 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
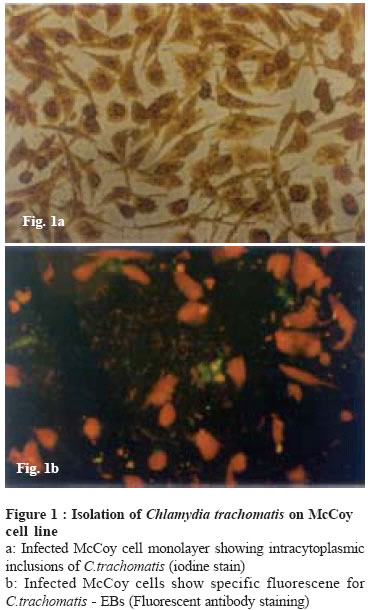
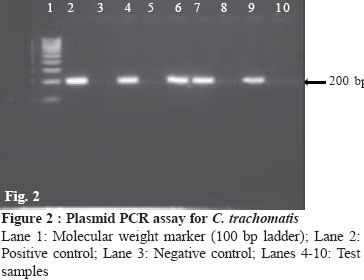
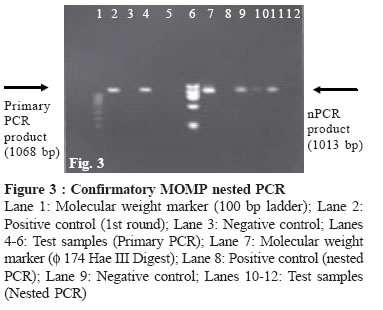
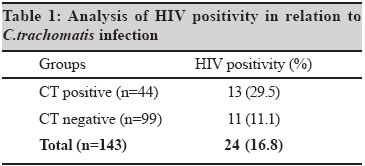
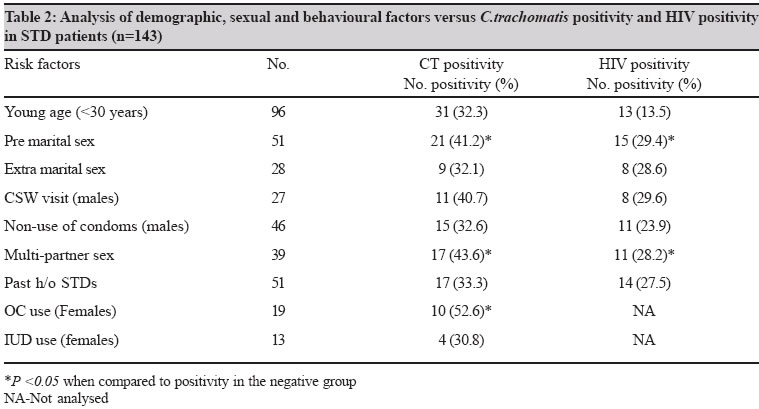
Indian Journal of Medical Microbiology, Vol. 23, No. 1, January-March, 2005, pp. 37-40 Brief Communication Genital chlamydial infection in STD patients: Its relation to HIV infection Joyee AG, Thyagarajan SP, Reddy EV, Venkatesan C, Ganapathy M Department of Microbiology, Dr. ALM PGIBMS, University of Madras, Taramani, Chennai - 600 113, Tamil Nadu Code Number: mb05008 ABSTRACT In the present report, we have analysed C.trachomatis infection and HIV positivity among patients (n-143) who attended the STD clinic at the Institute of STDs, Government General Hospital, Chennai. HIV positivity rate was significantly high among those with chlamydial infection than in those without chlamydial infection (29.5% (13/44) vs. 11.1% (11/99); p<0.05). The results of the present study suggest the association between C.trachomatis and HIV infections and reinforce the need for routine screening for C.trachomatis as a necessary intervention to reduce the burden of chlamydial diseases and to reduce the risk of HIV and its spread in India.Key words: C.trachomatis, HIV Genital infection due to Chlamydia trachomatis (CT) is currently the most prevalent among the bacterial STDs.[1] C.trachomatis infection, if undiagnosed and untreated, can result in pelvic inflammatory disease (PID), epidydimitis etc., finally damaging the human reproductive tract irreversibly. The health costs due to the destructive clinical sequelae caused by C.trachomatis infection is enormous. Further to this, growing evidence points that active C.trachomatis infection is an important risk factor facilitating sexual transmission of HIV infection.[2],[3] Hence, documentation of C.trachomatis infections in high-risk populations can assist in designing HIV-risk reduction strategies as well. In this report, we have analysed the infection rates of genital chlamydial infection and HIV infection and the possible association between the two infections. MATERIALS AND METHODS Symptomatic men and women patients (n=143) attending the STD out patient clinic at the Institute of STDs, Government General hospital, Chennai, were enrolled in the study during the period of September 1998 to August 2000. The study was approved by the Ethics committee of Govt. General Hospital. A written informed consent was obtained from each patient and detailed history, demographical and clinical features were recorded. Blood samples and genital swab specimens were obtained from each patient. Urethral and endocervical swabs were collected from males and females respectively, placed in 0.2M sucrose phosphate (2SP) transport medium and were used for both chlamydial culture and PCR assays. The serum samples were subjected for the detection of IgG specific antibodies to C.trachomatis by using a commercial immunoperoxidase assay kit (IPAzyme Chlamydia, Savyon diagnostics, Israel). Culture for C.trachomatis was performed on cycloheximide treated McCoy cells. Aliquots of 2SP specimens were tested initially by a plasmid PCR assay and further confirmed by a nested major outer membrane protein (MOMP) PCR assay. The culture and PCR methods were described in detail in our earlier report.[4] A patient was considered as ′truly infected′ for C.trachomatis if positive for culture and/or if the MOMP PCR confirmed the initial plasmid PCR positive results.[4] Anti-HIV ELISA Detection of antibodies to HIV in the patients sera was done by using commercial ELISA kits. The initial screening was done using HIV CheX ELISA, Xyton Diagnostics, India and the positive results were counterchecked by another ELISA kit, Genelavia Mixt (Sanofi Pasteur, France). Statistical methods The data analysis was performed by using statistical softwares PSSS for windows version 8.0 and Epi Info version 6.04.[5] RESULTS C.trachomatis was isolated from 27 (18.9%) cases. Out of the 46 initial plasmid PCR positive cases, 44 cases were reconfirmed by MOMP PCR.[4] Based on an ′expanded spectrum of positivity′ which included culture [Figure - 1] and PCR assays [Figure - 2], [Figure - 3], 44 (30.8%) patients were considered as ′truly infected′ for C.trachomatis and thus the prevalence of confirmed C.trachomatis infection was 30.8%. It was observed that 84 (54.7%) patients had the presence of IgG specific antibodies to C.trachomatis. HIV positivity rate was significantly higher in men than in women [(27% (17/63) vs.8.8% (7/80); P<0.05)]. C.trachomatis positivity was analysed in relation to HIV seropositivity. This showed that 29.5% (13/44) of the C.trachomatis infected cases had HIV co-infection. The study revealed [Table - 1] that HIV positivity rate was significantly high (13/44, 29.5%) among those with chlamydial infection than in those without chlamydial infection (11/99, 11.1%). The difference was statistically significant (P<0.05). Similarly, the analaysis also revealed that C.trachomatis positivity was significantly higher in the HIV positive cases than in the HIV negative cases (13/24, 54.2% vs.31/119, 26.1%; P<0.05). The serological results showed that 17 (70.8%) of the HIV positive patients had the presence of IgG antibodies to C.trachomatis, which suggested previous exposure in these cases. Notably, 11 (84.6%) of the 13 Chlamydia and HIV coinfected cases had anti-chlamydia IgG positivity. Demographic, sexual and behavioural risk factors were analysed in relation to C.trachomatis infection and HIV positivity [Table - 2]. The analysis revealed that C.trachomatis infection was significantly associated with risk factors like premarital sex, sex with multiple partners and use of oral contraceptives (OC) in women. HIV positivity also showed significant correlation to premarital sex as well as multiple sexual partners in this study population. DISCUSSION Recent studies suggest that C.trachomatis. infection of the lower genital tract may facilitate the transmission of HIV.[6] The high rate of C.trachomatis infection in STD patients observed in the present study assumes significance in view of risk of HIV transmission and spread. It was observed that HIV positivity significantly correlated to C.trachomatis infection. Our data suggests the association between HIV and C.trachomatis infections. The combined epidemiology of these infections may partly be due to the fact that STDs including HIV and C.trachomatis have common sexual/behavioural risk factors. In the present series of STD patients, premarital sex and sex with multiple partners were seen to be significant risk factors for both CT infection and HIV infection. However, STD patients represent a high-risk group compared to the normal population in the community and therefore, it may be appropriate to conclude that all sexual/behavioural factors could potentially interplay for the acquisition of these infections. Nevertheless, C.trachomatis infection and HIV infection have interrelationship independent of the sexually transmissible risk factors. The possible relationships between HIV infection and C.trachomatis infection are: 1) The invasive intracellular pathogenesis of C.trachomatis can cause substantial damage to the genital epithelial layer which may facilitate HIV infection,[7] (ii) immunological changes due to HIV infection may favour C.trachomatis infection.[8] The interrelationship between the two infections and mutually associated transmission pattern remain to be understood in greater detail. Epidemiological studies have linked genital chlamydial infection to an increased risk for acquisition of HIV disease.[2],[3] On the other hand, immunosuppression due to HIV may lead to more aggressive chlamydial disease conditions like PID in those who are infected with C.trachomatis.[9] Thus, early diagnosis and treatment of chlamydial infection is important to prevent HIV risk and devastating clinical consequence. Our results show that 30% of the Chlamydia infected cases had HIV infection, while the analysis also revealed that 50% of the HIV positive cases happened to be proven C.trachomatis positive cases. However, it could be speculated that C.trachomatis was prevalent prior to the HIV exposure among the STD cases, because the rate of the anti-chlamydia IgG antibody positive individuals was much higher than that of the HIV seropositive individuals (58.7% vs.18.8%) and therefore, it is not likely that the lower prevalence of HIV induced a higher prevalence of C.trachomatis. In the light of the present findings and in view of the substantial burden of HIV disease in India, it needs to be emphasized that controlling genital chlamydial infection may have positive impact in the control of HIV transmission and spread. The observations of the present study reinforce the importance of routine screening for C.trachomatis as a necessary intervention to reduce the burden of chlamydial disease and to reduce the risk of HIV and its spread. REFERENCES
Copyright 2005 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb05008t1.jpg] [mb05008f2.jpg] [mb05008f3.jpg] [mb05008t2.jpg] [mb05008f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}