 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
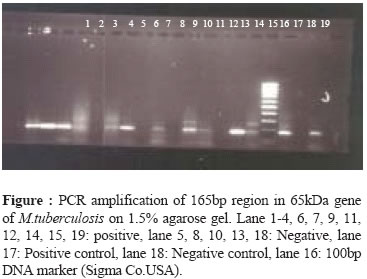
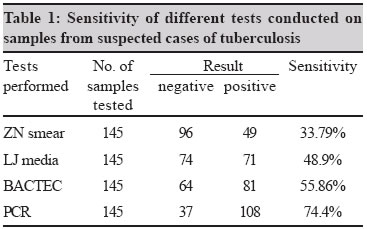
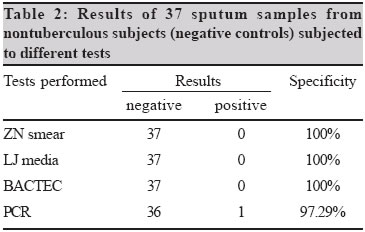
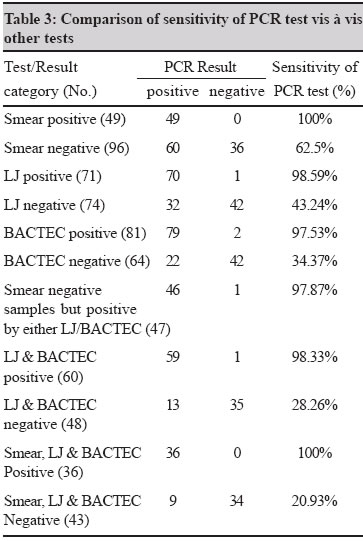
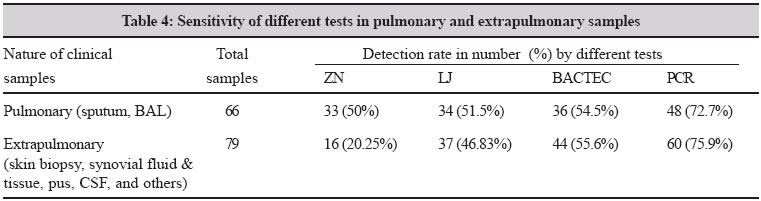
Indian Journal of Medical Microbiology, Vol. 23, No. 1, January-March, 2005, pp. 29-33 Original Article Comparison of the conventional diagnostic modalities, bactec culture and polymerase chain reaction test for diagnosis of tuberculosis Negi SS, Khan SFB, Gupta Sunil, Pasha ST, Khare S, Lal S Department of Microbiology, National Institute of Communicable Diseases, New Delhi - 110 054 Code Number: mb05006 ABSTRACT PURPOSE: To evaluate the performance of 65 kDa antigen based PCR assay in clinical samples obtained from pulmonary and extrapulmonary cases of tuberculosis.METHODS: One hundred and fifty six samples were processed for detection of Mycobacterium tuberculosis by ZN smear examination, LJ medium culture, BACTEC radiometric culture and PCR tests. RESULTS: A significant difference was seen in the sensitivities of different tests, the figures being 74.4% for PCR test, 33.79% for ZN smear examination, 48.9% for LJ culture and 55.8% for BACTEC culture (P<0.05). However, there was no significant difference (P>0.05) as far as specificity of different tests was concerned. PCR test sensitivity in pulmonary and extrapulmonary clinical samples were 72.7% and 75.9% respectively and found to be significantly higher (P<0.05) when compared with those of other tests. The mean detection time for M.tuberculosis was 24.03 days by LJ medium culture, 12.89 days by BACTEC culture and less than one day by PCR test. CONCLUSIONS: PCR is a rapid and sensitive method for the early diagnosis of pulmonary and extrapulmonary tuberculosis. Key words: Tuberculosis, M.tuberculosis, PCR, LJ medium, BACTEC Tuberculosis (TB), one of the major air borne infectious bacterial disease, remains a major world wide health problem with global mortality ranging form 1.6 to 2.2 million lives per year.[1] the situation is further exacerbated with the increasing incidence of drug resistant TB.[1] Early diagnosis plays a vital role in control of TB. Diagnosis of mycobacterial infections, however, remains an enigma. Although acid fast bacilli (AFB) microscopy, and conventional Lowenstein Jensen (L-J) culture remain the cornerstone of the diagnosis of TB, these traditional bacteriological methods are either slow or their sensitivity is quite low, especially with clinical samples that contain small number of organisms.[2] This can affect treatment by either delaying it or causing inappropriate empiric therapy for TB to subjects without mycobacterial infections or with atypical mycobacteria.[3] Several studies have been done to detect M.tuberculosis in respiratory and other clinical samples by amplifying different DNA sequences of M.tuberculosis by polymerase chain reaction (PCR) test with encouraging results.[4],[5] These studies have mainly focused on IS6110 sequence of mycobacterial genome and partly on 38 kDa protein antigen b (Pab), and 65 kDa antigen encoding gene.[4],[5] The present study was carried out targeting the 165bp gene coding for 65 kDa antigen (cell wall protein A) which is specific for M.tuberculosis.[6] The study aimed at evaluation of the 65kDa antigen based PCR test in specimens obtained from pulmonary and extrapulmonary cases of tuberculosis with varied clinical manifestations. We also aimed to compare the results of PCR test with those of conventional ZN (Ziehl-Neelson) stained acid fast bacilli (AFB) microscopy and culture by LJ and radiometric BACTEC system. MATERIALS AND METHODS One hundred and fifty six clinical samples were obtained with a strong clinical, radiological and histopathological evidence of TB including clinical response to antitubercular treatment referred from different hospitals of Delhi like LNJP (Lok Nayak Jai Prakash), GTB (Guru Teg Bahadur), KSC (Kalawati Saran Children), AAA (Aruna Asaf Ali) hospitals in the year 2003. These criteria were used as gold standard for classifying cases of TB. All the necessary clinical details were obtained from the referring hospital in the prescribed format provided by us. Clinical specimens Clinical specimens were selected based on the clinical manifestations presented by the patient. The samples included 56 sputum samples from adult pulmonary TB cases, 16 BAL (broncho alveolar lavage) from children with pulmonary tuberculosis, 20 skin biopsies from skin TB cases, 17 synovial fluid and synovial tissue from osteoarticular TB, 6 urine (UTI), 26 pus, 1 pleural fluid, 3 lymph node aspirates, 1 bone marrow aspirate, 1 ascitic fluid, 3 other biopsies, 3 CSF, 1 endometrial biopsy, 1 menstrual blood, and 1 semen. In addition, 37 sputum samples obtained from nontuberculous individuals (chronic asthmatics, chain smokers) initially screened by AFB smear examination and chest X-ray were also used in the study as negative controls. Processing of Samples For every clinical sample, two smears, one direct and other concentrated after processing by N-acetyl-L-cysteine NaOH (NALC - NaOH) method and other appropriate methods depending on the nature of samples were prepared. Ziehl - Neelsen (ZN) staining was done on these smears using standard techniques. Deposits obtained after processing of sample were inoculated into two bottles of LJ medium and one BACTEC 12B vial.[7] One LJ medium bottle was incubated at room temperature and other at 37°C. BACTEC vials were kept at 37°C only. In case of conventional LJ media based cultures, readings were taken on a weekly basis till eight weeks, whereas in case of BACTEC cultures, for first week, bottles were read every day and thereafter at weekly intervals for six weeks.[8] Biochemical test The mycobacterial isolates obtained were subjected to niacin and NAP test for speciation of mycobacteria.[7],[9] Polymerase chain reaction Sample preparation for DNA extraction Different methods were employed for extraction of DNA from different clinical samples. Samples of sputum, pus, BAL and pleural fluid were treated with NALC-NaOH method for the decontamination and liquefaction to obtain the pellet for DNA extraction.[7] Synovial tissue was ground in a preautoclaved mortar and pestle whereas synovial fluids were used as such. Skin, lymph node and other biopsy material were ground in a mortar and pestle. In all cases, one millilitre of sample was used for DNA extraction. Urine was pelleted for DNA extraction by centrifugation at 3000g for 20 minutes. DNA extraction and amplification of the 65 kDa gene (165 bp) of M.tuberculosis. DNA was extracted using commercially available QIAmp DNA kit (QIAGEN) with one initial additional step. The preliminary processed materials, as described above, were kept at 80°C for 10 minutes for inactivation of possible mycobacteria. The material was then further processed as per the guidelines of the manufacturer of the kit to obtain the DNA. A 165bp region of the 65kDa antigen coding gene of M.tuberculosis was chosen as the primer target for DNA amplification.[6],[10] The sequence of the two primers used were: forward primer: 5′ CTA GGT CGG GAC GGT GAG GCC AGG 3′ (91-114); reverse primer: 5′ CAT TGC GAA GTG ATT CCT CCG GAT 3′ (254-231). DNA amplification by PCR was performed with a total reaction volume of 25μL by using a model PCR system 2700 thermal cycler (Applied Biosystems). The amplification reaction contained the forward and reverse primers at final concentrations of 0.01 and 1mM, respectively, 2.5 U of Taq polymerase (Perkin Elmer) in amplification buffer, 200μM (each) of the four deoxyribonucleoside triphosphate and 5μL of DNA. Positive control DNA from H37Rv strain of M.tuberculosis and negative control (water) were also used for amplification. The temperature of the reaction mixture was first raised to 95°C for 120 seconds, and 72°C for 40 seconds were given to extend the DNA chain. After final extension, the samples were immediately processed or kept at -20°C till tested. PCR products were detected on 1.5% agarose gel in 0.5 X TBE buffer containing ethidium bromide at 10μg/mL concentration. Samples showing the presence of 165bp band under ultraviolet transillumination were considered positive for the presence of M.tuberculosis [Figure - 1]. Statistical analysis The difference between sensitivity and sensitivity rates for various clinical samples by different tests were compared using the chi square test with Yates correction. RESULTS Initially, 156 clinical samples with strong clinical suspicion of tuberculosis were subjected to all the tests mentioned. Out of these 11 samples, four samples were also found to be contaminated in BACTEC culture (2%). Accordingly, in this study, we compared the results of 145 samples. In addition, 37 sputum samples obtained from nontuberculous patients were subjected to these tests. The results are given in [Table - 1] and [Table - 2]. The results show that ZN smear examination has a sensitivity of 33.79% and a specificity of 100%. For LJ media culture, sensitivity was 48.9% and specificity was 100%. BACTEC culture showed a sensitivity of 55.86% and a specificity of 100%. In comparison PCR test was found to have a much higher sensitivity of 74.4% and a specificity of 97.29% [Table - 1], [Table - 2]. All the culture isolates obtained were confirmed as mycobacteria with the biochemical tests mentioned. We also tried to compare the sensitivity of PCR test vis à vis three different tests i.e., smear examination, L-J culture and BACTEC culture result individually as well as in combination [Table - 3]. As is evident, the PCR test was found to be much more sensitive than smear examination, LJ culture or BACTEC culture (p<0.05). The sensitivity of detection of M.tuberculosis in AFB smear positive samples by PCR approached 100%, whereas that in smear negative specimens had a sensitivity of 62.5%. A sensitivity of 98.59% was observed for detection of M.tuberculosis in clinical samples which were found positive in LJ media culture. Similarly, a 97.53% sensitivity rate was observed by PCR test in clinical samples which were positive by BACTEC culture. PCR showed a sensitivity of 98.33% for the clinical samples which were positive for M.tuberculosis by both the culture methods used. PCR also showed 100% sensitivity for clinical samples which were positive by all the other three methods used (ZN, LJ and BACTEC). In 43 samples negative by all the other three tests used, PCR test was able to detect nine positives (20.93%) and these were not likely to represent false positive result as PCR repeatedly was positive on these samples and these samples belonged to highly suspected cases of tuberculosis who responded to the antitubercular treatment [Table - 3]. The mean detection time for M.tuberculosis was 24.03 days by LJ media culture, 12.89 days by BACTEC and less than one day by PCR test. The ensitivities of PCR test as well as BACTEC culture method were found to be near similar in both pulmonary and extrapulmonary tuberculosis, though, smear sensitivity was found to be much higher in pulmonary TB compared to extrapulmonary TB. Even LJ media based culture gave a higher sensitivity in pulmonary TB cases compared to extrapulmonary samples [Table - 4]. DISCUSSION The specificity, sensitivity and speed of PCR test in diagnosis of M.tuberculosis infection shown in this study should encourage the use of this method in routine diagnosis of TB. We compared the performance of various tests in different clinical samples for diagnosis of TB. PCR showed the highest sensitivity as compared to other tests as reported by others.[4] With the use of PCR test, we were able to detect M.tuberculosis in 97.87% smear negative samples which were positive by either of the culture methods. PCR test detected M.tuberculosis in less than one day, compared to average 24.03 days required for detection by conventional (LJ) and 12.89 days by radiometric BACTEC technique, as supported by earlier studies.[11] In a few samples, ZN smear examination and PCR results were positive but culture was negative; this could be due to the presence of nonviable mycobacteria in the samples as some of the subjects were receiving antitubercular treatment. The two samples of sputum and synovial fluid where AFB smear and PCR were negative but culture was positive could be due to presence of PCR inhibiting substances in the samples and low bacterial load as supported by earlier studies.[12] There was only one false positive result by PCR test which could be due to the ability of the PCR test to detect very low number and even dead bacteria in a sample which can be present in a symptomatic individual.[12] PCR test was also shown to be reasonably sensitive (75.9%) in diagnosis of extrapulmonary TB.[13],[14],[15] To conclude, molecular diagnosis of tuberculosis by PCR has a great potential to improve the clinicians′ ability to diagnose tuberculosis. This will ensure early treatment to patients and prevent further transmission of disease.[13] However, further work is needed for improving sensitivity, specificity and reproducibility of this test and to make it more user friendly and cost effective. REFERENCES
Copyright 2005 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb05006t1.jpg] [mb05006t4.jpg] [mb05006t2.jpg] [mb05006f1.jpg] [mb05006t3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}