 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
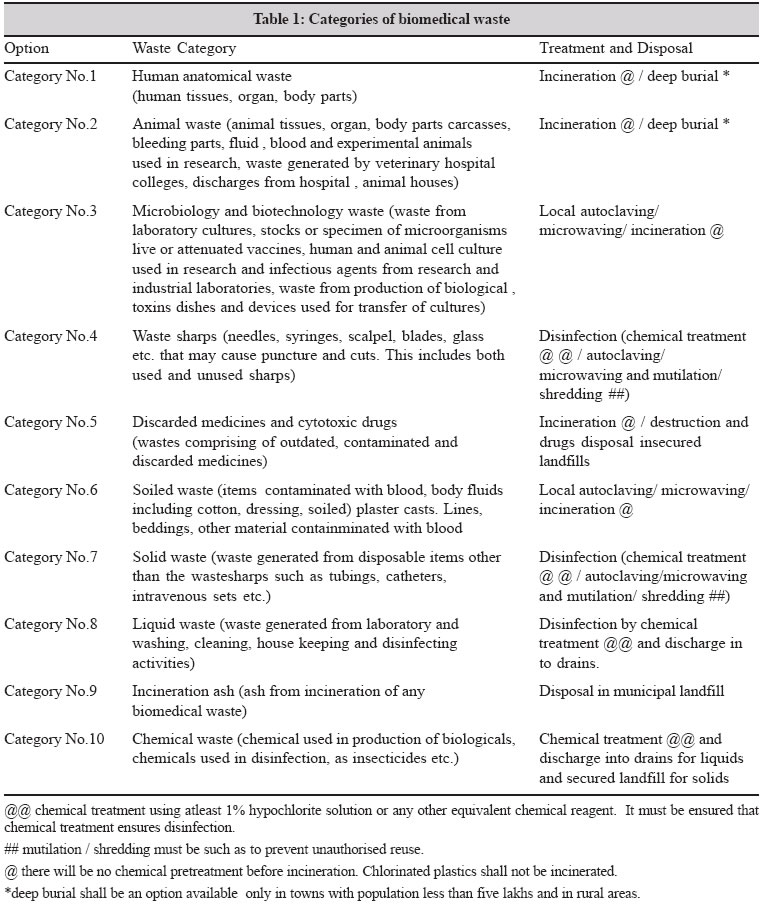
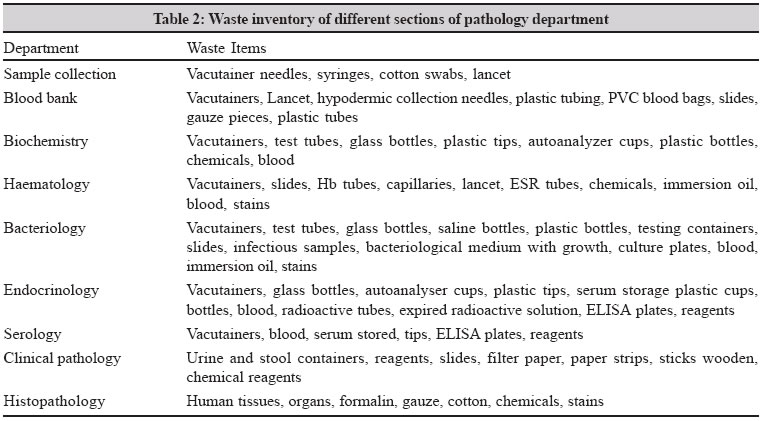
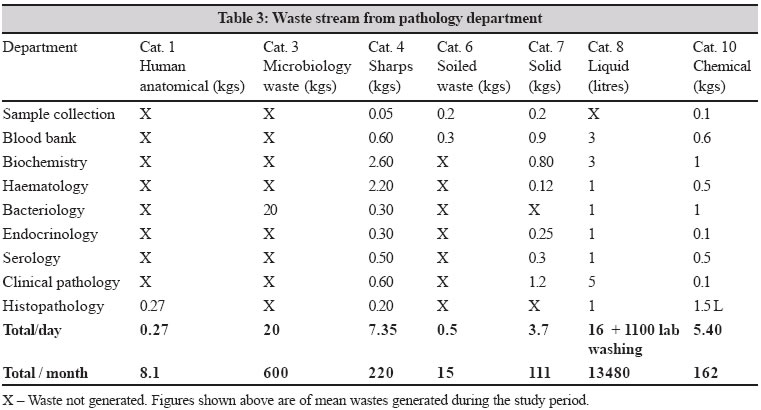
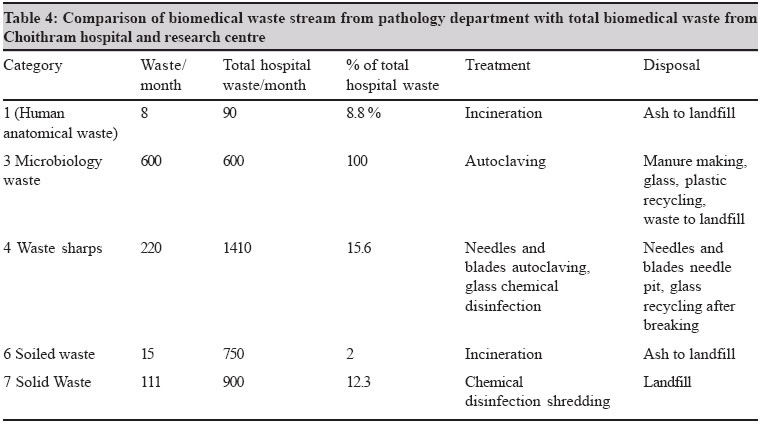
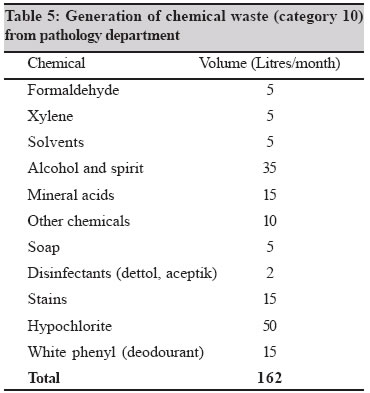
Indian Journal of Medical Microbiology, Vol. 23, No. 1, January-March, 2005, pp. 6-13 Review Article Biomedical waste in laboratory medicine: Audit and management Chitnis V, Vaidya K, Chitnis DS Department of Microbiology and Immunology, Choithram Hospital and Research Center, Indore - 452 001, Madhya Pradesh Code Number: mb05002 ABSTRACT Pathology, microbiology, blood bank and other diagnostic laboratories generate sizable amount of biomedical waste (BMW). The audit of the BMW is required for planning proper strategies. The audit in our laboratory revealed 8 kgs anatomical waste, 600 kgs microbiology waste, 220 kgs waste sharps, 15 kgs soiled waste, 111 kgs solid waste, 480 litres liquid waste along with 33000 litres per month liquid waste generated from labware washing and laboratory cleaning and 162 litres of chemical waste per month. Section wise details are described in the text. Needle sharps are collected in puncture proof containers and the needles autoclaved before sending to needle pit. The glass forms the major sharp category and is disinfected with hypochlorite before washing/recycling. All microbiology waste along with containers/plates/tubes are autoclaved before recycling/disposal. The problem of formalin fixed anatomical waste as histology specimens is pointed out. The formalin containing tissues cannot be sent for incineration for the fear of toxic gas release and the guidelines by the Biomedical waste rule makers need to be amended for the issue. The discarded/infected blood units in blood bank need to be autoclaved before disposal since chemical treatments are difficult or inefficient. The liquid waste management needs more attention and effluent treatment facility needs to be viewed seriously for hospital in general. The segregation of waste at source is the key step and reduction, reuse and recycling should be considered in proper perspectives.Key words: Biomedical waste, audit, management. All pathology, microbiology laboratories and blood banks are governed by the regulations of biomedical waste (BMW) management rules, 1998.[1] However, authorization for handling and management is required for the laboratories with a patient attendance of more than 1000 per month.[2] Microbiologists often are expected to take a lead in programs such as hospital infection control and biomedical waste management. Biomedical waste programs have been largely discussed in India with reference to overall hospital waste management but pathology and microbiology laboratories generate a significant proportion of biomedical waste and have not received much attention. The present article is focused on biomedical waste generated in the laboratories and the practices required in their management. Categories of biomedical waste Ten categories of biomedical waste have been described in schedule I of BMW rules 1998 [Table - 1]. Human anatomical waste is usually generated in operation theatres but a number of specimens are sent to the pathology department for diagnosis. Hence it is a liability of the laboratory to dispose the tissues as biomedical waste. Category 2 (animal waste), category 5 (discarded medicines and cytotoxic drugs) and category 9 (incineration ash) are not generated in a pathology laboratory. Microbiology waste generated in the form of specimen, cultures, tubes and plates used in identification and drug sensitivity test and stock cultures have perhaps the highest infectious potential. However, autoclaving has been a time-tested method of disinfection of microbiology waste. Among waste sharps (category 4) the quantity of glass in pathology is more than needle sharps and category 6 (soiled waste) is a small quantity in form of cotton balls used while blood collection or used as absorbent material for accidental blood and body fluid spillage. Category 7 is the solid waste mainly from disposable items other than sharps for example tubings, tubes and containers used for blood and other pathological samples, blood collection sets in blood bank and blood bags. Category 8 includes liquid waste generated while washing of laboratory waste and processing of samples on the analysers. Category 10 is the chemical waste generated while testing and analysis. Audit of biomedical waste Audit of biomedical waste is required to understand the type and quantity of waste generated. It helps in formulation of the plan for segregation, waste handling and management. Choithram hospital and research centre, Indore is a tertiary care centre in central India. The daily outpatient department (OPD) attendance of patients is 475 while average bed occupancy is around 250 beds. The audit presented here is based on a study carried out during June to November 2002 in the pathology department. The pathology department is further divided into sections like sample collection, blood bank, biochemistry, haematology, bacteriology, endocrinology, immunology, clinical pathology and histopathology. The solid biomedical waste was weighed on weighing machines (kilograms) and liquid was measured in volumes (litres). Non infectious waste Non infectious waste from the pathology department in form of stationary and printed material was 120 kgs/month while packing material cartons, paper, thermocol and plastic was 60 kgs/month. It has been a practice to collect and send the waste paper once a week to central stores for shredding and it is sold for recycling. The non infectious waste needs to be segregated at source to prevent mix up with the infectious waste. Improper segregation will unnecessary increase the load of infectious waste. Waste stream from pathology department The inventory of biomedical waste from each section of pathology department is as in [Table - 2]. The quantum of waste in different sections is detailed in [Table - 3]. Pathology BMW versus total hospital biomedical waste Pathology department forms an important support service section for a tertiary care centre. A comparison of biomedical waste generated vis à vis the total hospital biomedical waste is shown in [Table - 4]. Sample collection section On an average 100-125 patients from OPD visit our sample collection area for giving blood samples and other specimens like urine, stool, sputum etc. Samples from admitted patients are collected by pathology or nursing staff and sent to pathology laboratory. The blood samples are collected in vacutainers. The vacutainer system is expensive than the blood collection by syringe and needle and adding blood samples to in-house anticoagulant /plain containers. However, accidental blood spillages have practically been eliminated after the collection of blood samples by vacutainers. Further, the sample remains sterile and proportion of anticoagulants are constant. However, the vacutainer needles cannot be mutilated conveniently and need to be capped carefully by keeping the cap on the table surface and pushing the needle in it without touching the cap and then fitting the cap. The training needs to be thorough and in our department not a single incidence of needle prick occurred in the last 5 years as against several incidences in the wards while using conventional syringes and needles. The conventional needles are partly mutilated by burning over the electric needle destroyer. All the partly burnt needles and vacutainer needles are collected in blue puncture proof containers. The needles from different sections of the hospital are collected centrally by a deputed person. Needles and sharps from the blue containers from wards and labs are transferred to metal box carried on a trolley. The supervisory staff in all the wards and laboratory have to sign a register circulated by the deputed person as part of documentation system. The needles from all over the hospital are collected in the metal box and passed on to the microbiology laboratory for autoclaving in disposal autoclave and the autoclaved needles are transported to burial pit for needle disposal. Autoclaving was started instead of chemical disinfection with 1 % hypochlorite as research conducted at our end has shown the limitations of hypochlorite.[3] The needle burial pit is a cemented tank with a lock and key system. The blood contaminated cotton swabs form a small amount of solid soiled waste of pathology laboratory. It is discarded in red bags which are incinerated. A documentation register has been made for the blood contaminated cotton swabs as category 6 and blood collection sets as category 7. Bacteriology All the culture plates, drug sensitivity plates, culture material with bacterial growth in liquid or solid media in tubes, bottles and plates and specimens from patients are collected in stainless steel trays which are directly loaded in to autoclave. The autoclave holding time is 1.5 hours at 121°C (15 lbs psi). The melted media and liquids in the containers (after autoclaving) are emptied in stainless steel buckets and the plastic/glass containers are washed and reused. Microscopic slides used in microbiology are also autoclaved in disposal autoclave before discarding as glass sharps and sent for recycling of glass. The material not required for further reuse in the laboratory is transported to central stores for recycling. The plastic glass material is segregated and the contractor transports the same for recycling. It is important to note that all the organic matter collected from autoclaved containers (600 kg/month) is added to a microbiology manure pit for manure making. This also includes the discarded blood units (HIV, HBV and HCV reactive units or contaminated and expired units). Our earlier work had pointed out the limitations of the use of hypochlorite and difficulties with formaldehyde for the disinfection of blood units.[4] Autoclaving was found to be the best way of decontamination of blood units before disposal. Further, documentation of quality assurance tests for autoclaving are essential. The chemical sterilization indicator tape is used for every cycle and biological indicator is used once in 15 days at our end. The autoclave is fitted with thermograph. The documentation register which is daily submitted to director medical services has the following columns :date, weight of load, pressure and temperature attained. Biochemistry The section receives approximately 250 blood samples in vacutainers. Samples for sugar testing are spun and plasma at the top pipetted out directly for tests over autolab analyser. The plasma/serum from the samples for other tests are separated and stored in 4 mL polypropylene storage vials. Bulk of the biochemistry tests are run over Hitachi 04, Detona autoanalyser and Elite electrolyte analyser. Biochemistry analysers require approximately 300 microcups. Post analysis plasma/ serum/blood from various containers is decanted carefully into stainless steel kettle and the containers with residual blood/plasma are discarded in buckets containing 10 litres of 1% hypochlorite. This practice is adopted because our earlier work has shown that hypochlorite gets masked with blood and huge volumes of hypochlorite will be required.[5] After 1 hour immersion of the containers in hypochlorite, the disposable containers are sent to central stores for disposal. The containers which are to be reused are taken up for washing. The residual hypochlorite used for disinfection is drained into sink. The blood/plasma/serum decanted in stainless steel kettles is autoclaved in disposal autoclave in microbiology before disposing it to manure pit. Biochemistry laboratory uses about 500 microtips which are also disinfected with hypochlorite before reuse or disposal as plastic waste. Glass tubes used for biochemical analysis are also disinfected with hypochlorite before washing. Blood samples for blood gas analysers are received in syringes capped with needles. The needle portions are discarded as sharps and the plastic syringes as plastic waste (detailed in sample collection section). Haematology About 125 samples in vacutainers are received daily in haematology. The vacutainers containing blood are treated for disinfection with hypochlorite as detailed in biochemistry section. Almost 150 blood smear slides covered with immersion oil accumulate in haematology every day. These slides are boiled with detergent and washed and reused in clinical pathology and blood bank. ESR is performed in disposable polystyrene westergreen tubes and discarded in red polythene bags which are sent for incineration. Prickers and capillaries for bleeding time and clotting time are discarded in blue colored puncture proof containers and disposed off as sharps as mentioned in collection section. Clinical pathology About 100 urine samples and 40 stool samples are received daily. Urine and stool is flushed in toilet and the containers are sent to central hypochlorite tank of the hospital. After hypochlorite treatment the plastic containers are sent as plastic waste. The polypropylene tubes used for centrifuging urine samples are decontaminated with hypochlorite before washing and reusing. Endocrinology and immunology These sections receive about 150 samples daily and the general handling and disposal is as detailed in biochemistry section. The department has voluntary testing and counselling centre for AIDS and infectious disease. Screening for blood bank is also carried out in the immunology section. Radio immuno assay laboratory follows the guidelines of radiation protection committee of BARC. Briefly the liquid radioactive waste Iodine125 is kept for 3 months before draining into the sinks. The plastic waste contaminated with radioactivity is stored for 3 months before decontaminating with hypochlorite and disposed as plastic waste. It needs to be mentioned that RIA laboratory has to primarily follow the guidelines from radiation protection committee. Histopathology Total quantity of anatomical waste in the form of histopathological specimens is around 8 kgs/month. The BMW rule has no option other than incineration for the anatomical waste. However, the rule also states that no chemical treatment needs to be given for the material which is incinerated. The tissues in histopathology are fixed in formalin and as a result are free of live organisms of any type but formalin treatment makes it unfit for incineration and toxic gases are likely to be released on incineration. The BMW rule makers must look into this anomaly and an alternative needs to be suggested. The reasons for incineration of anatomical waste appear to be aesthetic and sentimental. It is feared that cremation will not be accepted by communities. At our end, we wash the tissues with water to remove formalin and then send in yellow bags for incineration. Even if alternatives like burial is suggested in the BMW rules, thorough washing of tissues to remove free formalin is necessary to allow biodegradation during burial. Histopathology section also generates hazardous chemical waste like formalin and xylene. BMW rule has not clarified the disposal of such chemicals. Blood bank On an average 800 - 900 units of blood is collected every month and 60% of the units are given as blood components. Approximately 80 units are discarded as reactive for HIV/HBsAg/HCV or contamination/reactions to recipients and expired units. These discarded units are sent to disposal autoclave in microbiology. The reasons for selection of autoclaving as against chemical disinfection with hypochlorite or formalin have been explained earlier. After autoclaving, the blood is sent for manure making and plastic material as category 7 waste for shredding. Disposal of sharps is an important BMW issue in blood banks. Lancets or prickers used for rapid blood group screens and the needles of donor sets form the major sharps. The lancets are discarded in blue capped puncture proof containers. After blood collection, sample remaining in the tubing is aliquoted in plain and citrate tubes for infectious disease screening and cross match and the needles containing portion cut and added to sharp disposal containers. As pointed out earlier, all sharps are collected centrally, autoclaved and disposed in secured needle pit. The glass tubes and plastic tooth picks for mixing blood and reagents for blood grouping are discarded in trough containing hypochlorite. The tooth picks are subsequently discarded as plastic waste while glass slides are washed and reused. The glass tubes and blood containing materials are disinfected and washed as mentioned in biochemistry section. The blood donor sets, after cutting out the needle parts, are discarded in metal boxes which are sent for autoclaving in microbiology disposal autoclave before sending the plastic for disposal. This practice of autoclaving is used because the blood containing tubings, being made of polyvinyl chloride, cannot be incinerated as incineration of PVC material leads to release of toxic dioxins. Liquid waste Liquid waste generated from laboratory washing, cleaning and disinfecting activities has to be disinfected by chemical treatment before discharging in drain. However, it is not practical to disinfect huge volumes of liquid waste as seen in [Table - 4]. Instead, the practice of disinfection for blood containers is a better approach. Blood samples received for analysis are carefully decanted in metal kettles and are autoclaved in disposal autoclave. The small amount of residual blood in the containers is disinfected by hypochlorite. The routine washing procedures (after disinfection of the labware contaminated with blood or body fluids) could be discharged in the drain. However, hospital liquid waste is likely to contain pathogens and noteworthy have been the multidrug resistant bacterial pathogens.[6] In view of this, the hospitals in cities, where central municipal effluent treatment plants are not available, can have their own effluent treatment facility. We have installed effluent treatment plant which can treat over 3 lakh litres of effluent and makes available 3 lakh litres of treated water that can be used for sanitary cleaning and green belt irrigation. Chemical waste It includes chemicals used in testing and processing during analysis and also chemicals used in disinfection. Chemical treatment with hypochlorite has been suggested for chemical waste treatment in BMW rule but we consider this inappropriate since treatment with agent like hypochlorite cannot neutralize the chemical waste. More practical and appropriate approach needs to be decided in the BMW rules. Presently, the final dilution of drain needs to be considered. The audit of the chemicals used in our laboratory is displayed in [Table - 5]. The total volume of hospital effluent per day is around 3 lakh litres and hence the final dilution appears to be very high. Emphasis on recycling Recycling of disinfected waste needs to be emphasized and the new amendments in BMW in this regard are expected shortly. The autoclavable plastics, glass tubes and petri plates after disinfection can be washed and reused. The disinfected plastic waste could be shredded and then passed on for plastic recycling. For the fear of the use of duplicated supplies or unauthorized usage, the mutilation or shredding of glass is also suggested in the BMW rules. However, shredding of glass bottles results in to sharps that are likely to be hazardous while collection and handling. Hence, we feel that the glass bottles, if contaminated, could be disinfected but mechanical crushing could be avoided before sending for recycling. The main problem arises for the disposal of sharps such as needles. Presently burial in secured pits has been suggested in BMW rules. However, smelting for metal extraction needs to be persued as an alternative. Practice for smaller laboratory setups The detailed practice for larger hospital laboratories is mentioned above. The smaller laboratory setups, including those which cater to patient population of less than 1000 per month, need no authorization for biomedical waste but they are also supposed to follow the guidelines of biomedical waste rules. All the needle sharps could be mutilated and discarded in puncture proof containers which could be handed over to common central biomedical waste management facility. In absence of common facility, the sharps could be discarded in metal container which can be disinfected in oven/autoclave and sent to secured landfill. The blood/body fluid soaked cotton/gauze could be discarded in coloured polythene bag which could be sent to common facility or autoclaved and then the material sent as general non infectious waste. The practice of careful decanting of infectious waste like blood and body fluid samples into a metal kettle and then disinfecting the containers containing small amount of liquid waste by immersion in 1% hypochlorite before washing the containers should be practiced. The kettles containing blood/body fluids could be autoclaved before discarding the waste as non infectious material. The gloves used in the laboratory could also be disinfected with hypochlorite before mutilating and disposal. Histopathology specimens could be washed with water to remove formalin and then sent in yellow polythene bags to central common facility for incineration. The most important infectious material is bacteriology waste in the form of cultures/samples and needs to be autoclaved before washing/disposal. Finally, we all must remember that the proper BMW management is the responsibility of the generators of waste and it is our moral duty to take care of the waste so that ourselves, our staff members and the community at large is protected from the risks of hazards of biomedical waste. ACKNOWLEDGEMENT The authors wish to acknowledge the financial support given by the hospital management in carrying out this waste audit study. REFERENCES
Copyright 2005 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb05002t1.jpg] [mb05002t2.jpg] [mb05002t5.jpg] [mb05002t3.jpg] [mb05002t4.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}