 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 5, No. 2, August, 2008, pp. 126-131 Reproductive Health Knowledge And Practices Among Junior Secondary School Grade One Students In Enugu State: Threat To Achieving Millennium Development Goals In Nigeria Obioma C. Nwaorgu1 , Nkechi G. Onyeneho1, May Okolo1,, Ebele Obadike3, Gloria Enibe3 1Department of Parasitology & Entomology, Received 26th May 2008, Revised 12th June 2008, Accepted 30th June 2008 Code Number: lp08024 Abstract Objective: This was
designed to provide background information for the implementation of family
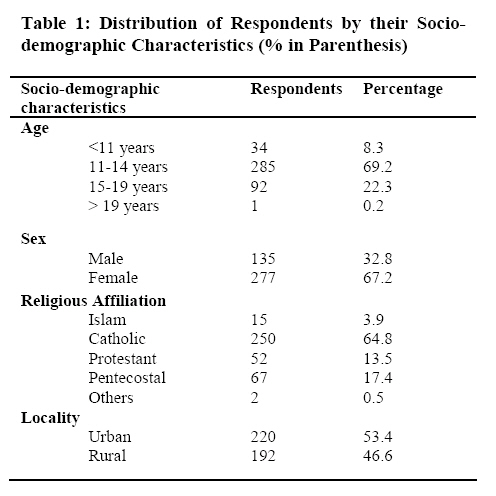
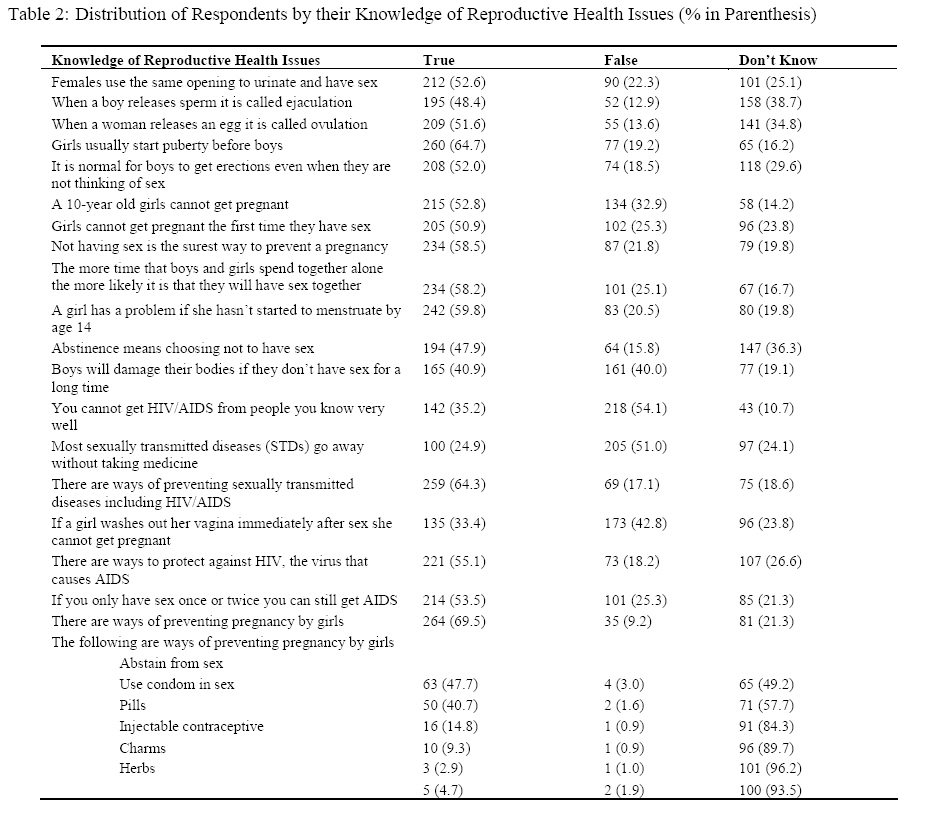
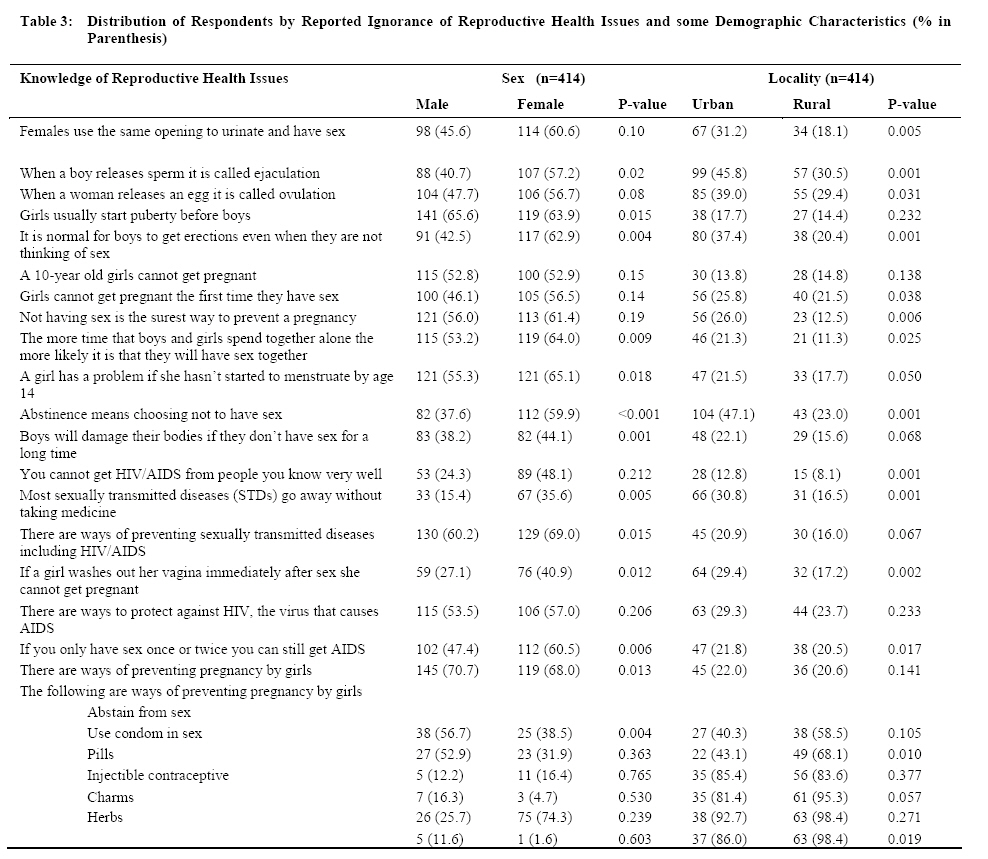
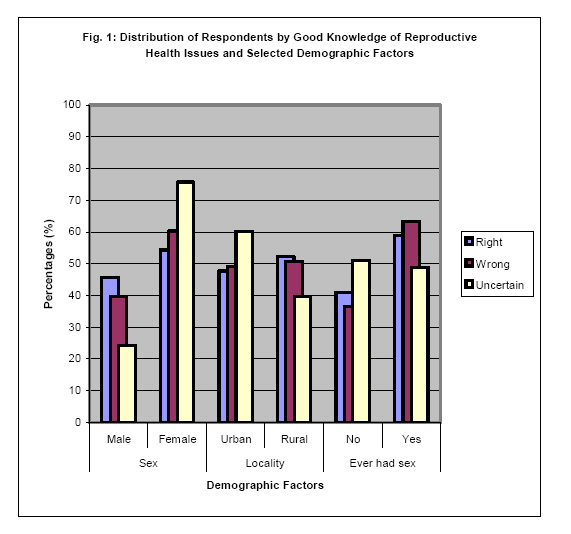
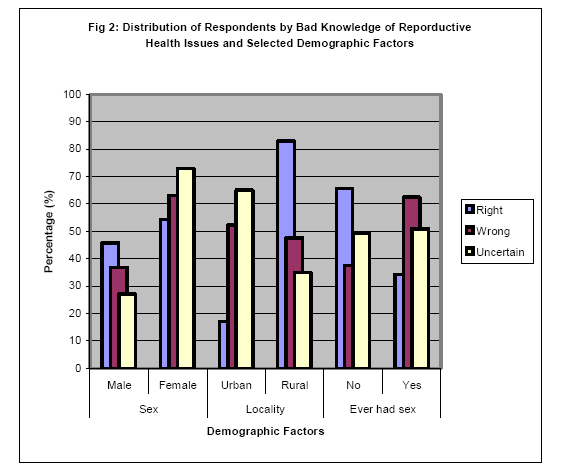
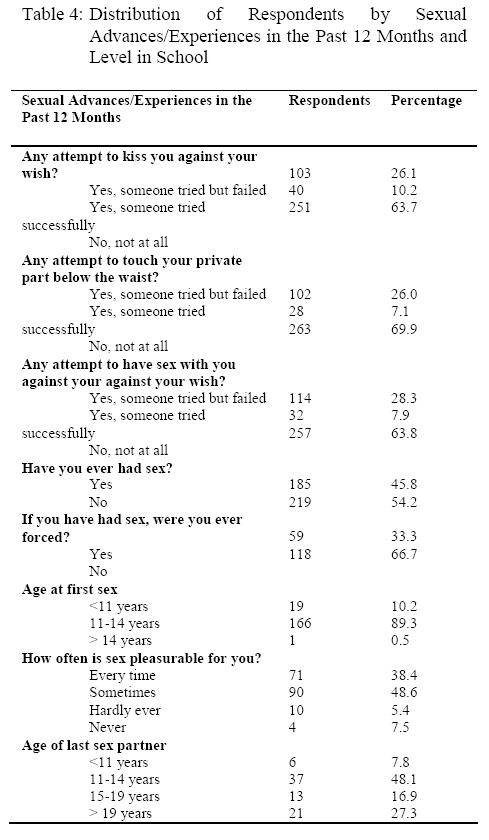
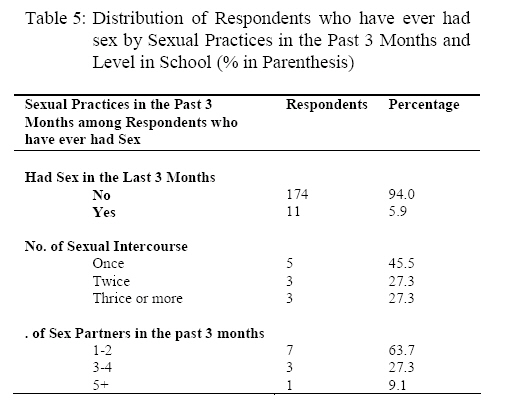
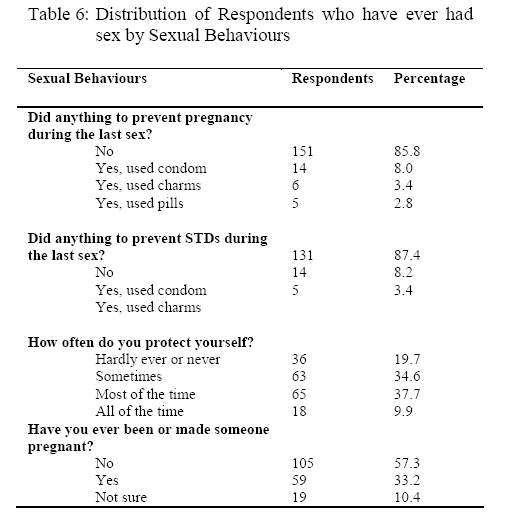
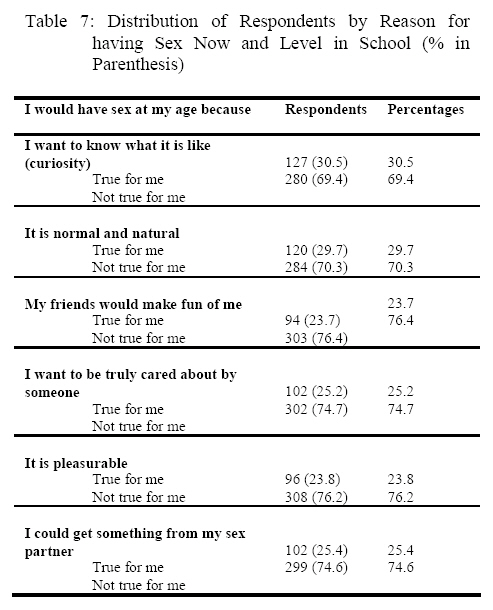
life and HIV/AIDS education in post primary schools in the Enugu State. Keywords: Family-life-education, Nigeria, Reproductive health behaviour, MDGs Introduction The current reproductive health practices among pupils in junior secondary schools in Enugu State constitute substantial threat to the realization of two critical targets of the United Nations millennium development goals (MDGs). These targets include reducing by three quarters between 1990 and 2015, the maternal mortality ratio and to have halted and begin to reverse the spread of HIV/AIDS by 2015 (1). Midway into the target date of 2015, reproductive health practices, which drive the spread of HIV/AIDS and poor maternal health remains a source of concern particularly among the young people in Nigeria. A recent compilation of reproductive health facts of young people in Nigeria revealed that the young people have not been prepared for the attainment of these targets and their goals. The young people aged 10-24 years constitute one-third of the over 140 million Nigerian population (2). This number of young people was projected to exceed 57 million in 2025 (3). The improvements in the sexual activities of this segment of the population are therefore germane to the realization of a society with reduced maternal mortality and one, which has successfully halted and reversed the spread of HIV/AIDS by 2015. It shows that lack of sexual health information and services is exposing these young people to the risks of unwanted pregnancy, illegal and unsafe abortion, sexually transmitted infections (STIs), and HIV/AIDS (4). A National Population Commission survey, showed that over 16% of teenage girls had their sexual debut by age 15 (5). The same survey revealed that 13% of the girls and over 27% of the boys reported exchanging money, gifts or favours for sex in the previous 12 months. Young people also lack knowledge of contraception or at best use it inconsistently (4) Among the teenage girls surveyed by the National Population Commission (5), 37.5% knew some method of contraception; 36.3% knew modern methods. Among their male counterparts, 50.3% knew some modern methods. However, only 29% of the young people in this survey ever used a modern method of contraceptive. Reason for non-use of contraception, among the sexually active single teenagers included fear of complication (46.7% of males and 48.5% of females) and religious and ethical beliefs (12% for males, 21.2% for females). Forty percent of youth believe that condoms, for instance, would reduce sexual fruition and pleasures (6). Traditionally, modern contraceptives, especially the condoms are alien to Nigerian culture. Contraception is neither taught in school by biology teachers nor in the moral instruction of parents at home. The biology teachers only teach ‘what is necessary to pass examinations (7) while the mothers teach them to make good housewives. The young ones are ostensibly protected from getting sexually immoral while they are exposed to the risk of the ubiquitous reproductive health hazards (8). Young women with the risk of unwanted pregnancy take to ineffective methods like douching with vinegar for protection (9). Others take to a number of unorthodox mixtures and techniques after sexual intercourse, hardly conscious of the cost to their reproductive health (8). Unwanted pregnancies among youths disrupt the social development of these girls who live with stigma (10). Mindful of the social stigma of having unwanted pregnancies, many young girls who become pregnant seek abortion as the only way to end unwanted pregnancies. Performing or seeking an abortion is illegal in Nigeria, except to save a woman’s life. Even though Experts estimate that more than 600,000 Nigerian women, most of them young girls obtain abortion each year (11). Otoide et al (12) reported that one-third of women obtaining abortions were adolescents. A survey of post secondary school girls in Enugu State revealed that 21 per cent of the girls surveyed have had unwanted pregnancies and 18 per cent indicated that they have had induced abortion (13). As reported by WHO (14), abortion related complications contribute to 13% of maternal deaths in Nigeria. Concerns for the reproductive health of young people go beyond unwanted pregnancies and abortion related complications and outcomes. There are also the problems of sexually transmitted diseases. Okonofua (15) noted that more than 60% of new HIV infections in Nigeria occur in the youth ages of 15 to 25 years. In a study of rural female teenagers in Nigeria Brabin et al (16) observed that 16.5% of the over 80% sexually active girls had some sexually transmitted infections (STIs). The NPC survey (5) reported that even though most young people knew about HIV/AIDS and gonorrhoea, less than 15% females and 27% males knew about other sexually transmitted infections. This situation poses serious social constraints on the realization of the MDGs with respect to reduction of maternal mortality ratio as well as halting and reversing the spread of HIV/AIDS in Nigeria. It is however hoped that effective, innovative programme to provide the young people with the necessary sexual health information will drive the process of behavioural change and the realization of the MDGs. In meeting this need, the Global Health Awareness Research Foundation (GHARF), a non-governmental organization based in Enugu, with funding support from MacArthur Foundation and in collaboration with the Enugu State Government instituted the family life and HIV/AIDS education (FLHE) into post primary schools curriculum at junior level in Enugu state. As part of the programme, a situation analysis of the reproductive health knowledge and practices of young people in the junior secondary schools in the state was conducted. This paper thus discusses the reproductive health knowledge and practices among pupils in junior secondary school grade one in the state. Methodology Study Design and Area The study was located in Enugu State, south-eastern Nigeria. The people are predominantly Igbo with strong attachment to traditionalism. Though highly Christianized and civilized, the people attach great importance to certain acts considered abominable and sinful against the earth (8). Some of such acts are premarital sex and pregnancy out of wedlock. Adults do not discuss sexuality with the young persons with the fear that they might be exposed to immorality and commit abominable while adolescent receive such information from their peers. The young people, however, access Western cultures through the ubiquitous cyber cafes, now available in the rural areas also, and learn acts. These adolescents strive to experiment what they learnt from these sources without adequate knowledge on how to protect themselves. A cross sectional design was employed in the study, which focused on junior secondary school grade one (JSS1) pupils as the unit of analysis. This is the group that has just completed their first six years of primary education and proceeded to the first secondary education level. Survey method was used to obtain information from these young people. Population and Sampling and Data Collection Enugu State is divided into six educational zones, namely Agbani, Awgu, Enugu, Nsukka, Obollo-Afor and Udi a total of 285 secondary schools and a total student population of 156,800. The target population was students in JSS1 junior secondary one. They constitute one-sixth of the entire student population in the state. In estimating the sample size for the study, 50% probability score at 95% confidence interval with 5% precision level was assumed because there is no known previous publication on the level of knowledge on reproductive health issues among this category of persons in Enugu State. The formula gave a minimum sample size of 384 students. However 412 students were interviewed in the survey. Two post primary schools (one urban and one rural) were randomly selected and sampled from each of the six educational zones in Enugu State giving a total of 12 schools. Thirty-five junior secondary one students were selected by balloting from each of the study schools. A uniform set of an already pre-tested self-administered questionnaire was employed to obtain data from these in school youth. On a Pearson coefficient test, the pre-testing gave positive validity and reliability coefficient of 0.73 and 0.81 respectively for the questionnaire. Results Socio-demographic Characteristics of Respondents More than sixty per cent (67.2%) of the respondents were females. The ages of the respondents ranged from 10 to 20 years with a mean age of 13.5 years and a standard deviation of +/- 1.642 years. The modal and median ages were 13 years respectively. Table 1 also shows that Christian affiliations dominated the study area and majority (64.8%) of the respondents were Catholics. Slightly more than half (53.4%) of the sample resides in urban area. Knowledge, Perceptions and Attitudes about Reproductive Health To test the knowledge of the respondents on reproductive health issues a number of statements were put to the respondents, who were requested to indicate each statement that was “true” and those that were “false”. Table 2 showed a fair knowledge on reproductive health issues among the JSS1 students. However, the data show that in the area of protection the students performed very poorly. In all the methods for preventing pregnancy listed, high proportions of the students were ignorant. Table 3 shows the levels of knowledge of the JSS1 pupils from different locations on reproductive health issues. Even though, in most cases the differences were not statistically significant, more females than males indicated ignorance of their reproductive health issues with regard to (don’t know) common ways of preventing pregnancy among girls. Similarly, more of the rural dwellers indicated ignorance (don’t know) on issues related to ways of preventing pregnancy. The performance of the respondents with different demographic characteristics, with respect to their knowledge on reproductive health matters was also examined. Figure 1 revealed differences in level of knowledge score when considered against the sex and locality of the respondents. There was a significant difference in levels of knowledge on reproductive health issues between the male and female respondents (p=0.0001). More girls than boys were uncertain on the correct options to the questions asked about reproductive health issues. Boys have better knowledge on reproductive health issues than girls. Similarly, it was observed that levels of knowledge on RH issues was better among the rural dwellers than the urban dwellers (p<0.094). Figure 1 also reveals some difference in knowledge between those who have and those who have never had sex. It showed the knowledge score to be better among those who have never had sex even though the difference was not significant (p= 0.081). Figure 2 confirmed the trend in Figure 1 above. It shows that the boys were less certain about what constitutes the wrong ideas about reproductive health systems than the girls (p=0.042). In the same vein, there was a significant difference (p<0.0001) in the proportion of the rural residents, vis-à-vis their urban counterparts that could correctly identify the wrong idea about human reproduction. Over fifty per cent of the urban residents were uncertain about the wrong idea whereas only 34.0% of the rural residents fell into this category. With respect to the distribution by the sexual experience of the respondents, Figure 2 also revealed poor knowledge among those who have ever had sex than among those who have never had sex. It showed that statistically most of those who have ever had sex were uncertain about reproductive health issues (p=0.004). Sexual Practices The respondents were further interviewed on their actual sexual practice within the past 12 months. Table 4 shows that 10.3% of the respondents were actually kissed on the lips within the last 12 months. Within the same period, 7.1% of the respondents were touched in their private parts below the waist while another 7.9% indicated that someone successfully had sex with them. Also 26.1% of the respondents indicated that attempts were made to kiss them on the lips within the last 12 months. Slightly more (28.3%) had sexual advances made to them within the same period. Table 4 also revealed that 45.8% of young persons interviewed have had sex and of this number almost two-thirds (66.7%) did so at their own free will. Most of the participants (89.3%) had their sexual debut at age of 11-14 years and (10.4) at age < 11 years. The age at sexual debut ranged from <11 years to more than 14 years with a mean age of 12.2 years. The median and modal ages were 12 years with a standard deviation of +/- 1.3 years. This shows that at age 12 years most of the young persons have had their sexual debut. Ten percent (10.2%) of these sexually active JSS1 pupils had their sexual debut before their 11th birthday when they should be in primary school. More than a third (38.4%) of the respondents who have had sex indicated that they always find sex very pleasurable. Only 7.5% indicated that they never find it pleasurable. The age distribution of their sex partners shows a range of less than 11 years to more than 49 years, with a mean of 20.75 years and standard deviation of +/- 8.5 years. The median age of their sexual partners is 21 years. More importantly the modal age is 12 years. An examination of the characteristics of these sexually active young persons revealed no statistically significant difference in sex and locality. Thirty of the young persons interviewed reported that they have had sex for a number of times and with various partners ranging from one to more than five (Table 5) in the past 3 months. Table 5 shows that 11 of the respondents have had sex once in the last three months. Six of them have had sex twice or more in the last three months and of this number 4 have had sex with 3 or more persons within the last three months. Table 6 shows that a very great majority (85.8%) of those who have ever had sex did nothing to prevent pregnancy. Similarly, 87.4% did nothing to protect themselves against sexually transmitted diseases during their last sexual act. The Table also revealed that two in every ten sexually active persons interviewed hardly ever protected themselves during sexual intercourse. The reasons why the young persons would indulge in sexual activities irrespective of their age include ‘curiosity’ (30.5%) or ‘it is natural’ (29.7%) and because they hope to get something from the sex partner (22.2%) among other reasons (see Table 7). Discussion The study revealed fair knowledge about reproductive biology, given their age and level of education. This may be attributed to the class work in school. However, the number with misconceptions about very critical elements of reproductive health issues is a source of worry for teachers, parents and practitioners of reproductive health among young persons. They hold misconceptions about reproductive health hazards. More than half (50.9%) of the respondents agreed with the suggestion that a girl cannot get pregnant during her sexual debut. This is akin to what Amazigo (7) described as teaching the pupils only the aspects of reproductive biology to enables them to pass examination but not for self-protection because of existing ethics and norms about sexuality. Level of knowledge on RH issues was also found to be better among the rural dwellers than the urban dwellers (p<0.094). Though this is curious, the poor knowledge among the students with urban background may be linked to the numerous avenues they have to unguarded information outside the school. This also explains the level of misconceptions among the respondents. The rural segment may have depended more on the civil and religious education they get and less of wrong peer influence. The study confirms that young persons are sexually active. Almost half (45.8%) reported having ever had sex, some at very early ages of less than 11 years when they must have been in the primary school and 89.3% between age 11-14 years. A number of them indicated that they have sex even at their young age because they find it pleasurable or because they hoped to gain sometime from it. This bring to fore the reports of NPC (5), which showed that young people engage in sex in exchange for money, gifts among other reasons. This may also explain the variation in the ages of the people they had sex with. The ages ranged from less than 11 years (similar to theirs) to more than 49 years, obviously those that are referred to as ‘sugar daddies and sugar mummies’ in the colloquial parlance. Many of those who are sexually active lack correct knowledge or information on reproductive health issues and worse still engage in unprotected sex for different reasons. Some of them rely on charms to protect them from unwanted pregnancy and sexually transmitted diseases. Some do nothing at all to protect themselves against pregnancy and sexually transmitted diseases. These findings are pointers to the threat the current reproductive health behaviour of these young people in Enugu and indeed Nigeria pose to the realization of the MDG goals in Nigeria. The concern here is that even recent efforts at giving recognition to the reproductive health issues adolescents in the society tended to focus on the unmarried youths in tertiary institution. The younger ones have been taken for granted. The results of this survey revealed young people are sexually active in very young ages. The mean age at sexual debut for the pupils covered in this survey is a pointer to the fact that some of them may have started engaging in sexual activities while still in primary schools. Juxtaposing this on the acknowledged ignorance about protection against reproductive health hazards one is faced with a threatening situation. It follows therefore to avert the imminent threat of not only missing the MDGs but also having an explosion of sexually transmitted infections including HIV/AIDS hazards in our societies; there is urgent need to start earlier to teach them family life and HIV/AIDS education in schools. Adolescents in upper primary school should also benefit from this teaching as already approved by the Federal Ministry of Education. References
Copyright 2008 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp08024t4.jpg] [lp08024t2.jpg] [lp08024t6.jpg] [lp08024t7.jpg] [lp08024t5.jpg] [lp08024t3.jpg] [lp08024f2.jpg] [lp08024t1.jpg] [lp08024f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}