 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
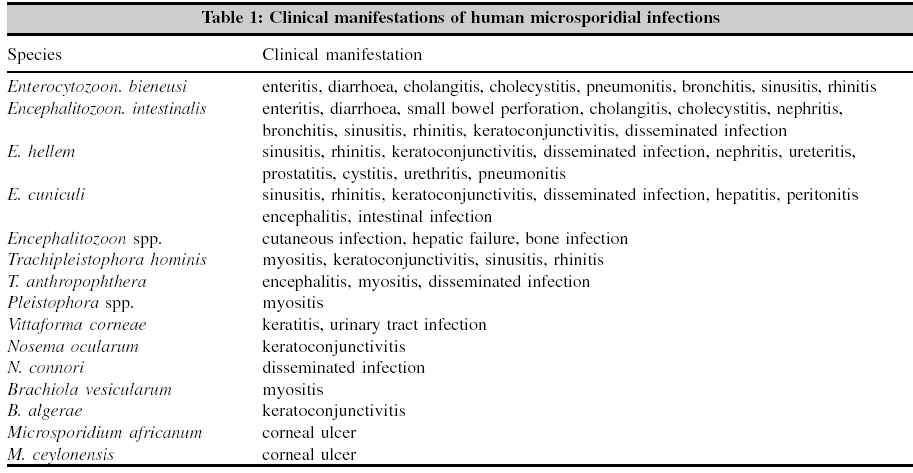
Indian Journal of Medical Microbiology, Vol. 23, No. 2, April-June, 2005, pp. 80-91 Review Article Microsporidia: Emerging Ocular Pathogens Joseph J., Vemuganti G.K., Sharma S. Jhaveri Microbiology Center, Hyderabad Eye Research Foundation, LV Prasad Eye Institute, LV Prasad Marg, Banjara Hills, Hyderabad Correspondence Address: Jhaveri Microbiology Center, Hyderabad Eye Research Foundation, LV Prasad Eye Institute, LV Prasad Marg, Banjara Hills, Hyderabad - 500 034, savitri@lvpei.org Code Number: mb05024 Abstract Microsporidia are eukaryotic, spore forming obligate intracellular parasites, first recognized over 100 years ago. Microsporidia are becoming increasingly recognized as infectious pathogens causing intestinal, ocular, sinus, pulmonary, muscular and renal diseases, in both immunocompetent and immunosuppressed patients. Ocular microsporidiosis, though uncommon, could be isolated or part of systemic infections. It occurs mainly in two forms: keratoconjunctivitis form, mostly seen in immunocompromised individuals; stromal keratitis form seen in immunocomptetant individuals. Recent reports indicate increasing number of cases of ocular microsporidiosis in immunocompetent individuals. The ocular cases present as superficial keratitis in AIDS patients, and these differ in presentation and clinical course from the cases seen in immunocompetent individuals which mainly appear to be as deep stromal keratitis. For most patients with infectious diseases, microbiological isolation and identification techniques offer the most rapid and specific determination of the etiologic agent, however this does not hold true for microsporidia, which are obligate intracellular parasites requiring cell culture systems for growth. Therefore, the diagnosis of microsporidiosis currently depends on morphological demonstration of the organisms themselves, either in scrapings or tissues. Although the diagnosis of microsporidiosis and identification of microsporidia by light microscopy have greatly improved during the last few years, species differentiation by these techniques is usually impossible and electron microscopy may be necessary. Immuno fluorescent-staining techniques have been developed for species differentiation of microsporidia, but the antibodies used in these procedures are available only at research laboratories at present. During the last 10 years, molecular techniques have been developed for the detection and species differentiation of microsporidia.Key words: Microsporidia, keratitis, conjunctivitis, diagnosis, AIDS Microsporidia are spore forming, small, obligate, intracellular living eukaryotes infecting a broad range of vertebrates and invertebrates. Though they were initially included in genus and species of protozoan, recent reports suggest that they resemble fungus.[1] Till date a number of species have been identified and isolated from various sources. Although microsporidia were discovered more than 100 years ago,[2] the first well documented case of human microsporidiosis was reported in 1959.[3] After that only ten well documented cases were described until 1985. It was only in the last decade that interest in the organism heightened because of their association with the HIV and AIDS.[4],[5] and these parasites are now recognized as one of the most opportunist pathogens in immunocompromised patients. The ability of these parasites to cause disease in immunocompetent persons is still being elucidated. Microsporidia can cause a variety of human diseases, involving multiple organ systems, which include intestinal, ocular, sinus, pulmonary, and muscular and renal diseases, in both immunocompetent as well as immunocompromised patients.[6] The first case of microsporidiosis from India was a patient with diarrhoea and was reported in 2001.[7] The ocular manifestations include superficial punctate keratoconjun-ctivitis, and corneal stromal keratitis and these two manifestations are directed by the genus involved as well as the immune status of the patient. Keratoconjunctivitis is usually seen in immunocompromized individuals or in contact lens wearers, mostly by genus Encephalitozoon while Nosema and Microsporidium cause the stromal keratitis. However, recent reports suggest that keratoconjunctivitis can also occur in immunocompetent individuals.[1] In view of the increasing number of reports from all parts of the world, it is important to update our selves with the new clinical manifestaions, latest techniques of identification and the new treatment modalities to overcome these infections. In this paper we review the epidemiology, pathogenesis, clinical manifestations, diagnosis and management of microsporidia with special emphasis on ocular microsporidiosis. Taxonomy and Classification Taxonomically, the microsporidia were grouped and classified on the basis of their natural hosts and ultrastructural features such as size of the developing and mature organisms, nucleus arrangement (monokaryon or diplokaryon), number of polar filament coils, interface with the host cell during development (e.g., direct contact with host cell cytoplasm, replication within a host-cell derived parasitophorous vacuole, replication of organisms surrounded by endoplasmic reticulum, sporogony within a parasite-generated sporophorous vesicle), and mode of cell and nuclear division (binary division, karyokinesis with delayed cytokinesis). Molecular biology methods have subsequently been used to further classify the microsporidia, and in 1986, Vossbrinck and colleagues reported that the eukaryotic microsporidia possessed prokaryote-like ribosomes because the ribosomal genes encoded 16S and 23S subunits without an independent 5.3S subunit that is typically observed in eukaryotes.[9],[10] These results suggested that the microsporidia were early-branching protozoa. Edlind and colleagues then reported that the alpha-tubulin and beta-tubulin gene sequences of the microsporidia were more closely related to those of fungi than to other protozoans.[11] Comparisons of gene sequences encoding for translation elongation factors EF-1 and EF-2 and the largest subunit of RNA polymerase II also supported a close relationship between the microsporidia and the fungi.[12] Furthermore, mitochondrial-type HSP70 gene sequences for the microsporidia, Varimorpha necatrix and Nosema locustae, were identified and found to be more closely related to HSP70 gene sequences of fungi than of protozoa.[13]-[15] These findings suggested that the microsporidia once did possess mitochondria, are related to fungi, and are eukaryotes that did not branch as early as first believed.[16] Genus and species specific characteristics There are four genera that infect humans namely: Encephalitozoon Parasites of the four genera affecting humans can be distinguished by their developmental cycle and host-parasite relationships in infected cells. Encephalitozoon cuniculi develop within host cells in vacuoles bounded by a membrane that is thought to be of host cell origin. The spores are ellipsoid and measure approximately 2.5 by 1.5 mm They have a corrugated exospore surface, a thick endospore, four to seven (usually five or six) coils of the polar tubules, and often a polar vacuole.[1],[5] Nosema Some of the structures lie in cysts bounded by membranes, but most of the parasites are in direct contact with the cytoplasm. Spores are oval, measuring approximately 4 by 2 mm. Nuclei in the diplokaryon arrangement are seen in all forms. The polar tube has about 11 coils.[1],[5] Pleistophora Organisms resembling microsporidia of the genus Pleistophora have been recognized in one human patient. The spores were oval, approximately 2.8 by 3.4 mm. Not all developmental stages were seen. The spore wall is typical for many microsporidia, having a thin electron-dense exospore layer, a thick electron-lucent endospore, and a thin internal plasmalemma. Approximately 11 cross sections of the polar tubule were recognized in spores.[1],[5 Enterocytozoon Enterocytozoon bienusi is the microsporidian parasite most commonly recognized in humans and, so far, has been detected only in enterocytes All stages are seen in direct contact with the host cell cytoplasm. Early developmental stages may have diplokaryotic nuclei but later stages display isolated nuclei. The parasites are small, approximately 2 to 4 mm in diameter, and have a simple plasma membrane during the early stages of division. Spores are approximately 1.5 by 0.5 mm in tissue section and differ from other microsporidia by having a very thin endospore layer.[1],[5] Epidemiology The first well documented case of microsporidian infection in humans was reported in 1959, in a Japanese boy exposed to farm animals who presented with headache, convulsions, and recurrent fever. Examination of the cerebrospinal fluid revealed organisms identified as microsporidia, genus Encephalitozoon .[3] The next two reports were in 1973: An immunocomprimised infant with athymic aplasia died of severe diarrhoea and malabsorption.[17] The microsporidium Nosema connori were identified in most organs. The other report was of corneal involvement in a 11-year old boy from Sri-Lanka.[18] Between 1959 and 1990, only 8 cases of human microsporidiosis had been reported in the immunocompetent or immunocompromised individuals without AIDS.[19] Four of these cases involved the eye.[18],[20],[22] Since 1985, more than 60 cases of microsporidian infections have been reported in patients with chronic diarrhoea, and AIDS.[23] Microsporidia are being increasingly recognized as opportunistic infectious agents worldwide. Cases of microsporidiosis have been reported in developed as well as in developing countries, including: Argentina, Australia, Botswana, Brazil, Canada, Czech Republic, France, Germany, India, Italy, Japan, The Netherlands, New Zealand, Spain, Sri Lanka, Sweden, Switzerland, Thailand, Uganda, United Kingdom, United States of America, and Zambia.[24] The largest amounts of data have been accumulated on severely immunocompromised, HIV-infected patients found in North America, western Europe and Australia where the prevalence ranges from 2 to 50% or higher. In addition to AIDS patients, microsporidiosis has been reported in patients who are chemically immunosuppressed after receiving organ transplants. The prevalence data for microsporidiosis among non-HIV-infected persons is limited.[25],[26]
The first well documented case of ocular involvement in humans was in 1973[18] in a 11-year old boy who was diagnosed to have stromal keratitis caused by microsporidia.. Closely following were three additional cases of deep stromal keratitis.[20]-[22] In 1990 there were several cases of superficial keratitis in AIDS patients, which differed in presentation and clinical course from the earlier cases seen in immunocompetent individuals.[1],[27],[28] These individuals had a superficial epithelial keratopathy. In India, the first case of ocular microsporidiosis was reported in 2003, in an immunocompetent individual.[29] Although fecal-oral transmission
is the likely route of infection in humans with intestinal microsporidiosis,
the source of ocular infections is not clear. The relatively superficial
location of conjunctival and corneal tissues suggests that direct inoculation
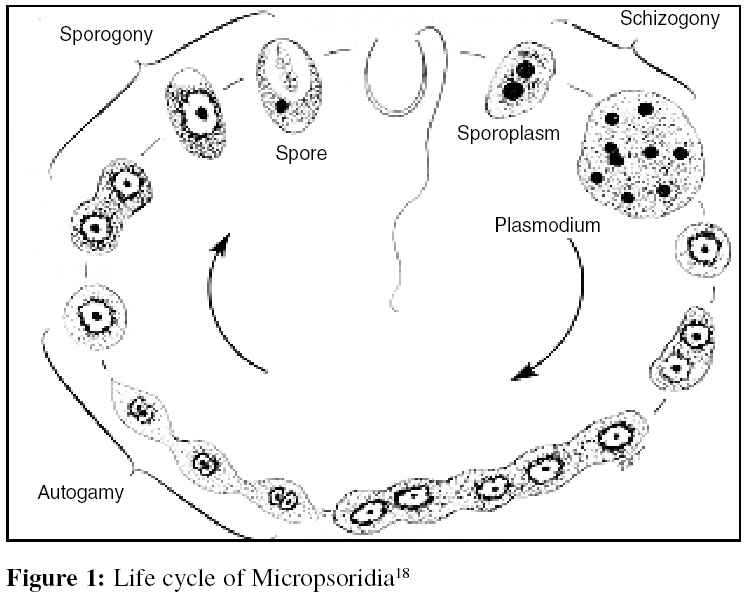
of the eye may occur.[5] In case of E. hellem and E. intestinalis there is evidence that the ocular findings are part of a systemic infection which may involve the sinuses, respiratory or gastrointestinal tract. There has been no large scale sero-epidemiological screening of AIDS patients to identify the prevalence of antibody positivity to various strains of microsporidia nor is the true number of cases, including reported and unreported cases, known.[30] The infection is by direct inoculation [Figure - 1] where the spore discharges into the host cell a polar filament through which the sporoplasm is introduced. The sporoplasm multiplies inside the host cell and develops into meronts (schizonts) and sporonts. Each sporont divides to form two sporoblasts, which, in turn, develop into spores at maturation.[31]-[35] Spores may disseminate from cell to cell inside the host or can be excreted via the skin[35] or urine. Urine to finger to eye transmission may be responsible for horizontal spread in humans.[36]
The only stage of microsporidia outside the host cell is that of infective spores. There are two distinct phases in the development of microsporidia: a proliferative phase (merogony) responsible for a massive increase in number inside the host cell and a sporogonic phase (sporogony),in which sporonts produce sporoblasts which mature into spores.[1]
The proliferative phase occurs once the sporoplasm enters a suitable host cell. The proliferative cells, referred to as meronts, develop in direct contact with the host cell cytoplasm (Nosema, Enterocytozoon ) in a parasitophorous vacuole lined by a host produced single membrane (Encephalitizoon ), in a parasite secreted amorphous coat (Pleistophora, Trachipleistophora, Thelohania ), or surrounded by endoplasmic reticulum of the host (Endoreticulatus, Vittaforma ).[37] Division occurs by binary fission or, karyokinesis occurs without cytokinesis, producing multinucleate cells called merogonial plasmodia.[1]
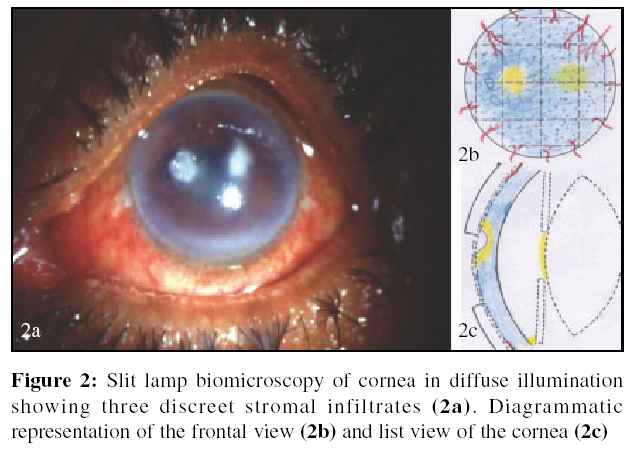
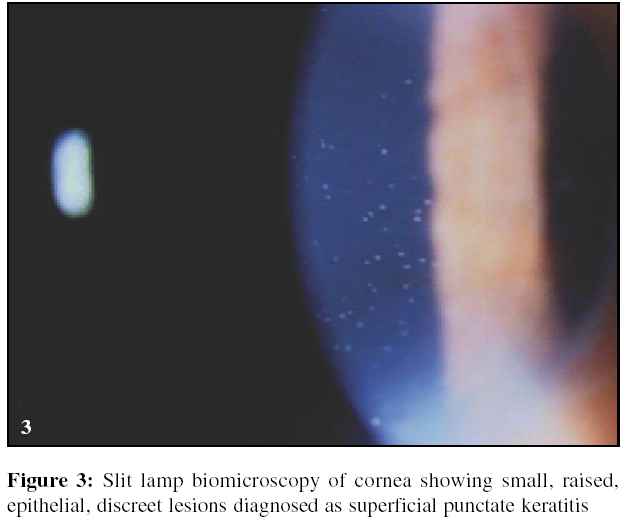
This process essentially involves conversion of meront into a sporont, the cell that produces the sporoblasts. which mature into spores.[1] The mature spores are then released to the surroundings by disruption of the cell membrane.[37] To infect their hosts, micropsoridia have developed a specific process that takes place in vitro .[9] It involves spore activation and polar tube discharge, by which the infective sporoplasm is injected into the host cell cytoplasm.[37] It is followed by immediate breakdown of sporoplasm compartmentalization, producing an increase in osmotic pressure which triggers polar tube eversion and injection of the sporoplasm into the host cell.[37] Clinical Presentation Ocular symptoms There are two clinical presentations of ocular microsporidial infections: corneal stromal keratitis [Figure 2a], [Figure 2b], [Figure 2c] and epithelial keratopathy with conjunctivitis [Figure - 3]. Deep stromal keratitides, occurring mainly in immunocompetent patients begin insidiously and mimick a progressive herpes disciform keratitis with recurrent stromal infiltration and uveitis. They have also been described to be presenting as vascularised corneal scar and perforated corneal ulcer with hyphaema, a clinical picture also mimicking herpes simplex virus (HSV) keratitis. Diagnosis can be made on corneal biopsy but penetrating keratoplasty may be necessary for visual rehabilitation.[19] Patients with deep stromal keratitis, suffer from a marked reduction in visual acuity from the infection.[19] In HIV-infected patients, keratoconjunctivitis may be caused by all three Encephalitozoon spp. (E. hellem, E. cuniculi and E. intestinalis ). Most patients present with bilateral conjunctival inflammation and also exhibit bilateral punctate epithelial keratopathy leading to decreased visual acuity. Often the keratoconjunctivitis is asymptomatic or moderate, but it can be severe, and rarely leads to corneal ulcers. Other species (V. corneae, N. ocularum, T. hominis, M. ceylonensis, M. africanum ) were reported only as single case reports.[19] Laboratory Diagnosis Diagnosis of microsporidia in general is based on the microscopic identification of the organism, the electron mircroscopic findings, nucleic acid methods and serological assays. The spores are generally resistant and can remain stable after fixing the specimens in 10% formalin. Fresh tissues can be stored in saline or culture media supplemented with antibiotics. The various samples that are tested for microsporidia include: stools, biopsy specimens, urine, sputum, bronchoalveolar lavage, nasal secretions, and cerebrospinal fluid. We describe the stains with special reference to ocular samples.
Diagnosis of ocular microsporidiosis is dependent on the identification of spores in clinical samples which include conjunctival and corneal scraping, swab or biopsy, corneal transplant button and a whole globe from an enucleation.[1],[19]
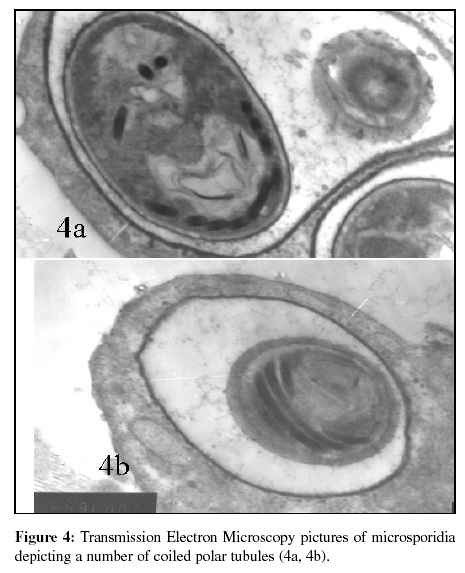
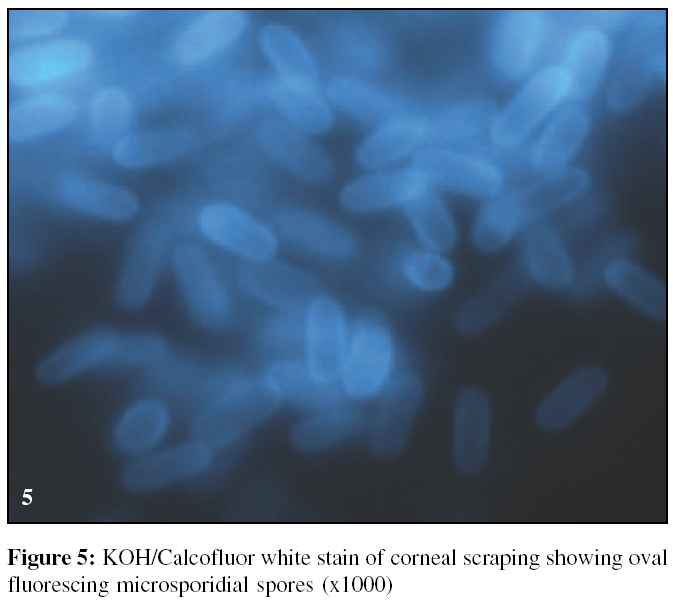
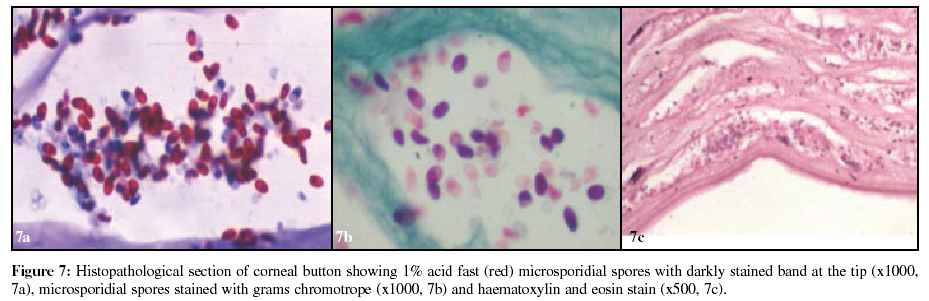
Light microscopic examination of specimens allows diagnosis of microsporidial infections, but genus and species differentiation is uncertain. Parasites are seen as oval refractile bodies within cells as well as extracellular. Specimens stained with Gram stain [Figure - 4] show oval, gram positive spores[19] resembling yeast but this can be confirmed by special stains like 1% acid-fast stain and Weber modified trichrome stain[26] which discloses bright pinkish-red spores and most have a distinctive diagonal or equatorial line. These spores measure about 1.5 x 3 mm. Also these strutures are non-budding, that allows microsporidia to be easily differentiated from yeast. Various chemifluorescent brighteners such as calcofluor white [Figure - 5] or Uvitex 2B bind to the endospore layer of microsporidia and allow spores to be detected quickly and easily in smears of specimens examined with a fluorescence microscope.[6] Although fluorescent stains seem to be more sensitive than chromotrope based trichrome or 1% acid fast stains, they may lead to some false positive results due to the similarity in staining of small yeast cells. Histopathology The corneal biopsy specimens show oval bodies measuring 2.5 to 3 by 4.5 to 5, involving mostly the deep stroma, with extension into anterior layers. The spores show a thick band like nucleus at one pole and stain positively with haematoxylin and eosin stain, chromotrope trichrome stain, 1% acid fast stain [Figure 6a], [Figure 6b], [Figure 6c] and variably with Gomori methenamine silver stain. Inflammation varies from moderate to severe, with deep stromal abscess and also show diffuse infiltration involving full thickness of corneal stroma. The semithin sections of the tissues show many viable, mature, immature, and degenerated spores, many of them being intracellular, within the macrophages as well as keratocytes.[19] The semithin sections of biopsy material stained with a variety of different stains are useful methods for visualization of spores and tissue stages of microsporidia.[28],[38] In case of superficial keratitis, the specimens reveal infection confined to the superficial epithelial layers of the cornea, sparing the stroma. Inflammatory cells can be seen intra-epithelially and sub-epithelially.[19] Transmission electron microscopy Originally, definitive diagnosis of microsporidiosis required ultrastructural examination of samples by transmission electron microscopy (TEM). Microsporidia can be identified to the genus or even species level based on fine structure features of the spores [Figure 7a], [Figure 7b], [Figure 7c] and proliferative forms, method of division and nature of host cell parasite interface.[1] In tissue, all stages of the life cycle can often be observed. Detection of microsporidia by TEM is highly specific, but the technique may lack sensitivity. Likewise, sample preparation and examination are laborious and time-consuming.[39] Cell culture The in vitro cultivation of several microsporidian species that infect humans has been of enormous benefit, both for our understanding of the biologic aspects of the host-parasite relationship and for the development of immunologic reagents for diagnosis and species differentiation. In vitro cultures have also been used to assess the effects of antimicrobial agents on several microsporidian species.[40]-[43] In vitro cultures combined with ultrastructural, biochemical, antigenic or molecular analysis have been used to confirm infections with existing species of microsporidia[44]-[46] as well as to define new species.[47] However, their use in routine clinical diagnosis is not practical because they are time consuming and laborious and only specialized laboratories maintain cell cultures with microsporidia.
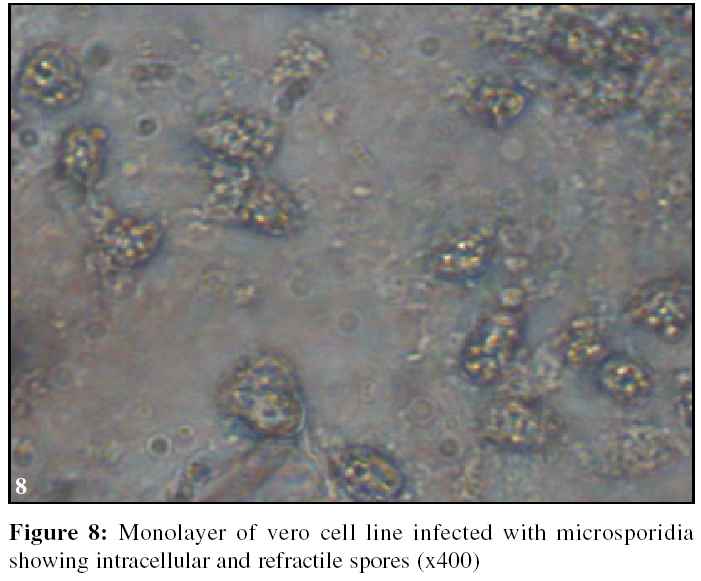
Microsporidia cannot be cultivated axenically because of their obligate intracellular development, but they have been successfully cultivated in a number of mammalian cell lines including monkey
[Figure - 8] and rabbit kidney cells (vero and RK13), human fetal lung fibroblasts (MRC-5), MDCK cells and several other cell lines.[44]-[48] Several animal models have been established to study microsporidial
infection[48]-[50] as well as for producing polyclonal and monoclonal antibodies.[45],[51],[52] BALB/c and C57B1/6 athymic mice have been used and have been injected intraperitoneally with Encephalitozoon cuniculi , Encephalitozoon hellem or Vittaforma corneae.[50],[53] SCID mice have also been infected by oral inoculation of E. cuniculi spores.[54] Successful transmission of E. cuniculi to rabbits by administration of spores orally and rectally has been reported.[49]
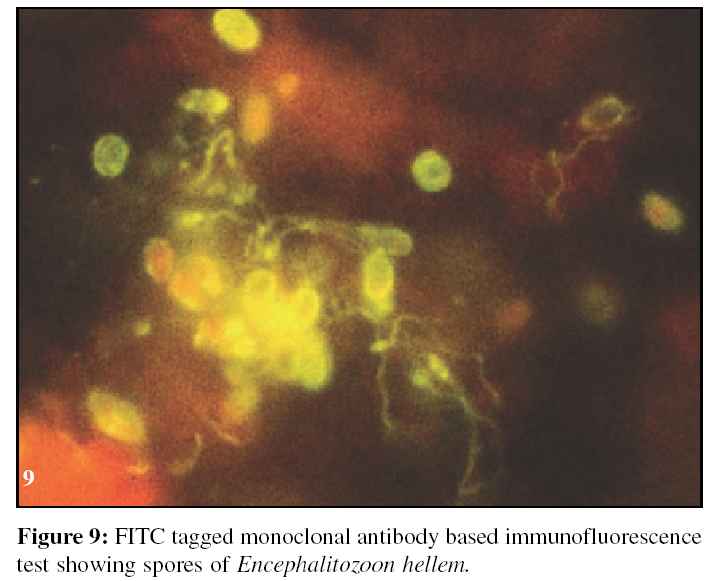
Microsporidium specific antibodies in immuno-fluorescence tests
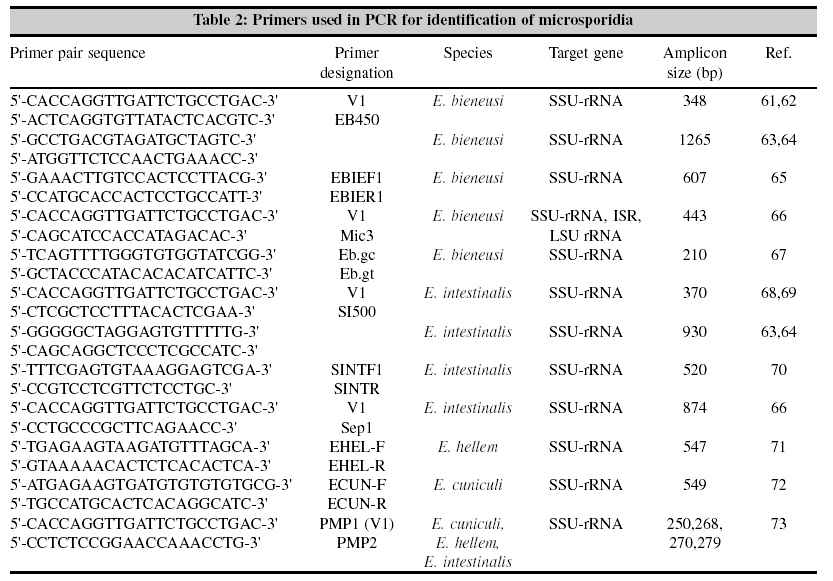
[Figure - 9] have been used for the diagnosis and species differentiation of microsporidia. Polyclonal and monoclonal antibodies were also used for Western blot analysis of several microsporidian species.[45],[51],[52],[55] These immunofluorescence antibody tests seem to be useful as they have been shown to recognize species-specific surfaces of the spores or polar tube proteins of microsporidia. Comparative studies with routine staining methods have shown lesser sensitivity of immunofluorescence detection procedures. As a consequence, immunofluorescence antibody tests, which are not widely available, should be used only as confirmation and for species differentiation after initial diagnosis with routine staining methods such as fluorescent or chromotrope based stain.[40] Serologic assays used to detect antibodies to microsporidia in human sera include immunofluorescence, immunoperoxidase, enzyme-linked immunosorbent assay (ELISA) and Western blot.[38],[56],[57] The specificity of all serologic tests used in humans, however, is still unknown, and it is uncertain whether detection of antibodies to microsporidia reflects true infections, antigen exposure without establishment of the parasite, cross-reactivity to other microsporidial or non-microsporidial microorganisms, or reaction due to polyclonal B cell stimulation, particularly in serum samples of patients with tropical diseases.[58] More studies with sera of immunocompetent subjects with proven microsporidial infections are required to define the diagnostic parameters of these serologic tests. There are no reports on use of serologic assays to detect antibodies in serum or tears in ocular microsporidiosis. Molecular studies Molecular studies of microsporidia are in their infancy. Many different genes of human infecting microsporidia have been sequenced in the last few years. One milestone is the complete sequencing of the whole genome of E. cuniculi by a research group in France.[59] Molecular based methods are important for taxonomic classification, phylogenetic studies and especially for detection and species differentiation of microsporidia in clinical samples.[1] Several polymerase chain reaction based methods have been published, to amplify different regions of the small subunit (SSU) and large subunit (LSU), ribosomal (rRNA) gene as well as the intergenic spacer region for diagnosis and species differentiation of microsporidia infecting humans.[1],[60] The list of primer pairs used in the identification of microsporidia are given in [Table - 2]. Several researchers have published studies with these primer pairs, usually with excellent results.[61]-[73] Comparison of molecular techniques with light microscopy, in the diagnosis of microsporidial infection, is difficult. In a blinded multicenter study that compared PCR with light microscopy, the greatest differences in sensitivity were found between individual laboratories rather than between different techniques.[74] Nevertheless, in combination with light microscopy, DNA amplification by PCR offers an excellent approach to diagnosing microsporidiosis with the advantage of a simple species differentiation.[75] Second step methods have been employed after PCR to corroborate or specifically identify the PCR products. These methods include DNA sequencing, RFLP and heteroduplex analysis. Southern analysis also has been used to detect E. bieneusi when insufficient PCR amplified rDNA was generated for visualization on ethidium bromide stained gel.[76] DNA probes and restriction enzyme digestion have also been used to confirm the identity of PCR amplicons.[77],[78] In a recent paper,[79] the shortcomings of the above techniques were overcome by developing a quantitative detection method for E. hellem, E. cuniculi and E. intestinalis that is specific and sensitive for clinical samples. This technique is called fluorogenic 5′ nuclease PCR assay. Its sensitivity on clinical specimens remains to be evaluated. In-situ hybridization In situ hybridization has been established for the diagnosis of infections with E. bieneusi in humans and experimentally HIV-infected rhesus monkeys.[77] The described probes were directed against the SSU-rRNA of E. bieneusi. and allowed the identification of different microsporidian stages including plasmodia and spores. However, this elegant but time-consuming method has not been described for other human infecting microsporidia and sensitivity and specificity have not been evaluated.[78] Future trends rRNA data have suggested that microsporidia are one of the most ancient eukaryotic lineages. On the other hand, the relatedness of microsporidia to fungi and animals, as suggested by the α and β tubulin and mitochondrion-type Hsp70 sequences, invites speculation that microsporidia evolved degeneratively from higher forms. Examination of protein-coding sequences from microsporidia will be of interest to answer this question and is under way. The taxonomy of microsporidia has undergone several changes during the last few years and will continue to change significantly in the near future when new DNA-based data are incorporated into new classification systems. At present, only limited data have been published comparing molecular techniques for diagnosis of microsporidia with traditional methods of determining the sensitivity and specificity of these new techniques. Nevertheless, these studies indicate that the sensitivity and specificity of molecular diagnostic techniques can be very high. Therapy Currently, antimicrosporidial therapy is in a state of flux. For the invasive microsporidia, especially the Encephalito-zoonidae , albendazole appears to be a useful therapeutic agent.This is not the case for Enterocytozoon bieneusi infection where fumagillin appears to be the most promising agent.[80] Resolution of infection of the corneal epithelium with itraconazole,[29],[81] metronidazole[1] as well as topical propamidine isethionate (Brolene)[27] has also been reported. Therefore, identifying microsporidia to species level could have important implications in the clinical management of patients.[1],[59]Prognosis Keratoconjunctivits is now invariably diagnosed on the basis of clinical and microbiologic findings, hence is more amenable to medical treatment. Stromal keratitis being deep seated and often misdiagnosed as herpetic keratitis may be missed on clinical diagnosis thereby necessitating surgical intervention. It is important to note that none of the cases have been reported to have an intraocular spread or recurrence of the infection. Introduction of new methods of in vivo diagnosis would however be very useful in clinical management. Although there are treatment regimens currently under evaluation that appear successful in relieving symptoms of ocular microsporidiosis, further clinical and epidemiologic studies are necessary to test and develop efficacious treatment regimens and to understand the natural course of the disease.Conclusions Microsporidia are an important cause of disease in HIV-infected patients and are now increasingly also recognized as pathogens in non-HIV-infected patients with or without immunosuppression. Therefore, high index of suspicion is warranted for both the clinicians, microbiologists and pathologists. In addition to morphologic diagnosis by conventional methods, efforts should be made to establish and validate the new methods (PCR, Serology and other molecular tools) for the diagnosis and species differentiation of microsporidia on clinical specimens.As is true for many other new and emerging pathogens, we have just scratched the surface of a complex and evolving relation between the phylum Microspora and humans. Application of molecular techniques to diagnosis, species differentiation, and phylogentic analysis of microsporidia will lead to an enormously increased knowledge of these organisms in the near future. References
Copyright 2005 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb05024f5.jpg] [mb05024f3.jpg] [mb05024f9.jpg] [mb05024f6.jpg] [mb05024f4.jpg] [mb05024f1.jpg] [mb05024f8.jpg] [mb05024f2a-c.jpg] [mb05024t1.jpg] [mb05024f7a-c.jpg] [mb05024t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}