 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
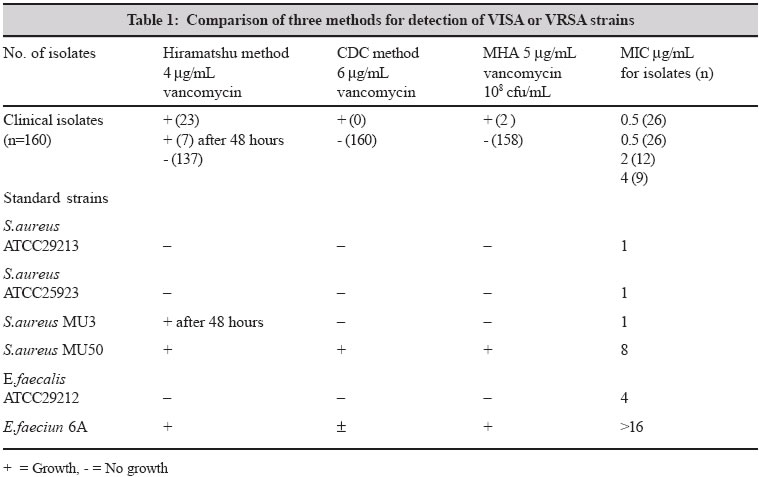
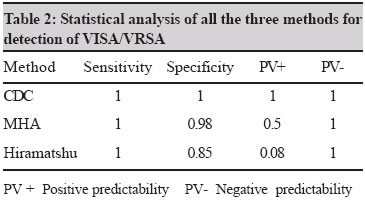
Indian Journal of Medical Microbiology, Vol. 23, No. 1, January-March, 2005, pp. 52-55 Brief Communication Detection of vancomycin resistant Staphylococcus aureus: A comparative study of three different phenotypic screening methods Bhateja P, Mathur T, Pandya M, Fatma T, Rattan Ashok Department of Microbiology, Ranbaxy Research Laboratories, R&D II, Sector 18, Udyog Vihar Industrial Area, Gurgaon-122 001, Haryana Code Number: mb05012 ABSTRACT The objective of this study was to investigate screening methodologies, to detect Staphylococcus aureus strains with decreased susceptibility to vancomycin. Three methods were used to screen 160 Staphylococcus aureus clinical isolates along with ATCC quality control strains. Subsequently, MIC of all these 160 strains were determined by NCCLS methodology. The MIC of all the 160 clinical isolates was < 4µg/mL and were classified as vancomycin susceptible by NCCLS criteria but 23 strains were positive by Hiramatshu method, two grew on MHA (5µg/mL vancomycin) while CDC method correctly identified no vancomycin intermediate S.aureus (VISA) or vancomycin resistant S.aureus (VRSA) strains with reference to there MIC. CDC method was found to be the most appropriate screening methodology for detection of VISA or VRSA for diagnostic laboratories.Key words: VRSA,VISA, MIC, screening, glycopeptide. Staphylococcus aureus is a major cause of hospital acquired infections, causing high morbidity and mortality throughout the world. The proportion of MRSA has risen worldwide during the last two decades. The recommended treatment for multiresistant MRSA are glycopeptides, particularly vancomycin.[1] Since the emergence of vancomycin resistance in enterococci in 1988 and its in vitro demonstration that its resistance genes (Van A and Van B) are transmissible to other bacterial species including S.aureus, emergence of vancomycin resistance in clinical staphylococci has become a great concern.[2] Clinicians are continually being challenged by infections caused by S.aureus. Not only is S.aureus a major cause of both community acquired and health care associated infections, but the treatment of suspected S.aureus infections is becoming increasingly more complicated.[3] Low level vancomycin resistance in coagulase negative staphylococci has been reported. In 1997 the first strain MU 3[1] with reduced susceptibility to vancomycin and teicoplanin followed by MU 50[1] were reported from Japan. Soon thereafter a report of two additional cases from the United States was published.[4] Recently there have been further reports of VRSA and hetero VRSA (hVRSA) from France, Spain and UK.[5] Vancomycin resistance in S.aureus is difficult to define mainly because of methodological problems in their detection.[6] VRSA strain MU 50 has MIC of 8µg/mL and strain MU 3 with heterogeneous resistance has MIC of 2µg/mL.[7] As per National Committee for Clinical Laboratory Standards (NCCLS) staphylococci with MIC of vancomycin < 4µg/mL is susceptible, while for which the MIC is 8-16µg/mL are intermediate and those with MIC > 32µg/mL are resistant.[4] VISA isolates are not reliably distinguished from vancomycin susceptible isolates by rapid automated methods such as Microscan. NCCLS disk diffusion method and the stokes method are not accurate predictors of reduced vancomycin susceptibility in S.aureus.[4] A screening strategy has been suggested to rapidly detect VISA or VRSA strains in a clinical laboratory.[5] We have investigated 160 recent isolates of S.aureus simultaneously by three methodologies and determined MIC using NCCLS methodology, in order to determine the most suitable screening method. MATERIALS AND METHODS Bacteria Clinical isolates of S.aureus (n=160), collected from tertiary care centers during microbial in vitro susceptibility testing were taken for the study, 13 isolates were MSSA and 147 were MRSA. In addition, S.aureus ATCC 29213, S.aureus ATCC 25923 (vancomycin susceptible), S.aureus MU3 and MU50 (Japan), E.faecalis ATCC 29212 (vancomycin susceptible) and E.faecium 6A (vancomycin resistant) were included as quality control strains (QC). Screening methods Screening of VRSA strains was performed by following methods. Hiramatshu method: Overnight grown cultures were adjusted to 0.5 McFarland approximately 1.5x108 cfu/mL and 10 L spot was inoculated on BHI agar containing 4µg/mL of vancomycin (Eli Lilly). The plates were incubated at 35°C for 24-48 hours.[1] CDC method: Overnight grown cultures were adjusted to 0.5 McFarland approximately 1.5x108 cfu/mL and diluted 100 times to get an inoculum of approximately 1.5x 106 cfu/mL. Spots 10μL of the cultures were inoculated on BHI agar containing 6µg/mL of vancomycin. The plates were incubated at 35°C for 24-48 hours.[4] Method by Tenover et al: Overnight grown cultures were adjusted to 0.5 Mcfarland approximately 1.5x108 cfu/mL and diluted 100 times to get an inoculum of approximately 1.5x 106. Spot 10 L of both the inoculum levels were inoculated on MHA agar (Difco) containing 5 g/mL of vancomycin. The plates were incubated at 35°C for 24-48 hours.[5] Vancomycin MICs for the clinical isolates were determined by agar dilution method in Mueller Hinton agar according to the protocol of National Committee for Clinical Laboratory Standards (NCCLS).[8] RESULTS All the QC strains included in the study indicated their previously described phenotype. All the 160 clinical isolates showed MIC of < 4µg/mL, amongst them 9 had vancomycin MIC of 4µg/mL and would therefore still be classified as vancomycin susceptible by NCCLS criteria. In the three screening methods, CDC method (6µg/mL vancomycin) correctly identified no VRSA strains. In the next method two strains grew on MHA (5µg/mL vancomycin). In Hiramatshu method as many as 23 strains grew on 4µg/mL vancomycin plates and seven amongst them were positive after 48 hours of incubation as shown in [Table - 1]. These strains would be considered as hetero VRSA (hVRSA). According to statistical analysis CDC proved to be the most sensitive and specific method showing positive and negative predictability as 1. In MHA (5µg/mL vancomycin) the sensitivity and the positive predictability is 1 and 0.5 respectively while Hiramatshu has positive predictability of 0.08 only as shown in [Table - 2]. DISCUSSION Isolates of vancomycin resistant S.aureus have emerged in many parts of the world. These isolates appear to achieve clinically relevant levels of resistance to vancomycin that leads to treatment failure. At present, the proportion of MRSA with reduced susceptibility to vancomycin is well known. Only 21 strains have so far been reported in literature. The first VRSA and hVRSA reported from Japan were MU 50 and MU 3, respectively.[7] The methods proposed for detection of hVRSA by Hiramatshu et al[9] is similar to the method used by Daum et al[10] to select S.aureus resistant to vancomycin. It remains unclear whether this method detects vancomycin resistance or selects for it.[11] Vancomycin resistance can be difficult to detect in clinical microbiology laboratory. Disk diffusion sensitivity testing by standard 30µg vancomycin frequently misclassifies intermediately susceptible isolates as fully susceptible. Presently MIC determinations by broth or agar dilution or by E test are the gold standard for determining vancomycin susceptibility,[6] but these methods are not suitable for routine use in the diagnostic laboratories. CDC has adopted three criteria to identify VISA strains: Broth microdilution vancomycin MIC of 8-16µg/mL, E test vancomycin MIC of > 6µg/mL and growth on BHI agar containing 6µg/mL vancomycin within 24 hours. MU3, the hVRSA strain does not grow on this medium therefore Hiramatshu et al suggest using BHI agar with 4µg/mL vancomycin. Bierbaum et.al [12] reported that 23 of 25 isolates showing growth on this medium were susceptible by NCCLS criteria.[4] According to Tenover et al[4] growth of number of S.aureus strains on 4µg/mL vancomycin containing agar did not have elevated MICs. In agreement with the above reports the present study showed that 23 of 160 strains growing on 4µg/mL vancomycin plates were infact susceptible by NCCLS criteria. Hiramatshu method is probably an inappropriate means of screening for detection of VRSA owing to high number of false positives. We would recommend that diagnostic laboratories screen their S. aureus isolates by the CDC method and submit strains growing on these plates to reference laboratories for confirmation of vancomycin resistance by determining the MIC. Clinicians should continue to exercise caution in their use of vancomycin in order to preserve this useful antibiotic and prolong its therapeutic usefulness. REFERENCES
Copyright 2005 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb05012t2.jpg] [mb05012t1.jpg] |
| |||||||||
{kind=link}
{kind=link}