 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
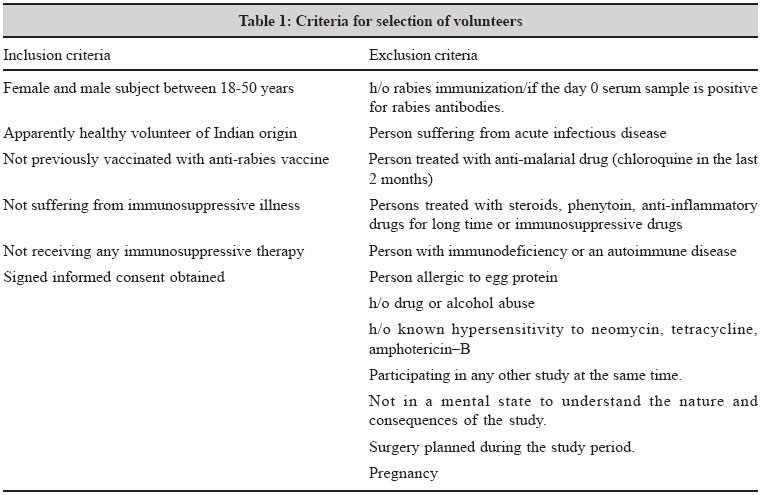
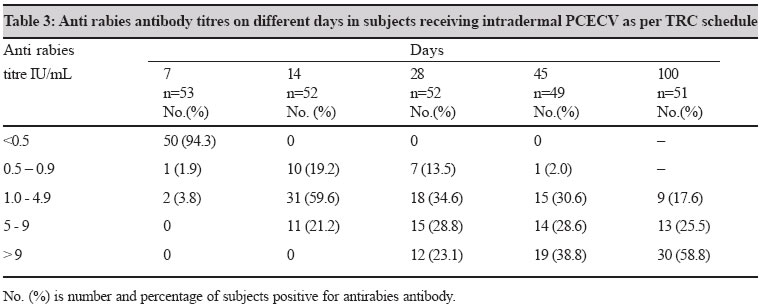
Indian Journal of Medical Microbiology, Vol. 23, No. 1, January-March, 2005, pp. 24-28 Original Article Safety and immunogenicity of the Intradermal thai red cross (2-2-2-0-1-1) post exposure vaccination regimen in the Indian population using purified chick embryo cell rabies vaccine Chhabra Mala, Ichhpujani RL, Bhardwaj M, Tiwari KN, Panda RC, Lal S National Institute of Communicable Diseases, Sham Nath Marg, New Delhi - 110 054 Code Number: mb05005 ABSTRACT PURPOSE: To test the immunogenicity of the WHO recommended "2-2-2-0-1-1" post-exposure rabies vaccination regimen in Indian subjects to determine the feasibility of replacing crude sheep brain nerve tissue rabies vaccine with modern tissue culture rabies vaccine at major anti-rabies treatment centers throughout India.METHODS: Purified chick embryo cell vaccine (PCECV) was administered in the dosage of 0.1mL per site to 53 Indian subjects. RESULTS: All subjects produced rabies antibodies above 0.5IU/mL by day 14 post-vaccination. Only minor adverse reactions including swelling (6.6%), erythema (5.4%) and pain (1.4%) were observed for which no treatment was required. CONCLUSIONS: This study demonstrated that PCECV is safe and highly immunogenic in Indian subjects when administered intradermally as 0.1mL/site using the "2-2-2-0-1-1" post-exposure regimen. Key words: Rabies, post-exposure prophylaxis, intradermal administration, tissue culture rabies vaccine, rabies antibody. As a direct result of the development of modern tissue culture rabies vaccine (TCV), rabies post-exposure prophylaxis has become safe, virtually painless and a less cumbersome procedure to administer.[1] Unfortunately, in India a large number of people exposed to bites from potentially rabid animals do not have the financial means to receive TCV and therefore still receive reactogenic nerve tissue vaccine (NTV) produced from rabies virus infected sheep brain tissue. To help resolve this problem, the World Health Organization (WHO) recommended the discontinuation of the production and usage of NTV in 1992 and national authorities have demonstrated a commitment to phase out its use in favour of TCV.[2] Epidemiological data collected from field studies conducted by the National Institute of Communicable Diseases in Delhi indicate that approximately 2.12 million animal bites occur annually. Of these, 1.1 million patients elect to receive post exposure treatment (PET), 0.45 million of which receive NTV which is given free of charge in the public sector and 0.65 million patients receive TCV on a self-financing basis.[3] The main limiting factors for replacing NTV with TCV are the limited availability and high cost of TCV. Non-availability of appropriate seed virus and cell lines has further hampered large-scale indigenous production of TCV in India. To help overcome these obstacles, WHO has recommended the intradermal route of administration of TCV for PET.[4] There are three types of TCV and one duck embryo vaccine presently available in India including: human diploid cell vaccine (HDCV), purified chick embryo cell vaccine (PCECV), purified vero cell rabies vaccine (PVRV) and purified duck embryo vaccine (PDEV). Based on immunogenicity, efficacy, and safety, WHO recommended a limited number of commercially available vaccines for PET using the intradermal route of injection.[4] WHO also recommends two intradermal vaccination regimens for PET including the "8-0-4-0-1-1" schedule, also known as the "Oxford" regimen for use with HDCV and PCECV and the "2-2-2-0-1-1" regimen, also known as the "Thai Red Cross" regimen for use with PVRV, PCECV, and PDEV. The "2-2-2-0-1-1" vaccination regimen consists of intradermal injections of either 0.1mL for PVRV and PCECV or 0.2mL for PDEV at two locations (one in each upper deltoid region) on days 0, 3 and 7, and at one location in the upper deltoid region on days 30 and 90. Thailand, Sri Lanka and Philippines have now adopted the use of intradermal route for PET and successfully incorporated it into their national rabies prevention programs.[5] However, up until the present time, India has not widely embraced the use of intradermal TCV for PET due to insufficient data in the Indian population. The present study was undertaken with the objective to determine the immunogenicity, reactogenicity, and acceptability of intradermal administration of TCV in the healthy Indian volunteers. MATERIALS AND METHODS Ethical clearance The protocol for the clinical trial was reviewed and approved by the ethical committee of the National Institute of Communicable Disease in Delhi, India, prior to enrolment of subjects and commencement of the study. Subjects Sixty-three employees volunteered to participate in the study. All subjects involved in the study were healthy volunteers of Indian origin, not previously vaccinated with any rabies vaccine. Subjects were either working at the Infectious Disease Hospital where patients with clinical rabies are managed, or were working in field units of the epidemiology branch of the Municipal Corporation of Delhi and involved in some activity pertaining to control of animal rabies, i.e., dog catchers. All subjects that participated in the study were at increased risk of exposure to rabies due to their vocation. Informed written consent was obtained from all subjects prior to enrolment. Inclusion and exclusion criteria were defined [Table - 1]. Persons suffering from acute infectious diseases, immunosuppressive illnesses, or receiving any immunosuppressive therapy were not included in the study. Individuals taking any anti-malarial drug in the last two months prior to enrolment were also excluded from the study. All subjects were advised to abstain from the use of alcohol during the study period. Vaccine Purified chick embryo rabies vaccine (PCECV), purchased from the market with label potency of >2.5 IUmL, was used throughout the study. The vaccine was reconstituted with 1mL of diluent provided by the manufacturer and was used within 6 hours of reconstitution, as per WHO recommendations. Study protocol All subjects received the Thai Red Cross ("2-2-2-0-1-1") PET vaccination schedule as recommended by WHO. Subjects were administered 0.1mL of PCECV intradermally into each deltoid on days 0,3], and 7 and an additional 0.1mL of PCECV in one deltoid on days 28 and 90. No vaccine was given on day 14. Blood samples were collected on days 0, 7, 14, 28, 45 and 100. Serum was separated and stored at -20°C until tested for the presence of antibodies to rabies virus. Vaccinators Three nurses, previously employed as BCG technicians, with extensive experience in the technique of intradermal injections administered all vaccines. In addition, a physician supervised each intradermal inoculation. Case records A detailed case record file (CRF) was maintained for each patient. The CRF contained the signed consent form, a detailed demographic profile including age, sex and address, a medical history of concomitant illness and medication, and general examination findings including height, weight, body temperature, pulse rate and blood pressure. Body temperature was recorded at the time of each visit. Adverse reactions were noted on every visit subsequent to vaccination. Evaluation of rabies antibodies The titration of rabies antibody was completed by a commercially available enzyme immunoassay kit (ELISA kit-PlatelliaR Rabies kit, Bio Rad). The test was performed exactly as per the manufacturer′s protocol. Negative and positive control sera were evaluated with each test in order to validate the quality of detection and establish the reference curve. All serum samples and controls were tested in duplicate as recommended in the product protocol. The reference curve was plotted with mean corrected ODs and used to calculate the titres of unknown sera. RESULTS Subjects and demographics Fifty-three of the 63 subjects that initially volunteered to participate successfully completed the study as per the protocol. Four subjects dropped our after the first vaccination visit, three subjects were unable to complete the vaccination due to scheduling conflicts, one subject underwent surgery and was dropped from the study and two subjects dropped out due to personal family reasons. The per protocol population consisted of 20 males and 33 females (M:F = 1:1.65), and ranged in age from 20-58 years of age (mean age 38 years) and in weight from 41-90 Kgs (mean weight 64Kgs). In the per protocol group, five subjects had been taking anti-hypertensive medication for approximately one year, three subjects were taking anti-lipidemic drugs due to a deranged lipid profile, two subjects were suffering from common cold and two subjects experienced minor injuries during the study and were administered tetanus toxoid, antibiotics, and analgesics. Sixty three vials of vaccine were used to complete the immunization of the 53 subjects in the per protocol population. Adverse reactions No severe adverse reactions were recorded in any of the volunteers. Reported adverse reactions in decreasing order of frequency were swelling (6.6%), erythema (5.4%) and local pain (1.4%) [Table - 2]. No subjects needed any treatment for the reported adverse reactions and all were self-limiting. No systemic adverse reactions occurred in any of the subjects. Presence of rabies antibody None of the subjects had a detectable level of rabies antibody on day 0. Rabies virus antibodies were detectable in 5.7% of the subjects by day 7 and all subjects had antibody titres at or above 0.5 IU/mL by day 14 [Table - 3]. Titres of all subjects remained above 0.5 IU/mL through day 100 when the study was terminated. DISCUSSION In the present study all the subjects vaccinated intradermally with 0.1 mL PCECV using the "2-2-2-0-1-1" regimen produced rabies antibody titres above 0.5 IU/mL by day 14. The findings are in corroboration with the findings reported in the literature. Briggs et al[6] reported anti-rabies antibody titres of above 0.5 IU/mL in all the 58 subjects who received intradermal PCECV by TRC schedule in 0.1 mL dosage per site. Madhusudana et al[7] and Charanasri et al[8] also reported similar findings in 25 and 65 volunteers respectively who received PCECV in similar dosage and schedule. In addition, in the present study, the immune response to the intradermally administered vaccine was unaffected in subjects concurrently taking medication in the form of analgesics or antibiotics for any associated illness. The adverse reactions observed in subjects that participated in the present study were mild, occurred at the site of injection only and resolved without treatment as have been reported in other intradermal studies.[6],[7],[8] The presence of rabies virus neutralizing antibodies has been reported to correlate with the protection against rabies and WHO recognizes a level 0.5 IU/mL as being an adequate level of antibody after vaccination.[2] In the current study, sera were evaluated for the presence of rabies virus antibodies using a commercially available ELISA test. The ELISA test measures the presence of rabies antibody in serum and does not require a highly specialized bio-containment laboratory facility to handle live rabies virus. Recent published reports have established ELISA as a reliable means of evaluating the presence of rabies virus antibody and have indicated that the antibody measured by ELISA is the same spectrum of antibodies as is measured by the fluorescent antibody virus neutralization test (FAVNT) and have determined that antibody levels as measured by ELISA and FAVNT are well correlated with protection against rabies challenge.[9],[10] The PET protocol for NTV consists of injecting either 2 mL (for children) or 5 mL (for adults) of NTV subcutaneously into the abdomen on 10 consecutive days followed by 2 to 4 booster injections. In many Asian countries NTV in public sector is provided free of charge to patients that may be exposed to rabies through bites from dogs and other potentially rabid animals. The cost of PET for millions of patients bitten or otherwise exposed to risk of rabies in Asia is beyond what they can afford and therefore they depend on government sponsored anti-rabies treatment centers to provide low cost or free PET. The financial burden for many Asian governments to replace NTV with intramuscular administration of TCV is prohibitive and therefore WHO has strongly recommended that these countries consider implementing either the reduced dosage intradermal regimen "2-2-2-0-1-1" or the "8-0-4-0-1-1" regimen. In any large anti-rabies clinic in India about 100-150 patients report for anti-rabies vaccination per day.[11] The present patient load would be reduced by approximately 50% if NTV were to be replaced by TCV as only 5 visits are required compared to the 10+ visits required for the administration of NTV. In India, one third of all patients seeking PET have experienced category III exposure requiring administration of rabies immunoglobulin. However, very few patients receive RIG either due to non-availability, high cost, or the fact that many physicians are unwilling to administer it. Without the additional immediate passive immune protection of RIG, it is of utmost importance to protect patients by inducing a rapid immune response through the administration of TCV. The economical advantage of using intradermal regimens is obvious, as theoretically only 0.8mL of vaccine is needed for each patient, resulting in the use of one vial per patient, as opposed to five vials per patient that receive PET using the intramuscular route. In the present study, we were able to retrieve between 6-8 0.1 mL doses per reconstituted vial and used 63 vials of PCECV to complete the immunization of 53 patients using the "2-2-2-0-1-1" regimen. It would have taken 265 vials of vaccine to immunize the same number of patients using the five-dose intramuscular Essen schedule. One dose of TCV costs approximately $ 6 US in India (cost of 53 vials = $ 318, cost of 265 vials = $ 1590). Thus, the use of the intradermal TRC regimen reduced the vaccination cost by about 80% in our study. Clearly this makes the "2-2-2-0-1-1" intradermal regimen an attractive option for resource-starved countries. Although the literature reports a rapid immune response by day seven in patients that received the "8-0-4-0-1-1" intradermal regimen,[5],[12] the operational problems associated with the use of this multi-site regimen discourage its wide spread use in countries like India. By significantly reducing the cost of PET in developing countries more patients will be able to afford modern TCV and will not have to suffer from the neuroparalytic reactions caused by NTV.[1] In conclusion, where the cost of rabies vaccines plays a determining role as to whether developing countries can afford to replace NTV with TCV for PET, the intradermal administration of vaccines like PCECV provides a viable solution and should be considered safe, immunogenic and efficacious. REFERENCES
Copyright 2005 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb05005t2.jpg] [mb05005t3.jpg] [mb05005t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}