 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
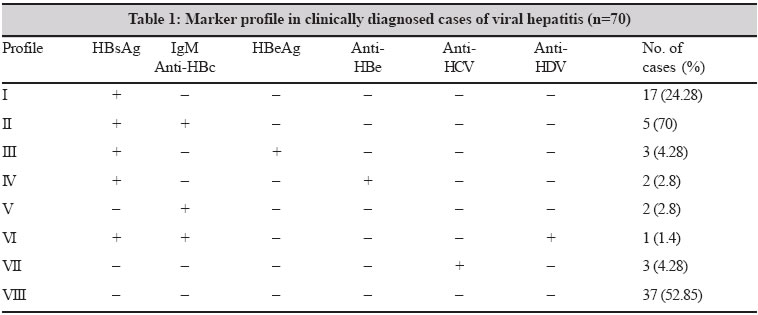
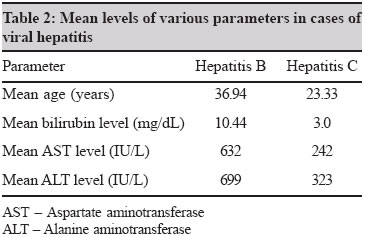
Indian Journal of Medical Microbiology, Vol. 23, No. 1, January-March, 2005, pp. 44-47 Brief Communication Prevalence of parenterally transmitted hepatitis viruses in clinically diagnosed cases of hepatitis Arora DR, Sehgal R, Gupta N, Yadav A, Mishra N, Siwach SB Department of Microbiology, Pt. B.D. Sharma Post Graduate Institute of Medical Sciences, Rohtak - 124 001, Haryana Code Number: mb05010 ABSTRACT Hepatitis B virus (HBV) is the most important causative agent of blood borne hepatitis in humans. Hepatitis D Virus (HDV) infection occurs either as a coinfection or superinfection in HBV carriers. Hepatitis C virus (HCV) is the major cause of transfusion non-A, non-B hepatitis and continues to be a major cause of human liver disease throughout the world. The present study was conducted on 70 clinically diagnosed cases of viral hepatitis to study the prevalence of parenterally transmitted viral hepatitis. The serum samples were tested for HBsAg, HBeAg, IgM anti-HBc, anti-HBe, anti-HCV and anti-HDV using separate ELISA kits. Of the 70 serum samples tested, 28(40%) were positive for HBsAg out of which 3 (4.28%) were positive for HBeAg also. Five (7.1%) of the HBsAg positive cases tested positive for IgM anti-HBc also. HBsAg alone was found in 17(24.28%) cases. The prevalence of anti-HCV was 3 (4.28%) in 70 cases. Thus early screening of clinically diagnosed cases of viral hepatitis is essential for establishing diagnosis and treatment to prevent long term sequelae.Key words: Viral hepatitis, Hepatitis B, Hepatitis C, Hepatitis D Hepatitis B virus (HBV) is the most important causative agent of blood borne hepatitis in humans. HBV is responsible for approximately 300 million cases of chronic infection worldwide.[1] The national average for HBsAg positivity in the healthy donor population in India is around 4.7%. With a population base of 900 million, the total HBV carrier pool in India is around 43 million.[2] The risk of transmission of HBV from HBsAg undetectable blood transfusion is one in 178 (0.6%). Indian data on transfusion - associated as well as sporadic hepatitis B are limited.[3] HDV infection occurs either as a coinfection or superinfection in HBV carriers. Intravenous drug abusers and patients receiving multiple transfusions of blood products are at high risk of developing HDV infection.[4] Very little is known about the prevalence of HDV in the Indian population. Prevalence of HDV in HBsAg carriers varies from 1 to 5% in the US, Western Europe and Asia. HDV prevalence varies from 0 to 7% in asymptomatic HBsAg carriers.[5] Hepatitis C virus (HCV) is the major cause of transfusion associated non-A, non-B hepatitis and continues to be a major cause of human liver disease throughout the world. The prevalence of HCV around the world ranges from 0.4 to 2%. Hepatitis C is gradually being recognised as a major health problem even in developing countries. Among Indian blood donors, the seroprevalence varies from 0.48% in Vellore[6] to 1.85% in New Delhi.[7] Paucity of data on prevalence of parenterally transmitted hepatitis viruses from our area prompted us to study the various viral markers in clinically diagnosed cases of viral hepatitis, so that early diagnosis can help us in treatment and prevention of longterm sequelae. MATERIALS AND METHODS A total of 70 serum samples were included in the study. These comprised of cases diagnosed clinically as those of viral hepatitis, and supported by evidence of raised levels (5 to 100 fold) of two critical liver function enzymes, aspartate aminotransferase (AST) and alanine aminotransferase (ALT) with or without icterus. All subjects with known non infectious hepatitis were excluded from the study. Hepatitis A and Hepatitis E cases were also excluded from the study group. Detailed history of the patients was recorded in a questionnaire which had several questions related to social background, drug abuse, sexual risk behaviour and blood transfusion. For detecting the presence of viral hepatitis markers, 5mL of blood was withdrawn from each patient aseptically taking adequate precautions and consent. Serum was separated and preserved at -20°C. Serum samples were tested for HBsAg, HBeAg, IgM anti-HBc, anti-HBe, anti-HCV and anti-HDV using separate ELISA kits: "Monolisa AgHBs", "Monolisa HBe" and "Monolisa HBeIgM" (obtained from Sanofi Diagnostics), "Murex anti-HCV" (Murex Diagnostics) and "Hepanostika HDV" (Organon Teknika). The methodology and technique detailed in the information inserts provided with these kits were strictly adhered to. RESULTS Of the 70 serum samples tested, 28 (40%) were positive for HBsAg, out of which 3 (4.28%) were positive for HBeAg also. Five (7.1%) of the HBsAg positive cases tested positive for IgM anti-HBc also. There were 2 (2.85%) cases in which IgM anti-HBc was the only serological marker present. Two (2.85%) cases were positive for HBsAg and anti-HBe markers. HBsAg alone was found in 17 (24.28%) cases. Only a single HBsAg positive sample tested positive for anti-HDV antibody. The IgM Anti-HCV antibodies were detected in 3 (4.26%) out of 70 cases. There was no case of coinfection with HBV and HCV [Table - 1]. The mean age at presentation of hepatitis B cases was 36 years and that for hepatitis C cases was 23 years. All cases of HCV infection were males while the male:female ratio for HBV cases was 1.7:1. The mean bilirubin levels among HBV and HCV infected cases were 10.44 mg/dL and 3.0 mg/dL respectively. The mean AST and ALT levels in HBV cases were 632 IU/L and 699 IU/L respectively, while the figures for HCV cases were 242 IU/L and 323 IU/L respectively [Table - 2]. All cases of HCV infection were anicteric while 24 (85%) of 28 cases of HBV infection were icteric. An attempt was made to know the probable mode of acquisition of viral infection. Adequate history could be obtained only in 28 cases of hepatitis B infection, out of which mode of acquisition of infections could be ascertained only in 17 cases, blood transfusion was the route in 4 (23.5%), sexual contact in 2 (11.7%) surgery in 6 (35.2%) and parenteral medications in 5 (29.4%) cases of Hepatitis B. DISCUSSION HBV and HCV infections are among the most prevalent infectious diseases in humans worldwide. Both infections are associated with a broad range of clinical presentations ranging from acute or fulminant hepatitis to chronic infection that may be clinically asymptomatic or may progress to chronic hepatitis and liver cirrhosis. HBV infection has several modes of transmission of which perinatal transmission and transfusion of infected blood and blood products are most important. Other important modes include sexual transmission, tattooing, needle stick exposure etc.[8] The prevalence of HBsAg positivity in different populations ranges from less than 0.5% to as high as 20%. A study conducted in Aurangabad reported 6.42% carriage in resident doctors.[9] Another study conducted in Delhi reported 6.9% transfusion associated hepatitis (TAH) among patients receiving blood transfusion for cardiac surgery; of the total TAH cases 20% were related to HBV.[3] However, in our study, conducted on clinically diagnosed viral hepatitis, 28 (40%) cases were HBsAg positive of which eight cases were acute HBV infections indicated by presence of IgM anti HBC or HBeAg. Another two HBsAg and anti-HBe positive cases showed remote HBV infections with low infectivity. The remaining 17 cases which were only HBsAg positive, however, suffered from severe hepatitis and showed very high levels of ALT and AST which could be due to atypical/mutant serotype HBV forms which have been implicated in producing severe hepatitis. In a study conducted in New Delhi 25.8% of 120 serologically characterized and histologically proven hepatitis B related chronic liver disease patients were infected with either precore or surface mutant form.[10] However, detection of HBV DNA by amplification technique can serve as an important tool in such clinical setting. Other researches have shown the presence of HBV DNA in cases where HBeAg was negative and liver function tests were abnormal.[11] But detection of HBV DNA was not possible in our hospital setting due to our constraints. Prevalence of HDV in HBsAg carriers varies from 1 to 5% in US, Western Europe and Asia.[5] HDV prevalence varies from 0 to 7% in asymptomatic HBsAg carriers.[5] The prevalence of HDV infection among blood donors positive for HBsAg is low (1.4 to 8%) but is quite high in those with repeated exposures such as intravenous drug abusers (20 to 30%) and haemophiliacs (48 to 80%). Co-infection of HBV-HDV is associated with a higher incidence of fulminant hepatic failure than is observed in primary HBV alone.[12] Our study also showed only a single case of fulminant hepatic failure which was positive for IgM anti-HDV, HBsAg and IgM anti-HBc. One group of researchers have reported that 20% of patients with HBV infection have associated HDV infection while others have reported 13.2% prevalence of HDV infection in HBsAg positive cases.[13] Very little data is available regarding HBV-HDV coinfection in our region and requires further evaluation. Hepatitis C virus is a major cause of liver disease throughout the world ranging from acute and chronic hepatitis to cirrhosis and hepatocellular carcinoma. About 0.04 to 26% of apparently healthy population in different countries of the world is suffering from chronic HCV infection. The parenteral route of HCV transmission is responsible for almost two third of hepatitis C cases while nonparenteral routes of transmission are perinatal and sexual routes. Prevalence is higher in high risk groups, thalassemics, haemodialysis patients, health care workers and IV drug abusers.[14] Depending upon the type of the test used for screening and confirmation, less than 0.2 to 4% of donors were found to be anti HCV positive.[15] In our study of 70 clinically diagnosed viral hepatitis cases only 3 (4.28%) were positive for IgM anti-HCV antibodies. Our results are in concordance with another study done in south India in which cases of hepatitis were analysed for hepatitis A to E viruses and hepatitis C was found in 3% cases. Seroprevalence of 0.5 to 2.5% using 2nd generation EIA[16] and 4.8% in hospital based general population using 3rd generation EIA[17] has been reported from India. Prevalence of 8.33% HCV infection among patients of chronic active hepatitis and cirrhosis has been reported from Calcutta.[18] Most of hepatitis C cases (70 to 80%) progress to chronic infection. In our study, no case of co-infection of HBV and HCV was detected. However, dual infection has been reported in 12% cases of chronic liver disease and 11.7% cases of hepatocellular carcinoma from India.[2] These findings are in contrast to our study probably because these studies comprised of proven cases of chronic liver disease and hepatocellular carcinoma whereas the cases in our study were included on the criterion of raised liver function enzymes and exclusion of other causes of hepatitis such as alcoholism and drug toxicity. The mean bilirubin level among hepatitis B cases was 10.44 mg/dL compared to 3.0 mg/dL in hepatitis C cases. Mean AST and ALT levels in hepatitis B cases were almost twice those in hepatitis C cases. This is in concordance with the fact that enzyme levels in most cases of hepatitis C are only moderately elevated, fluctuating and sometimes normal.[15] Most common symptoms in case of hepatitis B and C were anorexia, malaise and bodyache. On clinical examination 60% cases of hepatitis B had hepatomegaly and 80% had icterus. All cases of hepatitis C had hepatomegaly while none was icteric. These findings correlate with high bilirubin levels in hepatitis B cases and near normal levels in hepatitis C cases. On the basis of clinical data the mode of acquiring infection could only be ascertained in only 17 (51.5%) cases. Of which previous surgical intervention and intravenous drug abuse was most common. In 5 (15.1%) cases, the proper history could not be obtained as they were outdoor patients or could not adequately recall and report past history of invasive treatment or nature of medication. Thus in 11 cases (33.3%) no possible route of transmission of HBV and HCV could be elucidated. Similarly no history for possible route of transmission could be obtained in 52% cases in Delhi.[19] In summary, this preliminary study shows that early screening of clinically diagnosed cases of viral hepatitis for Hepatitis, B, C and D is an essential step for establishing diagnosis and initiating treatment so as to prevent the long term sequalae viz., chronic active hepatitis, cirrhosis and hepatocellular carcinoma. REFERENCES
Copyright 2005 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb05010t1.jpg] [mb05010t2.jpg] |
| |||||||||
{kind=link}
{kind=link}