 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East African Journal of Public Heath, Vol. 5, No. 3, December, 2008, pp. 157-159 Iron Deficiency in Frequent and First Time Female Blood Donors M. Boulahriss1 and N. Benchemsi1,2 Correspondence to: M BoulahrissRegional blood transfusion centre, Tel: 00 212 22 20 45 88, Fax: 00 212 22 20 45 89 , E-mail: crtscasa@menara.ma Code Number: lp08029 Abstract Back ground: Blood donation has a marked influence on
the body iron stores especially in female blood donors . Iron deficiency
anaemia is an important limiting factor for the number of donations in female
regular blood donors. Introduction Casablanca blood transfusion centre is the major organization involved in blood banking in Morocco and it collects blood from non-paid volunteers, of whom a considerable proportion donate blood frequently. Blood donation can lead to depletion of iron stores in the body. At each blood donation, approximately 213 mg iron or 9% of the total iron stores in women are lost. With continuous loss of iron, the body adjusts to lower levels of iron storage or results in iron deficiency and anaemia (1). About 28% of women in the reproductive age who donate just two times per year suffer from iron deficiency (2). If the lost iron stores in these donors are not replenished and they continue to donate blood, it results in iron deficiency anaemia and deferral of these donors in the future (3). Thus, a considerable number of regular donors who at present are the best source of safe blood are lost. In fact, iron deficiency anaemia is the main limiting factor in regular donors (1). At present, there is no confirmed or specific programme for prophylaxis of iron deficiency in blood donors. In order to have such a programme, an evaluation of the present situation and accurate statistics of iron deficiency in blood donors is needed. Though most of the researchers have concluded that the frequency of iron deficiency anaemia increases with the number of donations (1,4-7), Birgegard and co-workers have reported that increased number of donations in women does not necessarily result in iron deficiency anaemia (8). There are non accurate statistics of frequency of iron deficiency anaemia in Moroccan blood donors, and it is not possible to use the results of studies in other countries for blood donors in Morocco. Therefore, this study was performed to determine the frequency of iron deficiency and its related factors in blood donors at Casablanca Blood Transfusion Centre. Materials and Methods Between November 2005 and April 2006, we enrolled retrospectively a total of twenty one regular women blood donors who were selected according to the number of previous donations. Only female with at least 10 donations (3-4times per year) were included in frequent blood donors. The group of first time blood donors consisted of twenty-one women who were registered as new blood donors without any prior donation.
After obtaining consent, personal information including age, pregnancy status, previous episode of haemorrhage and previous anaemia was entered and recorded for all donors under study Two tubes of five millilitres blood were drawn from each case for measuring haemoglobin, serum iron, serum ferritin and Total transferrin Binding Capacity (TtBC). Samples were immediately carried out to the laboratory of haematology in EDTA tube for haemoglobin concentrations which were measured by cyanomet haemoglobin method using Coulter® GEN STM System 2 automated and Pasteur Institute of Casablanca for Serum iron, Serum Ferritin and TtBC Concentrations. Serum iron and TtBC concentrations were measured using VITROS 250 system chemistry automated analyser and ortho-clinical diagnostics kit. Ferritin concentrations were measured by the Immuno–Radio-Metric technique (IRMA) using IRMA-mat ferritin of diasorin kit. Haemoglobin and ferritin measurements
Statistical analysis Groups of first time and frequent blood, donors were compared with each other using Student's t-test. Results The population under study was divided into two groups:
Table 1 : Distribution of donors according to iron stores and ferritinemia.
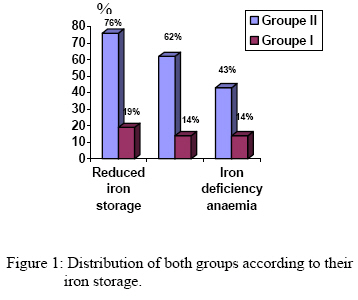
The percentage of iron-deficient women (serum Ferritin concentrations < 15µgL-1 and TtBC > 4mgL-1) increased with increase in number of donations. The frequency of iron deficiency was significantly higher in female regular donors (62%) compared to first time donors (14%) (p < 0.001) (Table 2). Table 2: Distribution of blood donors according to iron deficiency.
Table 3: Frequency of iron deficiency anaemia.
Table 4: Haemoglobin and iron status.
(*** p < 0.001) (** p < 0.01)
Discussion Serum ferritin concentrations had the strongest and most significant relationship with the number of donations compared to other laboratory investigations including haemoglobin and serum iron. Ferritin concentrations decreased significantly with an increase of the number of donations (P < 0.001). Other studies confirm our findings (1,5,7,9-13). As haemoglobin alone do not determine the iron storage levels of iron deficiency and considering the present findings, serum ferritin concentrations can be used as an indicator of the iron stores in blood donors. In the Iranian study 12.5% and 77.8% of first time and regular women blood donors respectively had iron deficiency (2). Other studies reported the same results (13-14). The present study showed that 14% and 62% of first time and frequent blood donors respectively had iron deficiency (Fig 1), which is similar to the findings of Javadzadeh and co workers in Iran. In the present study 76% of regular women blood donors had reduced iron stores (Table 1) with mean ferritin concentrations in frequent blood donors 10 ± 8 µgL-1 which was lower than the mean ferritin concentrations in first time blood donors 32 ± 20µgL-1 (Table 4). We demonstrated in agreement with others (15-17) an increase of gradual iron depletion corresponding to frequency of blood donation. About 62% of women regular donors had iron deficiency and 43% had iron deficiency anaemia. Iron deficiency and iron deficiency anaemia were seen in 77.8% and 55.6% respectively of women regular donors (2). Alvarez et al reported that 30% and 26% of women regular blood donors had respectively iron deficiency and iron deficiency anaemia (15). Cancado and Co-workers showed that 41.5% of women who had donated on several occasions had iron deficiency (14). In our study the frequency of iron deficiency and iron deficiency anaemia in regular women blood donors are higher than the other studies (14-15) but less than the findings of the Iranian study. These results could be due to the higher prevalence of iron deficiency in Moroccan and Iranian women populations due to the nutrition poor in iron. Conclusion Iron deficiency is very common in regular female blood donors at Casablanca’s transfusion centre. Frequent blood donation has a marked influence on the body iron stores in regular women blood donors. It is therefore recommended that blood transfusion centers focused on maintaining iron balance by measuring serum ferritin in women frequent blood donors, they have also to educate the donors about iron supplementation and yearly ferritin checking, for that we propose a schedule to minimize iron deficiency and anaemic complications in women regular blood donors :
As supplementation of iron not only increases the storage of iron in the donors but also leads the donor to donate blood in the future, it is suggested that research studies should be performed to determine the best method of iron supplementation with minimal complications. References
Copyright 2008 - East African Journal of Public Heath The following images related to this document are available:Photo images[lp08029f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}