 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 5, No. 2, August, 2008, pp. 103-110 The Effectiveness Of The TBA Programme In Reducing Maternal Mortality And Morbidity In Malawi Thomas Bisika Correspondence to: Thomas Bisika, School of Health Systems and Public Health University of Pretoria, South Africa. Email: tbisika@yahoo.com Received 26th November 2007, Revised 25th May 2008, Accepted 4th June 2008 Code Number: lp08020 Abstract Objective: The main
objective of this study was to assess the role of TBAs and the quality of their
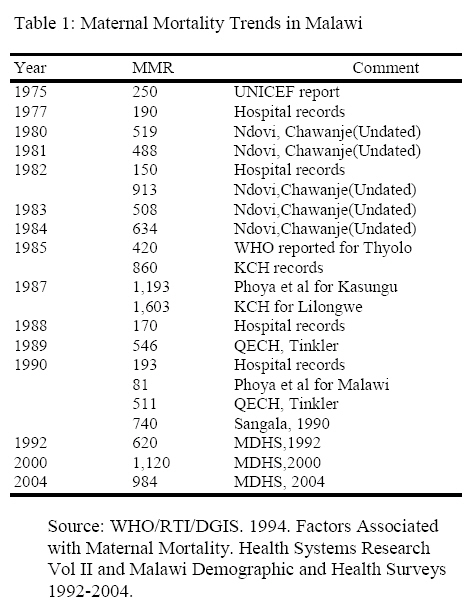
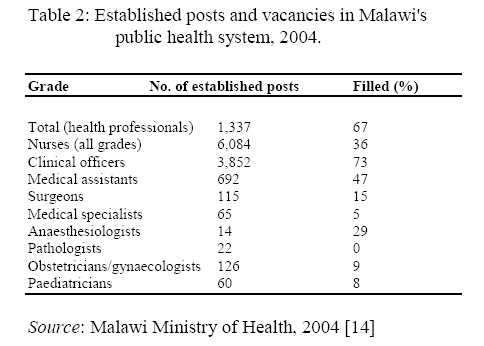
services in contributing to the reduction of maternal deaths in Malawi. Introduction The World Health Organization (WHO) reports that reproductive health problems account for more than one third of the total burden of disease in women. WHO further estimates that over 500,000 women die every year from complications of pregnancy, including abortion and virtually all these deaths occur in developing countries, which accounts for 99% of all these deaths (1). According to the Tenth International Classification of Diseases maternal death is defined as the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of duration and the site of pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes. For practical reasons this definition has been simplified as the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the cause of death. There are several indicators of the level of maternal mortality of which the most common ones are: Life time risk: This measure reflects the probability of maternal death faced by a woman over her entire reproductive life-span. Maternal Mortality Rate: This is defined as the number of women who die as a result of childbearing (maternal deaths) per 100,000 women aged 15-49 in a given year. Maternal mortality ratio (MMR) This is the number of women who die as a result of childbearing in a given year per 100,000 live births in that year. Maternal Mortality ratio defined in this way indeed looks more of ratio than a rate however Maternal Mortality Ratio (MMR) is also used to mean Maternal Mortality Rate which is the single most important indicator of maternal mortality. (2) Level and Trends in Maternal Mortality Globally and in Malawi World wide at least 1,600 women die each day from the complications of pregnancy and childbirth. Maternal mortality rates in developing countries average in the range of 450 to 2000 per 100,000 live births as compared to about 30 per 100,000 live births in developed countries (3). The maternal mortality rate for in Malawi is very high by any standard. According the Malawi Demographic and Health Survey (MDHS), the maternal mortality rate for Malawi almost doubled between 1992 (620 per 100,000 live births) and 2000 (1,120 per 100,000 live birth) and only declined slightly to 984 in 2004 (4). The life time risk of maternal death in Malawi in 1 in 17 which does not compare favorably with the world average of 1 in 74 and the 1 in 4,085 in industrialized countries (5). A study conducted in 1989 at Queen Elizabeth Central Hospital in Southern Malawi showed that there were 78 maternal deaths giving an MMR of 546 while another study in 1990 revealed that there were 73 maternal deaths resulting in an MMR of 511. This study also observed that there was an increase in puerperal sepsis in 1990 among maternal deaths (6).Earlier reports estimated MMR to be 250 per 100,000 in 1975 (7). Later aggregated hospital records showed MMRs of 190, 150 and 170 per 100,000 live births for the years 1977, 1982 and 1988 respectively. Hospital records for Kasungu further yielded an MMR of 1,193 (210 maternal deaths out of 17,604 deliveries) and Lilongwe Central Hospital gave an MMR of 1,604 per 100,000 live births in 1987 (i.e. 260 maternal deaths out of 16,217 deliveries ) (8). Phoya et al (9), observed an MMR of 193 per 100,000 live births in hospitals and 81 per 100,000 live births for Malawi. Although this study was hospital based, it was learnt that of 102 cases who died post-natally, 76 delivered in hospital, 4 at a TBA and 22 delivered at home. Table 1 below summarizes the trends in maternal mortality in Malawi since 1975 from various sources. Causes of Maternal Deaths The major causes of maternal mortality in developing countries include anaemia, haemorrhage, eclempsia, infections, abortions and complications of obstructed labor (1). A multi-country study on maternal mortality established that the most common cause of maternal mortality for Malawi and Songea district in Tanzania was bleeding / haemorrhage (39% -Malawi and 49%-Songea, Tanzania) and infection / puerperal sepsis ( 25%-Malawi, 33% Tanzania ). These are all preventable causes. In Malawi, the age group 16-20 accounted for 33% of the deaths followed by the 26-30 (25%), 31-35 (19%), 21-25 (16%) and those 36 years and over accounted for 8% (10). According to Phoya et al (9) most of the women who died in Malawi were married and more than half (58%) of women who died after delivering in hospitals were assisted by either a doctors or a clinical officer while 34% were attended to by a nurse/midwife. A multi-country case control study of risk factors associated with maternal mortality in Lesotho, Malawi, Uganda, and Zambia, concluded that about 30% of deaths were associated with abortion. Other factors associated with maternal mortality included lack of education or low education levels, single marital status, young age (less than 17 years) and older ages (more than or equal to 35 years) (10). The analysis of maternal deaths occurring at Kamuzu Central Hospital and Bottom hospital in Malawi indicated that 21 deaths were parity 1, 28 were parity 2-5 and 17 were parity 6-10 out of the 74 maternal deaths. Only 23 deaths (38%) were documented as having received some antenatal care (11). According to another study conducted at Kamuzu Central Hospital, a large proportion of maternal deaths were due to avoidable causes which included inadequate case management, non-availability of essential drugs, poor transport facilities for referral, unnecessary delays at peripheral health facilities and absence of qualified staff (12). A high prevalence of HIV/AIDS has also affected pregnancy outcomes. The Malawi Red Cross Society reports that “more than 90% of blood donors tests negative for the HIV test.” Which means that one in ten of the Malawi population could be carrying the deadly virus that causes AIDS. Similary the National AIDS Commission reported a national HIV prevalence of 14.4% in the year 2004 (13). Delivery of Maternal Services The Malawi government through the Ministry of Health is the main provider of maternal health services in Malawi. The services are provided by doctors, clinical officers, registered nurse-midwife and enrolled nurse-midwife in a hospital setting. Table 2 below shows that the skilled attendants in the hospitals are in short supply. The Table above shows that 64 % of established nurses posts and other involving health personnel in Malawi have not been filled due to serious staffing problems. Mid-wives provide the bulk of maternal health services in both government and private health facilities. Maternal services in government facilities includes ante-natal care, delivery services, post-natal care, family planning and other related reproductive health services. The other main provider of maternal health services in Christian Health Association of Malawi followed by private hospitals. The Traditional Birth Attendants (TBA) Recognizing the acute shortage of staff in the midwifery profession the Malawi government introduced the TBA training program. These TBAs, whether trained or untrained play an important role in the provision of delivery and other maternal and child health (MCH) services. There are now over 5,000 TBAs in Malawi out of which the Ministry of Health has managed to train just over 2000. Only the trained TBAs are given a delivery kit. TBAs are encouraged to refer all “at risk cases” to the hospital although logistical issues may make this difficult (15). Study Objective The main objective of this study was to assess the role of TBAs in contributing to the reduction of maternal deaths in Malawi as well as the nature and quality of their services. The study was also supposed to establish the utilization levels of the TBAs and assess their knowledge of danger signs of obstetric complications. Methodology The study technique that was used to adequately address the objective of this study was highly participatory with in built capacity building for the Reproductive Health Unit (RHU) of the Ministry of Health and Population. A qualitative research methodology was preferred mainly to uncover the unforeseen concerns of the target population. Several data collection instruments were used to ensure that the methods were “triangulated” so as to allow for comparison of findings. This was based on the understanding that when different methods applied to different categories of respondents yield similar results, the findings can be accepted with much confidence. Information was collected using focus group discussions (FGDs) which were conducted with women of reproductive age and some who have had at least one child. These FDGs were conducted by female graduates and undergraduates from Chancellor College, a constituent college of the University of Malawi. The research assistants were trained fully by a social scientist on methodological issues and the TBA Co-ordinators with the help of a Registered Nurse Midwife consultant on issues related to maternal and child health. Supervision of these Research Assistants was done by two TBA Co-ordinators identified by the RHU who were supervised by a social scientist conversant with public health issues including reproductive health. A consulting registered nurse/midwife who trained the research assistants was also part of the field team. As a requirement 6-10 women participated in each FGD and all FGDs were facilitated by two ladies one acting as a moderator while the other was a note taker. Once the FGD had been completed a full report was produced the same day to avoid recall bias. The interviews were not recorded because of the sensitivities associated with utilization of TBAs especially those who also double as traditional healers. In addition to the FGDs, in-depth interviews with community leaders who included chiefs, religious and political leaders as well as Village Health Committee Officials were conducted. In-depth interviews were also conducted with TBAs and an inspection of their environment and delivery kit was also done using inspection check list developed by the TBA Program. Finally, Key informant interviews were held with District Health Officers, Reproductive Health, MCH and TBA Co-ordinators and the matron at district level while at the hospital and health center level interviews were conducted with nurse or midwife in-charge of the maternity ward. A total of 11 districts were visited from all the three regions as follows Karonga and Mzimba (Northern Region), Lilongwe, Salima and Ntcheu ( Central Region) and Zomba, Blantyre, Machinga, Nsanje, Thyolo and Mulanje in the southern Region. In each district, 3 communities were selected. Two of these were from the rural areas while one was from the Urban. In each community at least 2 TBAs were interviewed. In additions, 4 community leaders were interviewed and 2 focus group discussions were also conducted in every community. Where there was a health center, the nurse was interviewed as a key informant. The final approach involved a detailed literature review on studies conducted to assess the effectiveness of TBAs in Malawi and other countries. Data Analysis A lot of information was collected which was qualitative in nature. With the help of text –base beta a primitive tree was constructed with the specific study objectives as nodes. Secondary nodes originated from the primary nodes. Information associated with each node was then attached to the specific node which was then managed manually. The fair notes from the field provided the information used in the actual “content analysis” while the tape recordings provided a backup. Ethical Considerations All the interviews were conducted in strict privacy where the respondents were neither heard nor seen by other people. The recruitment of respondents was on the basis of voluntary participation although this was tricky considering that the Malawi government commissioned the actual study a fact which was explained to the respondent as a requirement for obtaining an informed consent. All information collected during the study was kept confidential and sensitive quotations were not attributed directly to a particular respondent to protect their identity. The nature of the study was explained to the respondents before obtaining a verbal informed consent and no inducements of any form were used to coerce the respondents. The study protocol itself was submitted to the institutional review process and was approved by the management of the Centre for Social Research and the University of Malawi Research Coordinators office. Results The Effectivenes of TBAs From the literature review it was clear that there are still many developing countries where a large proportion of the population does not have access to maternal health services, relying on TBAs to meet their health care needs and Malawi is not an exception. A majority of births in such countries, particularly in the remote rural areas, take place at home or in the community usually assisted by relatives / friends or TBAs. In these countries, TBAs who have been trained can contribute to improving MCH as they offer the only means by which women in rural communities have access to a clean delivery. An evaluation of UNFPA support to TBAs conducted in 1996 noted that the effectiveness of TBAs can be increased if their programmes were part of the broader national strategy to improve reproductive health. Such programmes should include adequate supervision, transportation and provision of supplies. In particular the report recommended that TBA programmes should increase efforts to ensure the availability of supplies to conduct a clean delivery since this is essential for TBAs to follow aseptic procedures. In this regard, the report observed that locally produced TBA kits could be more practical and sustainable. The evaluation concluded that effective referral system is critical for TBA success no matter how well the TBAs are trained (16). In Indonesia TBAs were reportedly effective at distributing and monitoring of the intake of iron / folate tablets (17). However, a study conducted by UNICEF in Somalia observed that “despite a high standard of TBA training, when dealing with complications such as prolonged labor, haemorrhage or infections, families still preferred traditional practices. Families were unlikely to value the opinion of the TBA in making the decisions to refer a woman for emergency obstetric care.” The study also observed that TBA programmes that exist in isolation of other interventions are unlikely to have any significant effect on maternal mortality although clean deliveries and ante-natal care practiced by trained TBAs may reduce maternal morbidity and peri-natal mortality and morbidity (18, 19). Commenting on the effectiveness of TBAs, Asghar (20) in one of his studies conducted in developing countries involving obstetric complications and the role of TBAs argued that TBAs can be effective if they are trained and respected by their medical colleagues and he further reports that the availability of transport and accessibility of specialized medical care is an important factor in TBA effectiveness. In Bangladesh, Musha (21) reports that trained TBAs could serve a critical role in linking pregnant women and their newborns with the formal health care services. However, he acknowledges that recent debate has been fierce, and studies inconclusive, as to whether TBAs have the skills and competencies to actually impact maternal and peri-natal mortality. He further observed that trained TBAs as compared to untrained ones, are more likely to be knowledgeable about antenatal, intrapartum, and postpartum danger signs. They are also more persuasive in referring mothers for antenatal and even more active in visiting mothers and newborns and checking for complications. Finally the Bangladesh study concluded that Trained TBAs apply more hygienic delivery practices than their untrained counter-parts. Elsewhere, Patterson (22) reports that in their TBA project their approach was to give TBAs a special role. They wanted TBAs to encourage other women to access the formal health sector and to learn better maternal care. As a result of this orientation more pregnant women were reportedly seeking information on pre-natal care. In this case TBAs seem to have been very effective. Various studies have also demonstrated that by training TBAs in timely recognition and referral of pregnancy, delivery and neonatal complications, the health situation of the pregnant women and their newborns can be improved (23-28). In Nigeria, Imogie (29) records that “some women resort to TBAs because they have no other alternative while others believe in the effectiveness of TBAs.” However, Imogie cautions that “poor hygienic measures and late referrals of complicated cases on the part of TBAs have been indicated as major causes of maternal health problems.” The apparent success of TBAs enumerated above should be weighed against the background that The World Health Organization, in its World Health Day 1998 statement on safe motherhood (30) cautions that many women and newborns develop complications during or immediately after delivery which are difficult to predict, and which require a skilled attendant to manage appropriately. Skilled birth attendants are defined by WHO as trained midwives, nurses, nurse / midwives or doctors who have completed a set course of study and are registered or legally licensed to practice. This definition implies that TBAs are not skilled attendants. According to WHO skilled attendants are very important because “every pregnancy faces risk.” (31) Malawi Experience Role of TBAs According to the community leaders and members of their respective communities, the majority of pregnant women in the 11 districts that were visited seek maternal care from the health center or hospital. A significant proportion, however, especially in remote rural areas, were reportedly seeking help from TBAs. Some respondents reported that there are some pregnant women, who opt to deliver at home where they are assisted by relatives and friends. The community members and their leaders reported that the role of TBAs was to assist pregnant women during delivery. The roles that were mentioned by the TBAs themselves and the key informants who were mostly health center staff or staff based at the DHO’s office were much broader and included delivery service for women who are due, distribution of iron tablets, referral of pregnant women for anti-natal care (ANC), health education, screening of pregnant women for danger signs including advising women on neonatal care, taking care of pregnant women, ANC, giving advise to pregnant women, cooperating with the community, offering advice on nutrition and hygiene and stocking supplies like iron tablets and anti-malarial tablets for pregnant women as well as encouraging pregnant women to go for immunization at the hospital. With respect to neonates (infants up to 28 days of age), the TBAs are supposed to ensure that the child is well and they also have to monitor them closely. Cord Care (“kusamalira Pamchombo”) should be emphasized by TBAs. They should tell mothers not to apply herbs to the healing navel. TBAs should also make sure that the baby is sucking properly (“akuyamwa bwino”) and should emphasized the importance of exclusive breast – feeding. On HIV/AIDS, TBAs reported that they are supposed to advise pregnant women to bring their own razor blade and encourage women to go for HIV/AIDS test (VCT). With respect to record keeping, the TBA co-ordinators noted that TBAs are supposed to keep referral forms, a special register and danger signs cards. Quality of their services On the quality of their services there was a general feeling among TBA co-ordinators and other health personnel that it was still poor. This was mainly due to high levels of illiteracy, old age, and lack of supervision. According to the TBAs themselves, lack of equipment, supplies and logistical problems when dealing with referrals also affect the quality of TBA services. An inspection of their equipment and working environment revealed that TBAs are working under difficult circumstances. Poorly ventilated rooms, inadequate lighting, dilapidated and non-existent equipment and general lack of essential commodities for ensuring a clean delivery characterize their practice. Community perception on how TBAs can reduce delays TBAs have been identified by community members as important providers of care to pregnant women. As people who are trusted and held in high esteem by community members and leaders alike, TBAs have an important role to play in encouraging pregnant women to seek appropriate care on time in order to reduce the incidence of pregnancy adverse outcomes. According to community leaders and TBA co-ordinators, TBA could help reduce delays in care seeking by advising pregnant women to attend ANC and educating them on the importance of prompt care- seeking. TBAs co-ordinators insisted that TBAs should not work in isolation. They should work with the communities they save and attend meetings where they may also have a chance to talk to community leaders on issues that promote or constrain timely and appropriate care-seeking. They emphasized that TBAs should act as a link between the health center/hospitals and the community and that Health education should target the pregnant women as well as the community at large. The communities were of the opinion that TBAs can play a big role in encouraging women to seek appropriate care promptly. Community member observed that TBAs need to do a very good job in order to attract women who deliver at home. They also need to make their service more accessible by reducing the fees they charge. They also need to organize antenatal care services where prompt care seeking should be emphasized. The communities were also of the view that if TBAs cautioned women who come late this would have ensured that next time pregnant women would seek care promptly. The further observed that TBAs should also target men and the entire communities in their education programs on danger signs and the need for prompt care seeking. The District Hospital personnel emphasized that once a pregnant woman has arrived at the TBA for a delivery, the TBA assumes a special role. It becomes imperative on the TBA concerned to act swiftly. The TBA needs to refer cases on time and ensure that referral default is kept at a minimum. According to the health officials “TBAs need to work with the communities since some of them work in isolation. They should take advantage of community leaders and village health communities which exist in their communities. If this is done some of the barriers to prompt care-seeking will be removed”. Number and Reasons for referrals by TBAs Generally TBAs who are trained reported referring clients to the hospitals. The actual referral figures varied from TBA to TBA but overall TBAs reported that they refer 2 –7 people per month on average. In a year as many as 200 women could be collectively referred to the hospital by TBAs in one community. The fact that maternal deaths are quite rare at TBAs seem to indicate that the TBAs are indeed referring high risk cases to the hospital although the hospital staff report that they receive cases from TBAs who are in critical condition suggesting that these referrals are not timely. The reasons for referrals were many and varied. The main reasons for referral according to the TBAs were related to danger signs and obstetric complication which included short women, prolonged labour, anaemia, baby in transverse lie, postpartum hemorrhage, previous scar (a woman who has had an operation), retained placenta, first pregnancy, breech presentation, baby who comes with legs first, malaria, obstructed labour, ante-partum hemorrhage, deformed client (disabled), pre-eclampisia , multiple pregnancies, ruptured uterus, oedema, high blood pressure, big baby and mothers with small passage. TBA utilization levels From the desk study of the documents obtained from the southern region based Safe Motherhood Project, TBAs in Malawi assist in 1 out of 5 births (20%). They also provide treatment for infertility and STIs and some are traditional healers. According to the 1992 Malawi Demographic and Health Survey 18 % of deliveries in Malawi were assisted by TBAs. The 1992 MDHS further indicated that 50% of deliveries were attended by a nurse or trained midwife, 4% by a doctor while 21% were attended by a relative or friend. On the other hand the 2000 Malawi Demographic and Health Survey reports that 22.7% of deliveries were attended to by TBAs, 50. 2% of deliveries were attended by a nurse or trained midwife, 5.4% by a doctor, and 2.4% by no-one. A rural-urban differential was also noted in TBA utilization. According to the 2000 Malawi Demographic and health Survey, in Malawi TBAs assist in 10.5% of live births in urban areas and more two times this- 24.4% ( about a quarter) of live births in the rural areas (32-33). This means that in Malawi the proportion of deliveries being attended to by TBAs increased between 1992 (18%) and 2000 (22.7%) by about 5 percentage points. This may mean that the TBAs are becoming more popular by the day may be through the expansion of TBA training program and their growing integration in the formal health sector. This could also mean that the formal health system is increasingly becoming difficult to access. The findings from the literature review presented above does support the results we obtained during the field visits. The local leaders, community members and the TBAs themselves reported that TBAs are seeing many clients. Sometimes they see more clients than the hospital. The hospital based staff we interviewed also supported this claim saying that the hospitals have more ANC clients but conduct very few deliveries. This may mean that people are going to TBAs for deliveries. Actual TBA utilization rates obtained from the interviews ranged from 10% to 80% of all deliveries depending on the location and popularity of the TBA. The figures reported by the TBAs themselves were, however, very different some seeing as few as 2 women per month and others assisting as many as 20 clients in a single month. How TBAs recognize danger signs of pregnancy, labour and delivery The recognition of danger signs of pregnancy, labor and delivery is key in management of complications. This study attempted to solicit ways and means through which TBA recognize such danger signs. In their responses the TBAs reported that they conduct antenatal clinics where they screen pregnant women for danger signs using the danger signs card provided by the TBA Programme. They also reported that they conduct examinations to assess pregnancy stages and how labour is progressing. They went on to say that they record the onset of labour to monitor progress. They have a danger signs chat which they use when screening women. There was a suggestion from health centre staff that pregnant women should be screened by the skilled attendants themselves and the ones who seem not to be of high risk should be allowed to see the TBAs. This suggestion came about because there are some TBAs who are overconfident. They believe that they can manage some danger signs on their own especially the TBAs who are also practicing herbalists or traditional healers. Knowledge and management of danger signs and obstetric complications by TBAs Almost all respondents that were interviewed reported that TBAs are aware of the danger signs and obstetric complications. They are able to detect haemorrhage, infections, obstructed labour, eclampsia and abortion. According to the TBAs themselves all these danger signs are simply referred to the hospital for appropriate care. For the TBAs, the major obstacle to correct management of these problems is referral logistics such as transport and money problems as well as compliance. Referral default was actually reported by the TBAs. There were TBAs who reported that some pregnant women who were already referred to the hospital showed up again in even more serious condition. One TBAS actually said “Sometimes these clients who have already been referred resurface at the TBAs while already in labour, so we are forced to help them”. The TBA is forced to deal with cases that they would normally refer to the hospital because they fear that if the person dies the relative may argue that if the TBA assisted may be the outcome could have been different. The TBAs, however, contended that there are some women who come late to the TBA without any proper reason. This according to the TBAs also interferes with correct management procedures. The TBAs also pointed out that there were some relatives who may also interfere with TBA referrals for no apparent reason. This may mean that the communities are not aware of the importance of appropriate care seeking especially when danger signs have been noticed. Alternatively this is also an indication that the TBAs are not working with the communities they save. The TBAs argued that referrals may be genuinely adversely affected by the logistical problems of getting clients to a hospital especially when such clients go to TBAs at night. In this regard the role of men was been emphasized. Men need to provide resources and even accompany these women at night when it may be dangerous and even difficult to get to the hospital. Men can carry women on a stretcher or find the quickest means of getting a woman to the hospital. Strengths and weaknesses of TBAs All the respondents cited a number of strengths that TBAs have. These included the fact that they are community based, hence more accessible, they are kind and respected by the community, some respondents also reported that they provide food and warm water for bathing. The communities mentioned that some TBAs have been trained, while others conduct antenatal clinics and visit women and neonates within their communities which they thought was a clear advantage. The weaknesses associated with TBAs were poor working environment, inadequate lighting (especially considering that some of the women deliver at night when it may be even more difficult for them to get to the hospital), small and dirty rooms, poor equipment, lack of supplies, unhygienic procedures, unreasonable fees, illiteracy and old age. The midwives also mentioned that some TBAs are overconfident. They experiment on cases they are supposed to refer which causes delays and worsens the condition of the mother. Some TBAs are also using herbs to induce or speed up labour. This has caused “ruptured uterus” in some cases. Finally, the health personnel were of the opinion that TBAs do not have the skills required to deal with a whole range of problems that pregnant women and newborns face. TBA knowledge and management of neonates Overall TBAs are apparently knowledgeable about neonatal care. According to the TBAs themselves, they clean the baby and wipe the eyes. They also advise mothers to keep babies warm at all times and take sick babies to the hospital On cord care, TBAs advise women not to apply any traditional medicines on the healing navel to avoid infections. They also encourage women to exclusively breastfeed their new babies. Some even ask the women to take the babies to the hospital for vaccinations and there were also TBAs who visit the mothers in their homes to check on how women are looking after their babies. On HIV/AIDS, TBAs advise mothers to bring razor blades of their own and also encourage them to go for VCT where they can be advised on issues like prevention of maternal to child transmission of HIV. Cost-effectiveness of training TBAs as opposed to midwives. Studies in developing countries have shown that training TBAs could dramatically reduce the maternal mortality and other obstetric complications with very low cost and utilizing existing resource (20). The direct assessment of cost-effectiveness of TBAs is very difficult in the presence of serious shortage of staff. What this means is that under such circumstances whatever staff member you can produce in the shortest time possible becomes cost-effective. The training of TBAs is very cost-effective in terms of resource inputs and the current critical shortage of midwives. However, this should be a temporary measure due to the unsatisfactory associated with their practice. This means that long term plans on scaling training and education of midwives should still be intensified.. Effectiveness of TBAs According to the community leaders and the TBAs that were interviewed maternal mortality is rarely reported at TBAs and when it happens it is usually due to delays on the part of the client. It must be pointed out here that there were a lot of communities where maternal death at the hands of a TBA were never reported. This of course does not necessarily mean that TBAs are conducting deliveries well, however, this could be an indication that TBAs are indeed referring high risk cases to hospitals. Another explanation could be that the communities as well as the TBAs were not deliberately reporting maternal deaths for fear of repercussions. Maternal deaths could have also have been simply misclassified TBAs have been trained to be able to report maternal death. One of the charts they use provides for reporting of maternal as well as newborn death. In a hospital based study conducted by Phoya et al in 1990, it was learnt that of 102 cases who died post-natally, 76 delivered in hospital, 4 at a TBA and 22 delivered at home (5). This means that the women who delivered at TBAs were much less likely to die as compared to those who delivered at the hospital and home. This suggests that most of the women who deliver in hospitals report to the facility in critical condition.. TBA Supervision According to the key informants who participated in the study, the Health Surveillance Assistant (HSA) is the immediate supervisor of the TBAs in his or her jurisdiction. However, TBA Co- ordinators are charged with the responsibility of supervising TBAs to ensure that they adhere to the required standards. Some District Health Officers reported that supervision of TBAs has been difficult because the districts are large. They however reported that it is unfortunate that this is happening. Most of the TBAs reported that they are not regularly supervised and it takes time for TBA co-ordinators to visit them. Some of the co-ordinators also agreed that they are not supervising TBAs and in some districts like Lilongwe, TBA training had already stopped since the fate of the TBAs had not yet been established. Some TBAs even reported that they are not supervised at all. A few TBAs,, however, reported that they are supervised either monthly or quarterly. The problems of supervision are also complicated by the recent introduction of the health management information system (HMIS) which now receives returns and records from TBAs. According to the TBA co-ordinators they are not getting the necessary information from the officers concerned which they can then use to improve the delivery of service in the communities where TBAs are based. Overall the supervision of TBAs in the districts that were visited seem to be very erratic, adhoc and inconsistent at best. This is unfortunate because the supervision of TBAs constitutes the major link between them and the formal health care system (20). In the absence of such supervision TBA programmes are unlikely to have any significant positive impact. Conclusion Although the study could not determine the actual contribution TBAs are making towards the reduction of maternal mortality and morbidity it was very clear that TBAs who have been trained can contribute to improving MCH as they offer the only means by which women in rural communities have access to a clean delivery. TBAs, however, can only be effective if availability of transport and accessibility of specialized medical care is addressed. This can ensure that TBAs are effective in linking pregnant women and their new born babies with the formal health care services. This aspect has not been addressed adequately in Malawi as TBA training programmes have emphasized service delivery at the expense of linking TBAs to the health system. A significant proportion of women especially in remote rural areas, are seeking help from TBAs despite problems with quality of their services. The hospital staff acknowledge that they see many women during their antenatal sessions but conduct very few deliveries.There is also a general consensus from skilled attendants that TBAs do not have the skills and competencies they need to impact directly on maternal mortality as well as perinatal mortality. In particular, it was noted that some of the TBAs are overconfident and experiment on cases requiring immediate referral while others are illiterate and elderly. All these adversely affect the quality of their services. Training, constant supervision and effective referral system are necessary if the TBA program is to be effective. Although there is a good referral system in Malawi, logistical issues that have to be dealt with when a referral has been ordered by a TBA should not be underrated. Poor road infrastructure, inadequate telecommunications equipment, economic considerations and inadequate community participation, especially of males increases referral default. This study has also demonstrated that although there are officials entrusted with supervision of TBAs both at district (TBA Co-ordinators and Matron) and community level (HSAs), this supervision is adhoc and inconsistent at best. This is a serious problem as supervision is one of the most effective ways of linking TBAs to the formal health system. Reference
Copyright 2008 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp08020t2.jpg] [lp08020t1.jpg] |
| |||||||||

{kind=link}
{kind=link}