 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 23, No. 2, April-June, 2005, pp. 120-124 Original Article Evaluation of Methods for AmpC Beta-Lactamase in Gram Negative Clinical Isolates from Tertiary Care Hospitals Singhal S., Mathur T., Khan S., Upadhyay D.J., Chugh S., Gaind R., Rattan A. New Drug Discovery Research, Ranbaxy Research Laboratories,
Gurgaon - 122 001
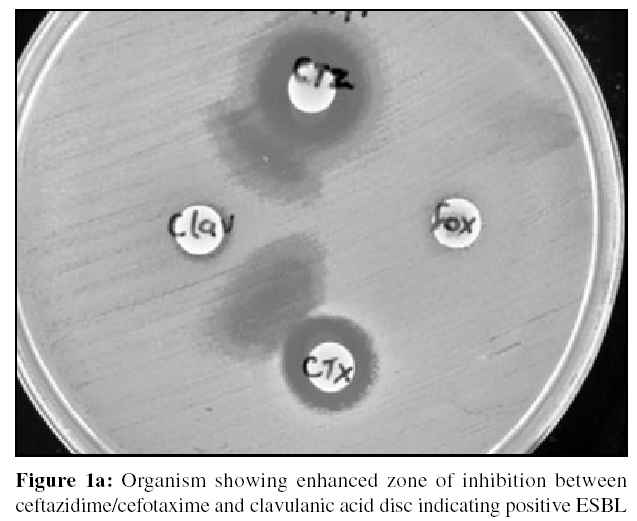
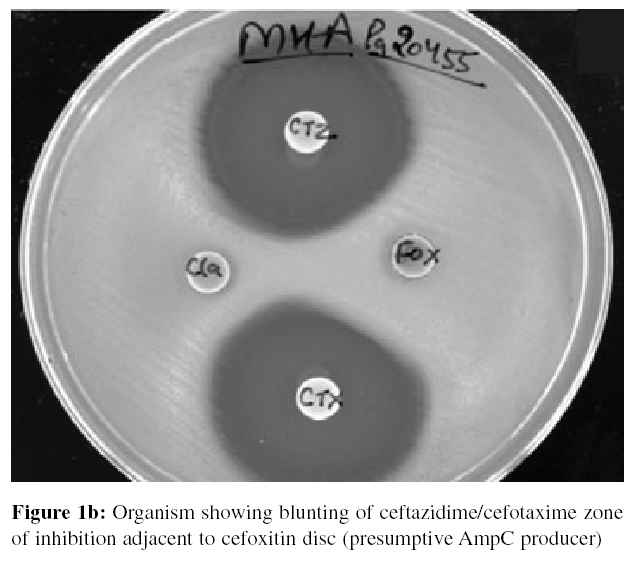
Code Number: mb05032 Abstract The purpose of this study was to simultaneously screen for Extended-spectrum β-lactamases (ESBL) and AmpC β-lactamases in gram negative clinical isolates from four tertiary care hospitals and further to compare two detection methods three-dimensional extraction method and AmpC disk test for AmpC β-lactamases. A total of 272 isolates were screened for ESBL and AmpC β-lactamase by modified double disk approximation method (MDDM). Synergy observed between disks of ceftazidime/cefotaxime and clavulanate were considered as ESBL producer. Isolates showing reduced susceptibility to either of the test drugs (ceftazidime or cefotaxime) and cefoxitin were considered as presumptive AmpC producers and further confirmed by three-dimensional extraction method and AmpC disk test. A total of 173 (64%) of the isolates were found to be ESBL positive and 61 (23%) showed resistant to cefoxitin. ESBL was detected in 80 (62%) isolates of E. coli and 71 (73%) of Klebsiella spp. The occurrence of AmpC β-lactamases was found to be 8% (22) of the total isolates and the two detection methods for AmpCβ -lactamase showed concordant results. Screening for ESBL and AmpC can be simultaneously done by MDDM method and confirmation for AmpC β-lactamase should be carried out routinely in tertiary care hospitals by AmpC disk test, as it is a simple and rapid procedure.Keywords: ESBL, AmpC β-lactamases, Disk test Extended-spectrum β-lactamases (ESBLs) and AmpC β-lactamases are of increasing clinical concern. ESBLs are most commonly produced by Klebsiella spp. and Escherichia coli but may also occur in other gram-negative bacteria. They are typically plasmid mediated, clavulanate susceptible enzymes that hydrolyze penicillins, expanded-spectrum cephalosporins (cefotaxime, ceftriaxone, ceftazidime, cefepime and others) and aztreonam.[1] AmpC class β-lactamases are cephalosporinases that are poorly inhibited by clavulanic acid. They can be differentiated from other ESBLs by their ability to hydrolyze cephamycins as well as other extended-spectrum cephalosporins.[2] AmpC- β-lactamases, demonstrated or presumed to be chromosomally or plasmid mediated, have been described in pathogens e.g., Klebsiella pneumoniae , Escherichia coli , Salmonella spp., Proteus mirabilis, Citrobacter freundii , Acinetobacter , Enterobacter spp. and Pseudomonas aeruginosa .[3] Although reported with increasing frequency, the true rate of occurrence of AmpC β-lactamases in different organisms, including members of Enterobacteriaceae , remains unknown. Coudron et al[4] used the standard disk diffusion breakpoint for cefoxitin (zone diameter <18 mm) to screen isolates and used a three- dimensional extract test as a confirmatory test for isolates that harbour AmpC β-lactamases. The current National Committee for Clinical Laboratory Standards (NCCLS) guidelines do not describe any method for detection of isolates producing AmpC β-lactamases.[5] The present study was designed to increase awareness and demonstrate the need to detect the occurrence of ESBLs and AmpC enzymes in clinical strains. We had screened the isolates by modified double disk approximation method (MDDM) and selected the isolates showing reduced susceptibility to ceftazidime/cefotaxime and cefoxitin or showing blunting of ceftazidime or cefotaxime zone of inhibition adjacent to cefoxitin. These isolates were further subjected for AmpC β-lactamases confirmation by modified three-dimensional extract test[2] and AmpC disk test.[6] Materials and Methods Bacterial isolatesA total of 272 gram negative consecutive, nonrepetitive clinical isolates from blood and urine from tertiary care hospitals of India were studied over a period of four months (January to April 2004). All the isolates were identified by standard biochemical methods at the referral hospitals. The participating hospitals were Safdarjung Hospital, New Delhi; AMU, Aligarh; BHU, Varanasi and KIMS, Hubli. NCCLS reference strains ESBL positive K. pneumoniae ATCC 700603 and sensitive E. coli ATCC 25922 were also included in the study. Screening for ESBL and AmpC producing isolates In order to simultaneously detect ESBL and AmpC, a modified double disk approximation method (MDDM), was devised. A 0.5 McFarland of test isolate was swabbed on Mueller Hinton Agar (Difco) plates and disk of cefotaxime (30 µg) and ceftazidime (30 µg) were placed adjacent to clavulanic acid (10 µg) and Cefoxitin (30 µg) disk at a distance of 20 mm from each other. After incubation, an enhanced zone of inhibition between any of the disks (ceftazidime / cefotaxime) and clavulanic acid were interpreted as presumptive evidence for the presence of ESBL [Figure 1a]. All ESBL positive isolates were further confirmed by determining their MICs in presence of clavulanate as per NCCLS micro broth dilution method.[7] Isolates showing blunting of ceftazidime or cefotaxime zone of inhibition adjacent to cefoxitin disk [Figure 1b] or showing reduced susceptibility to either of the above test drugs (ceftazidime or cefotaxime) and cefoxitin were considered as "screen positive" and selected for detection of AmpC β-lactamases. Detection of AmpC β-lactamases Modified three dimensional test The selected isolates were studied for the presence of AmpC enzyme by modified three-dimensional extract test.[2] Briefly, fresh overnight growth from Mueller Hinton agar (MHA) was transferred to a preweighed sterile micro centrifuge tube. The tube was weighed again to determine the weight of bacterial mass to obtain 10-15 mg of bacterial wet weight. The bacterial mass was suspended in peptone water and pelleted by centrifugation at 3000 rpm for 15 minutes. Crude enzyme extract was prepared by repeated freeze thawing of the bacterial pellet (approximately 10 cycles). Lawn culture of E. coli ATCC 25922 was prepared on MHA plates and cefoxitin (30 µg) disk were placed on the plates. Linear slits (3 cm) were cut using sterile surgical blade, 3 mm away from cefoxitin disk. At the other end of the slit a small circular well was made and the enzyme extract was loaded. A total of 30 to 40 µl of extract was loaded in the well at a 10 µl increment. The plates were kept upright for 5 to 10 minutes until the liquid dried and were incubated at 37°C for 24h. Enhanced growth of the surface organism at the point where the slit inserted the zone of inhibition of cefoxitin was considered a positive three-dimensional test and was interpretated as evidence for the presence of AmpC β-lactamases. Three different types of results were recorded. Isolates showing clear distortion of the zone of inhibition of cefoxitin were taken as AmpC producers. Isolates with no distortion were recorded as non-AmpC producers where as isolates showing minimal distortion were considered as indeterminate strains
AmpC Disk Test Results Screening for ESBLs and AmpC β-lactamasesTwo hundred and seventy two isolates were screened for both ESBL and AmpC b-Lactamase production by modified double disk approximation method (MDDM). Of this 173 (64%) isolates were found to be ESBL positive whereas 38 were ESBL negative. Out of the total isolates 73% of Klebsiella spp. (n=71) and 62% of E. coli (n=80) were found to be ESBL positive [Table - 1], [Figure 1a]. Of the 272 isolates, 61 showed reduced susceptibility to either of the test drugs (ceftazidime or cefotaxime) and cefoxitin [Table - 1]. Three of these isolates also showed blunting of the inhibition zone of either ceftazidime or cefotaxime adjacent to cefoxitin disk [Figure 1b] were considered as presumptive AmpC producers and further confirmed by three-dimensional extraction method and AmpC disk test.
Our results also demonstrated the co-existence phenotype of both ESBL and AmpC in two isolates. (One each of Klebsiella spp. and E. coli) . AmpC b-lactamase production was confirmed in 22 isolates (8%) of the 272 isolates or 36% of the 61 screen positive isolates by the three-dimensional test. A clear distortion of the zone of inhibition of cefoxitin was observed in 18 isolates whereas three isolates showed minimal distortion and were considered as indeterminate strains [Figure - 2].
AmpC Disk Test Discussion Despite the discovery of ESBLs and AmpC β-lactamases at least a decade ago, there remains a low level of awareness of their importance and many clinical laboratories have problems in detecting ESBLs and AmpC β-lactamases. Confusion exists about the importance of these resistance mechanisms, optimal test methods, and appropriate reporting conventions. Failure to detect these enzymes has contributed to their uncontrolled spread and sometimes to therapeutic failures.[8]The objective of this work was to obtain some experimentally based prediction on the possible emergence of ′extended spectrum′ AmpC β-lactamases in tertiary care hospitals and further to compare two phenotypic AmpC detecting methods. Detection and reporting isolates producing AmpC β-lactamases are more difficult issues than those associated with ESBLs. E. coli , Klebsiella pneumoniae and Proteus mirabilis are the species in family Enterobacteriaceae most commonly isolated in the clinical laboratory.[9] However, few studies have assessed the occurrence of AmpC β-lactamases among these species. The NCCLS documents[5] do not indicate the screening and confirmatory test that should be used for the detection of AmpC β-lactamases in Klebsiella pneumoniae and E. coli. With the modified double disk diffusion screen test we identified 173 ESBLs and 61 isolates as possible AmpC producers resistant to cefoxitin. Further investigation of this phenotypic screening method for identifying possible AmpC producers seems warranted, as it offers the potential to significantly reduce the number of isolates that would require a confirmatory test for AmpC production, such as the three-dimensional test or AmpC disk test with cefoxitin. Our initial screening also demonstrated the co-existence phenotype of both ESBL and AmpC in two isolates (one each of Klebsiella spp. and E. coli ). This could be because plasmid-mediated AmpC enzymes have also been shown to disseminate among Enterobacteriaceae , sometimes in combination with ESBLs. It might be highly desirable to develop an ESBL detection test that includes a substrate displaying a higher degree of resistance to such AmpC enzymes.[9],[10] We used cefoxitin resistance to screen isolates for detecting possible AmpC β-lactamases and three dimensional extract test and AmpC disk test for confirmation. The three dimensional and AmpC disk test are sensitive and 22 isolates were identified by both the methods as AmpC producers. In the present study, ESBL producing isolates of Klebsiella spp. (73%) and E. coli (62%) were isolated from inpatient units as well as from clinical samples from patients attending outpatient clinics. In contrast, all the AmpC harbouring organisms (8%) were found only in clinical specimens from admitted patients. It has been reported that at present in India AmpC harbouring isolates are largely restricted to the hospitalized patients only.[2],[11] In our study AmpC β-lactamases was seen mainly in Acinetobacter spp. (28.57%) followed by E. coli (6.97%) and Klebsiella spp. (6.18%). The AmpC disk test was an easier, reliable and rapid method of detection of isolates that harbour AmpC β-lactamases. This suggests that AmpC disk test can be used for routine screening of the AmpC enzyme in the clinical laboratory. Acknowledgement We appreciate the help of Dr. M. Shahid (AMU) Aligarh, Dr. Ravi (KIMS) Hubli and Dr. Arpita (BHU) Varanasi for providing the clinical isolates for this study.References
Copyright 2005 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb05032t2.jpg] [mb05032t1.jpg] [mb05032f2.jpg] [mb05032f1a.jpg] [mb05032f3.jpg] [mb05032f1b.jpg] |
| |||||||||
{kind=link}
{kind=link}
![[Figure - 2]](/showimage?mb/photo/mb05032f2.jpg){kind=link}
![[Figure - 3]](/showimage?mb/photo/mb05032f3.jpg){kind=link}