent changes taking place within the hospital to the extent that every time data collected tended to look obsolete. This necessitated constant reviewing of data collected to take into account new developments. The second limitation was the absence of written and well kept data especially with regard to inpatient service records. This necessitated the use of in depth discussions with key informants to get some of the required data. This may have affected the reliability of some of the data collected given problems of recalling past events. Results: Organization structure of the MNH The survey has shown that the MNH was evolving a complex organization structure based on functions of the different divisions of the hospital. At the apex there is the Board of Trustees whose Chairperson is appointed by the President of the United Republic of Tanzania upon recommendation by the Ministry of Health. The board is constituted of members drawn from the Dar es Salaam City Council, MUCHS, representatives of Workers Union, Attorney Generals Chamber, appointees of the Minister of Health, the Executive Director (who is the secretary to the Board) and representatives from the MNH management. The Board is the supreme organ vested with a wide range of powers and functions as stipulated in the Act Establishing the MNH (7). Among others the Board appoints senior members of the hospital management team and ensures the overall smooth running of the hospital. The tenure of office of the Board is three years and members of the board are eligible for re appointment Below the Board of Trustees there is the Executive Director who is the Chief Executive Officer (CEO) of the hospital. He/she is appointed by the ministry of health but accountable to the Board of Trustees. The CEO is responsible for the general conduct of the day to day operations, management of the hospital under the direction of the Board of Trustees. Under the Executive Director there are five divisions namely Surgical Services; Medical Services; Clinical support Services; Technical Services and Nursing Services Quality Division. Each of these divisions has a number staff working under the head of the division. The detailed structure is presented as Figure 2. Organization Structure of MUCHS (The structure has changed since 2007) Following separation of the college from the hospital the former had to develop its own organization structure as well. The organization structure of the college is equally complex but follows a common template of organization structures of institutions of higher learning in Tanzania. The top most organ of the college is the Governing Board whose chairperson shall be the Vice Chancellor of the University of Dar es Salaam. The Board shall be constituted of nine members namely the principal of the college who shall be the secretary to the Board, the MNH Executive Director; Director of Higher Education in the Ministry Science, Technology and Higher Education; Director of Human Resources in the Ministry of Health; an appointee of the minister for higher Education; the Treasury Registrar and a representative of the Attorney Generals Chambers. The Board is the principal policy making organ of the college responsible for ensuring the college fulfils its mandate efficiently and effectively. The principal of the College is the CEO, appointed by the President of the United Republic of Tanzania upon recommendation by the Vice Chancellor of the University of Dar es Salaam and the Minister for Science Technology and Higher Education. The principal is answerable to the Governing Board and is responsible for the day-to-day running of the college activities. Below the principal there are two principal officers: one responsible for academics and the other responsible for administration and finance. The two officers were known as the Registrar and the Deputy Registrar respectively. Under the Registrar, there are a number of schools and directorates dealing with training research and consultancy activities. These include the Schools of Medicine; Pharmacy; Dentistry; Nursing, Public Health and Social sciences; and Directorates of Research and Publications; Post- Graduate Studies, and Library Services. Schools and directorates have a number of departments or sections under them. On the other hand under the Deputy Registrar there are the departments of finance and administration, estates, and student welfare. The detailed structure is presented as Figure 3. Human Resources Situation in selected clinical departments During the survey it was noted that there was no central and up to-date inventory of all workers in the hospital. An attempt was made to establish the number of specialist health professionals (trained to master’s degree level or above) who are working in clinical areas that cut across both the Hospital and the College. The departments targeted were medical, surgical, obstetrics and gynaecology, paediatrics and psychiatry. Through discussions with the respective heads of these departments and other senior staff in the respective departments, a human resource profile for each of these departments was estimated. It was established that in most departments there was shortage of specialists required to deliver clinical services and teaching of students. Department of Internal Medicine. The department of internal medicine had eleven 11 specialists, 9 of whom have academic status and the remaining 2 are non- academic members. Of interest to note is the fact that the department has no single specialists in the areas of gastroenterology, rheumatology, clinical haematologist, geriatrician (elderly medicine) and infectious disease specialist. The required full strength of specialists is estimated at 34 leaving a deficit of 23 specialists. Department of Surgery Like Medicine, Surgery also cuts across teaching and hospital based clinical services. The survey has shown that currently the department has 21 surgical specialists out of whom 12 are academicians and 9 are non- academicians. The required number is 35 thus the department is operating with a shortage of 14 surgical specialists. The most critical need is in the cadres of orthopaedic trauma, cardiothoracic surgery and plastic/reconstructive surgery where the department has either none of these specialists or just one in each discipline. Obstetrics and Gynaecology Department. The Department of Obstetrics and Gynaecology has a total of 23 specialists out of whom only 8 are academicians and the remaining 15 are non- academics. Out of the 23 available the majority (about 20) are obstetricians/gynaecologists while there is only one gynaecologist/oncologist and two gynaecologist/VVF repair specialist. For the department to smoothly discharge its clinical and teaching functions, it requires a total number of 33 specialists. The department faces a shortage of 10 specialists, the most critical ones being oncologists and VVF repair specialists. Paediatrics and Child Health Department Paediatrics and Child Health Department was also surveyed to establish its human resource profile. The department was found to have a total of 13 specialist staff out of whom 6 are academicians and 7 are non-academicians. The required staff strength is 25, thus the department faces a shortage of 12 staff the most critical cadres being gastroenterologist, cardiologist, and neo-natalogist. Apart from staff matters, it was also observed that the department runs a Multi Purpose Paediatrics Laboratory complex. The complex is run as a semi autonomous entity with its own management structure. The Steering Committee oversees the overall functioning of the laboratory. The manager, assisted by an administrative officer, an accountant, and a team of laboratory technicians, does the day- to- day management of the complex. All these are under the doctor in charge. Through discussions with the head of department it was shown that generally this laboratory is an example of a successful cost centre in the sense that it is a self-sustaining business. The laboratory is capable of generating sufficient income to cover for its running costs including purchase of laboratory equipment and reagents. In overall terms the hospital and College faces a deficit of 62 key specialists as shown in Table 1 below. This represents a 45.2% human resource shortfall. Psychiatry Department The department of psychiatry has a total of 7 specialists against the requirement of 10. All the seven members are academicians. However out of the 7 available staff, 2 were on long term study leave and one was a retired officer working on contract. The department had a critical shortage of a child/adolescent psychiatrist and a forensic psychiatrist Selected Inpatient Performance Indicators. During the study an attempt was made to review two key performance indicators in the inpatient services namely bed occupancy rate and average length of stay for the inpatients. These indicators are widely used to measure efficiency and effectiveness of hospital services in as far as inpatient services are concerned. Bed Occupancy rate Average bed occupancy rate is one of the measures of utilization of hospital services in this case inpatient services. The rate is usually calculated by taking the total number of in-patients days in a week/month/year, divide by total number of bed days in a week/month/year times hundred. Normally data for calculating bed occupancy ratio (daily bed state) is supposed to be kept in the inpatient records. Calculation of occupancy rate can be done monthly or even weekly depending on the needs, but certainly at the end of the year an annual bed occupancy rate should be calculated. The higher the occupancy rate the greater the degree of utilization of hospital bed capacity. Conversely the lower the rate, the lower the utilization of bed capacity. While experts often differ on the optimal rate of utilization, it is often argued that an occupancy rate of more than 80% is likely to cause constraints to the services and hence cause inefficiency.)On the hand a rate lower than fifty percent is deemed to be under- utilization of bed capacity. However these standards could possibly be more applicable in developed economies with advanced and more adequate hospital services and not so much in less developed economies where the demand for hospital inpatient services often grossly exceeds available capacity. As far as the MNH is concerned, attempts to establish the bed occupancy ratio faced difficulties. There were no readily calculated figures for the hospital so it was necessary to go to primary data on daily bed states in order to establish the number of patients- days in a month and eventually in one year. Data was counted and calculated from each individual wards before being summed up at departmental level. It was very difficult to get complete data as some of it was missing and could not be located. We used data for the year 2002 since it was comparatively more complete. The calculations done indicate that the bed occupancy rate ranged from 42% in paediatrics wards to 121% in maternity wards. The overall (average) hospital bed occupancy rate was 90.4% as indicated in Table 2 . Table1. Summary of selected specialist human resource profile
aInclude one retired officer. Table 2: Bed Occupancy Rate for the Year 2002.
aBed Occupancy Rates were calculated by taking total number of patient days in a year divided by the number of bed days in a year times a hundred. Table 3. Average Days of Stay (2003 estimates)
Average Days of Stay. Average days of stay for inpatients are one of the indicators of the efficiency and effectiveness of services provided. This indicator is calculated by dividing the total number of days stayed by inpatients by the number of admissions. Taking other factors to be equal, the lesser the patient stays in a ward, the more efficient and effective the services are deemed to be. This indicator requires that record of patients admission and discharge/death dates are properly recorded and kept, and later on summed up to get average days of stay. There were no readily calculated data for this indicator. To make matters worse it was virtually impossible to track records of admissions and discharges/deaths because of poorly kept records. This situation posed a major obstacle. For purposes of getting a rough picture of this indicator, it was decided to use in-depth discussions with senior nursing staff in the respective wards. In each ward a group of between 3 and four senior nursing staff were engaged in a discussion aimed at estimating the number of days a patient stays while hospitalized. The estimated figures are for the year 2002. As shown in table 3 the average days of stay differ significantly from one ward to another. The lowest number of days was estimated for the medical wards (6 days) and highest for the surgical wards (11.4 days) Collaboration Between MNH and MUCHS (now MUHAS) As mentioned earlier, prior to the separation of the hospital from the college in the year 2000, the MNH and the Muhimbili University College of Health Sciences were operating as one institution with a rather complex organization structure and reporting relationship. Notwithstanding the complexity of the reporting relationship, under this structure, cooperation between the two institutions was taken for granted since the two were in reality operating as one institution. However with the legal separation of the two institutions in the year 2000, they became separate entities with different leaderships reporting to different authorities. Under these circumstances, the need to work out new modalities of cooperating became necessary. The need for the two institutions to continue to work together cannot be over-emphasized as the two are closely inter dependent. The College on the one hand cannot effectively carry out its functions particularly the training one without the hospital. Students and staff need the hospital for clinical training. The hospital on the other hand relies of the College to supply highly trained personnel in the different medical and related disciplines for specialized referral services. Logically therefore the two institutions need to collaborate for their mutual benefit and for the benefit of the general public The main areas of collaboration include: students clinical training, collaborative research, services provision and continuing education for staff. In all these areas close coordination is required from both sides. It was reported that during the initial stages of the reforms the relations between the two institutions were found to be a little bit un-cordial due mainly to the uncoordinated decisions and changes that were taking place in both sides without prior information to the other party. For example it was reported that the decision to rehabilitate the inpatient wards and reduce their bed capacity by almost half is something that had a negative impact on the college side in terms of reduced number of patients for training purposes. Yet the issue was never discussed and agreed upon by both parties before implementation. Modality of cooperation between the two institutions: Any fruitful cooperation between two or more parties with mutual interests requires at least two conditions: First is good will from both or all parties, and secondly it requires a legal and mutually agreed upon mechanism to regulate the modalities of cooperation to be in place. As the survey was being undertaken, the two institutions had completed working on a Memorandum of Understanding (MoU) that would govern their relationship as public institutions (8). The MOU defines clearly the way the two institutions relate with each other and defines the roles, responsibility, and obligations of each institution. The document also explains the modalities of settling disputes between the two parties in the event such disputes occur. Additionally the two institutions have agreed to formulate a “Supplementary Service Contract” (9) for clinical staff who would be working in both institutions. The contracts define the duties, roles and obligations of clinical staff who are working on both sides that is the hospital and the college. Each clinical staff will be required to sign this contract with the hospital under the terms that have been mutually agreed upon by the hospital and college managements after a long consultative process. These are important moves aimed at laying the foundation and consolidating the already close working relationship between the two institutions. The challenge that now lies ahead is for both institutions and individuals to implement what has been agreed upon in the two documents. Discussion Organization structures From the findings it has been established that after separation, both the MNH and MUCHS have developed their own organization structures that are fairly complex reflecting their mandates as stipulated in the Acts establishing the two institutions. The structures put in place are founded on the traditional organizing theories in which departmentalization forms the core basis for functional structures to be created (10). In both the MNH and MUCHS the groupings are based more or less on the similarity of tasks performed. For the MNH the new structure created is a major departure from the old pre separation structure as a lot of new units and reporting relationship have been put in place. The spirit of decentralization embedded in the new structure is potentially advantageous in terms of expediting decision- making and increasing efficiency and effectiveness in service delivery. The major challenge facing the hospital now is to strengthen the capacity of the departments so as to handle the added responsibilities. The offices of the heads of department need to be provided with an adequate number of administrative support staff such as administrative officers cum accountants. Further re organization of the clinical departments may be needed to cope up with the relative increase in the number of employees under their supervision. For instance the positions of Heads of firms may need to be re-defined and strengthened so as to provide effective assistance and support to the heads of departments. Human Resource Situation. The study has shown that generally the MNH is understaffed especially when we consider specialist cadre who are the most needed for specialized care as well as for teaching and research. As shown in the findings virtually all clinical disciplines face shortage of specialists. Internal Medicine had a deficit of 23 specialists, surgery 14, obstetrics and gynaecology 12; paediatrics and child health also 12 and psychiatry had a deficit of 3 specialists. In total the hospital faced a deficit of 62 specialists needed by both the hospital and the college. This is a significant shortage of staff with far reaching implications for specialized patient care, training and research. Although not documented in this paper, heads of departments clearly indicated that the shortage of staff was cutting across other cadres as well such as Registrars, and technicians. The main reason attributed to shortage of specialists health professionals was their scarcity in the local market because of low output of such graduates coupled with brain drain to other countries. This deficiency in skilled personnel is likely to affect the quality of services given both at the hospital and college sides. It should be underscored that the MNH as a referral hospital and MUCHS as a College of health sciences are required to have an adequate number of highly trained specialists in the different disciplines in order for the two institutions to fulfil their respective obligations. It should be further observed that with the on going reforms that involve decentralization of powers to the departments, there is need for all departments to be supported by strong teams of administrators cum accountants to assist the heads of departments to perform their expanded range of duties. The responsibilities of planning, budgeting, and personnel management that now weigh heavily on the shoulders of heads of department certainly need a strong administrative support backing. Inpatient Indicators. Bed Occupancy Rate and average length of Stay. As noted from the findings, the hospital bed occupancy rate is estimated at 90.4%. The highest recorded rate is in obstetrics and gynaecology with 121%. This implies the maternity services are grossly over used to the extent of having floor cases! The overall rate of 90.4% generally compares with experiences in many poor countries in Africa. However a study made in the Suez General Hospital indicated a slightly different picture of bed occupancy rate of between 12% for the ophthalmology department to 90% in the ENT department (11). Similarly for the average length of stay the study showed a range of between 4 days to 18 days for the different disease conditions. This roughly compares with the situation at the MNH. What do these indicators mean in terms of quality of inpatient services? The average length of stay is an important indicator of efficiency of hospital resource utilization. Differences in the average length of stay among comparable types of departments may imply differences in prevailing treatment practices across the hospital. However without more information about case mix and severity, it is difficult to use length of stay as a direct indicator of efficiency. Nevertheless stays in the wards that are unusually long raise many questions regarding efficiency and hence the need to have a closer look at the possible causes. A higher bed occupancy rate on the other hand does not necessarily indicate better hospital performance. When bed occupancy rates are too high it means the volume of services is beyond the designed level of the hospital. Two scenarios can be used to explain this situation. On the one hand high occupancy rate may reflect a relatively efficient situation in which patients with modest lengths of stay are served (high bed turn over rate). On the other hand high occupancy rate may result from deficient situations having a long length of stay (low bed turn over rate). As far as the MNH is concerned, the latter scenario is most likely applicable given the generally low level of services provided. However for these indicators to be accurately calculated, the hospital has to collect and properly keep the primary data. Conclusions. In summary this survey has shown the following salient features of the management situation prevailing at the MNH and MUCHS: Following the separation of the two institutions, both have put in place new organization structures that are fairly complex but reflect their respective roles and responsibilities as defined in the Acts of law establishing these institutions. The structures appear good enough and time is needed to prove their effectiveness. The study has observed that some of the vital inpatient performance indicators/data particularly average days of stay and bed occupancy rates are not readily available. Part of the problem is that the hospital does not have a system of calculating these indicators for use by the hospital decision makers. This calls for deliberate efforts by the hospital to ensure essential performance indicators are periodically calculated and properly kept for use. The human resource situation is a critical area of deficiency that really needs to be addressed as soon as possible since without the requisite trained personnel it may not be easy for both institutions to realize their goals. The two institutions are now in the right track of formalizing their close working relationships. The newly created instruments to regulate the cooperation (MoU and Supplementary Service Contract) are important steps in the right direction. Recommendations It is recommended that both the hospital and the college should make more concerted efforts to ensure the two institutions are properly staffed with adequate number of qualified staff in the different job positions as per staff establishment and needs. Since MUCHS is the main source of high- level human resources in the health sector, it is recommended that the college should take measures aimed at increasing enrolment of post graduate training in the different medical specialities to meet the growing demand for such cadre of workers both for the MNH and the college itself. The hospital should endeavour to collect, keep properly and periodically analyse basic data related to inpatient as well as other services within the hospital. Information such as occupancy rate and average length of stay for inpatients are vital indicators such that the hospital should routinely calculate them for management use. Finally it is recommended that the two institutions should continuously strive to work together closely in order to ensure both meet their objectives and at the same time serve the larger public. It should be underscored that given scarce human resources, sharing of these resources between the hospital and the college is perhaps the best option that also works for national interests. Acknowledgement. The authors wish to sincerely thank the Abbot Fund and Axios Foundation for funding the baseline Survey upon which this paper is based on. Sincere appreciation is also extended to all staff of MNH and Muhimbili University College of Health Sciences (MUCHS) who in one way or the other participated in the generation of information leading to the production of this paper. References:
Copyright 2008 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp08019f2.jpg] [lp08019f3.jpg] [lp08019f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}