
|
Indian Journal of Medical Microbiology
Medknow Publications on behalf of Indian Association of Medical Microbiology
ISSN: 0255-0857 EISSN: 1998-3646
Vol. 23, Num. 4, 2005, pp. 214-219
|
Indian Journal of Medical Microbiology, Vol. 23, No. 4, October-December, 2005, pp. 214-219
Review Articles
Enterococcal resistance - An overview
Marothi YA*, Agnihotri H, Dubey D
*Corresponding author (email: )
Depatment
of Microbiology, MGM Medical College, Indore-, Madhya Pradesh
Code Number: mb05068
Abstract
Nosocomial acquisition of microorganisms resistant to multiple antibiotics
represents a threat to patient safety. Here, we review the antimicrobial
resistance in Enterococcus , which makes it important nosocomial
pathogen. The emergence of enterococci with acquired resistance to vancomycin
has been particularly problematic as it often occurs in enterococci that
are also highly resistant to ampicillin and aminoglycoside thereby associated
with devastating therapeutic consequences. Multiple factors contribute
to colonization and infection with vancomycin resistant enterococci ultimately
leading to environmental contamination and cross infection. Decreasing
the prevalence of these resistant strains by multiple control efforts therefore,
is of paramount importance.
Keywords: Enterococci, antimicrobial resistance, therapeutic options, control efforts
Enterococci, though commensals in adult faeces are important nosocomial pathogens. [1],[2],[3]Their emergence in past two decades is in many respects attributable to their resistance to many commonly used antimicrobial agents (aminoglycosides, cephalosporins, aztreonam, semisynthetic penicillin, trimethoprim-sulphamethoxazole)[4],[5] and ease with which they appear to attain and transfer resistant genes,[6] thus giving rise to enterococci with high level aminoglycoside resistance (HLAR), β -lactamase production and glycopeptide resistance.
The most common nosocomial infections produced by these organisms are
urinary tract infections (associated with instrumentation and antimicrobial
administration), followed by intra-abdominal and pelvic infections. They
also cause surgical wound infections, bacteraemia, endocarditis, neonatal
sepsis and rarely meningitis.[2],[6],[7] E.faecalis is
the most common cause (80-90%)of infection followed by E.faecium (10-15%).[7] However,
emergence of enterococci with multi drug resistance particularly to vancomycin
is predominantly seen in E.faecium [8] followed
by increase in frequency of its recovery from infection. As vancomycin
resistant enterococci (VRE) also have ampicillin resistance and HLAR,
they are the most difficult to treat. Thus, this entity merits a complete
description of antimicrobial resistance, current possibilities for treatment
and variety of measures that may limit the proliferation of resistance
within a health care environment.
Antimicrobial Resistance Enterococci have a remarkable ability to survive in an environment of heavy antibiotics. Indeed, it is the resistance of these organisms to multiple antimicrobial agents that makes them such feared opponents. Antimicrobial resistance in enterococci is of two types: inherent/ intrinsic resistance and acquired resistance. Intrinsic resistance is species characteristics and thus present in all members of species and is chromosomally mediated. Enterococci exhibits intrinsic resistance to penicillinase susceptible penicillin (low level), penicillinase resistant penicillins, cephalosporins, lincosamides, nalidixic acid, low level of aminoglycoside and low level of clindamycin.[1] Although most enterococci are susceptible to co-trimoxazole in vitro , this combination does not work in vivo , because enterococci are able to incorporate preformed folic acid which enables them to bypass the inhibition of folate synthesis produced by co-trimoxazole.[2] On the other hand, acquired resistance results from either mutation in DNA or acquisition of new DNA. Examples of acquired resistance include resistance to penicillin by β -lactamases, HLAR, vancomycin, chloramphenicol, erythromycin, high level of clindamycin, tetracycline and fluroquinolone resistance.[1] Resistance to β -Lactams
Intrinsic resistance
Enterococci begin with intrinsic resistance to most β -lactam antibiotics because of low affinity penicillin binding proteins (PBPs), which enable them to synthesize cell wall components even in the presence of modest concentration of most β -lactam
antibiotics.[1],[2] While most isolates of E.faecalis can be inhibited by concentration of penicillin achievable in the plasma (MIC of 1 to 8 μgm/mL) this is usually not the case with E.faecium (MIC of 16 to 64 μgm/mL). Higher level of resistance in E.faecium has been attributed to over production of low affinity PBP-5, a protein that can take over the function of all PBPs.[9] Moreover, concentration of ampicillin that are needed to inhibit enterococci are about half that of penicillin.[3] Thus, in general, ampicillin is more effective than penicillin in vitro .[10]
Tolerance
In addition, enterococci are "tolerant" to the activity of β -
lactams, that is, enterococci are inhibited but not killed by these agents.
This property is an acquired characteristic. Enterococci quickly develop
tolerance after exposure to as few as five doses of penicillin. As most
enterococci are tolerant to cell wall active agents, penicillin or glycopeptide,
alone often fail to cure serious infections like endocarditis and meningitis
which require bactericidal therapy and this is achieved by synergistic
effect of penicillin/ampicillin plus aminoglycoside: standard treatment
for serious infection.[2],[3]
β -lactamase enzyme
Enterococci, exclusively strains of E. faecalis , expressing β -lactamase
enzyme and having high level resistance to penicillin (HLPR) and ampicillin
(MIC > 256 μgm/mL) have been reported from various locations. [11],[12],[13],[14],[15],[16]Its
production is plasmid mediated and enzyme is constitutively produced. Because
amount of β -lactamase production by enterococci may be insufficient for detection by routine antibiotic susceptibility testing, isolates from serious infection such as bacteraemia should be screened specifically for β -lactamase
production.[17] Recommended
and reliable method for β -lactamase production is chromogenic cephalosporin,
nitrocefin.[18] E. faecalis strains
producing β -lactamase are not susceptible to anti-staphylococcal
penicillins but are susceptible to ampicillin, amoxicillin and piperacillin
combined with drugs that inhibit penicillinase such as clavulanic acid,
sulbactam and tazobactam.[3],[14]
With a single known exception, isolates of E.faecium do not produce penicillinase yet confer high level resistance (HLR).[8],[19] This, HLPR of E.faecium may be extreme example of intrinsic resistance associated with low affinity PBPs or may represent acquired resistance.[1]
Aminoglycoside Resistance
Intrinsic resistance
Enterococci exhibit low level resistance to all aminoglycosides (MIC
8 to 256 μgm/mL) which appears to be due to low uptake of these agents.
However, aminoglycoside uptake is enhanced when enterococci are exposed
to β -lactams.[1] This synergy underlies the long standing practise of combining both classes of antibiotics to treat serious enterococcal infections as combination overcomes the intrinsic resistance exhibited by enterococci and a synergistic effect is usually achieved since the intracellular penetration of aminoglycoside is facilitated by cell wall active agent.
Acquired resistance
Combination of penicillin plus streptomycin produced bactericidal
killing of enterococci, until unfortunately, enterococci developed HLR
to streptomycin. [20],[21],[22],[23],[24] But
these isolates were not highly resistant to gentamicin thereby leading
to widespread use of gentamicin plus penicillin for serious infections.
Subsequently, however enterococci developed HLR to gentamicin (HLGR) that
caused resistance to synergism between gentamicin and penicillin.[8],[11],[13],[16],[19], [25],[26],[27] This
acquired resistance is highly specific and renders bacteria resistant to
high levels of aminoglycosides and as a result resistance to synergism.
HLAR is defined as occurring when drug concentration of > 2000
μgm/mL are required for inhibition of organism. HLAR is being conducted
by series of aminoglycoside modifying enzymes (AME) coded by plasmid and
are transferable. The most frequently encountered enzyme include a) dual
function 2′phosphotransferase and 6′acetyl transferase conferring HLR to all available aminoglycoside (kanamycin, gentamicin, amikacin, netilmicin, tobramycin) except streptomycin; b) 3′phosphotransferase coding for HLR to kanamycin and penicillin-amikacin synergy without HLR to gentamicin; c) 6′adenyl
transferase which produces HLR to streptomycin but does not inactivate
other useful aminoglycosides.[1] Although
no single enzyme can inactivate all available aminoglycosides, 30% of
VRE strains can produce multiple enzyme types and are thus highly resistant
to all known aminoglycosides.[9]
Screening for HLAR
As routine disc diffusion does not detect HLAR,[28] a
formal MIC determination which shows that the MIC is > 2000
μgm/mL is definitive for HLR and resistance to synergism. However, performing
full MICs routinely is quite cumbersome and time consuming. Thus, several
alternative methods have been proposed for detection of HLAR. These methods
are: agar screening, high content disc and broth dilution.
Agar screening
Concentration of > 2000 μgm/mL for streptomycin and
other aminoglycosides and 500 μgm/mL for gentamicin are recommended as
break points.[6],[10] The
500 μgm/mL dilution (rather than > 2000 μgm/mL) is used for
screening gentamicin since some strains exhibiting MICs of 500-1000 μgm/ml
also resist synergy of killing. Inocula of 104 and
106 cfu per spot gives best
result regardless of medium used.[29] Growth
of a single colony on agar dilution plates indicates resistance.
High content disc
Discs of 120 μgm of gentamicin, kanamycin and 300 μgm of streptomycin
are recommended for disc diffusion test. Resistance is indicated by
no zone and susceptibility by a zone of > 10mm, strains
with zone of 7mm-9mm should be tested by dilution methods. For amikacin
disc
test
results, considerable overlap occurs between zone size ranges of susceptible
and resistant isolates. Thus, amikacin cannot be used to determine E. faecalis susceptibility
to amikacin-penicillin synergy. In contrast, kanamycin disc more accurately
predicts amikacin-penicillin synergy than does amikacin. Thereby, kanamycin
proves to be an accurate and reliable substitute.[30]
Broth dilution test
Single concentration of 1000 μgm/mL of streptomycin[10] and
500 μgm/ml gentamicin by microdilution are recommended as break points.[31] An
inoculum of 10[5] cfu/mL
is recommended for testing since inoculum size has been found to be
important
factor in reliable detection of HLR.[29]
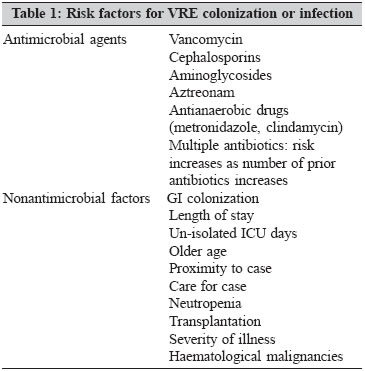
Glycopeptide Resistance Considerable consternation greeted the first report of appearance of VRE in 1980s[32] followed by its rapid spread[8],[25],[26],[33],[34],[35] thereby becoming a significant clinical problem. Three phenotypes of glycopeptide resistance have been reported in enterococci: Van A phenotype, with inducible high level resistance to both vancomycin (MIC > 64 μgm/mL) and teicoplanin (MIC > 16 μgm/mL), Van B with variable levels of inducible resistance to vancomycin (MIC 8 to 64 μgm/mL) and sensitive to teicoplanin (MIC < 1 μgm/mL), Van C phenotype with intrinsic, constitutive low level resistance to vancomycin (MIC > 8 and < 32 μgm/mL) and susceptibility to teicoplanin (MIC < 1 μgm/mL).[7] Van A and Van B are usually associated with E.faecalis and E.faecium whereas Van C are seen in E.gallinarum and E.casseliflavus strains. Van A is more widely distributed and thus the predominant type of resistance reported.[3] Moreover, vancomycin resistance has appeared preferentially in E.faecium, which is inherently more resistant to multiple drugs making therapy extremely problematic.[4] Clinically, vancomycin resistance has been associated with more frequent episodes of recurrent bacteraemia, persistent isolation of enterococci from primary sites of infection, increased frequency of endovascular infection and increased mortality.[10] Colonization and infection Faecal carriage of VRE is recognized to be frequently associated with serious clinical infection and it is likely that colonization of gastrointestinal tract occurs as a prelude to clinical infection. Risk factors for colonization and invasive disease include both heavy use of antimicrobial agents (especially vancomycin, third generation cephalosporins and antimicrobial agents with activity against anaerobes etc.) and variety of non antimicrobial factors including prior GI colonization with VRE, increased length of hospital stay, older age, proximity to case, care for a case by health care worker with GI colonization with VRE and immunosuppressive opponents[2],[5],[8],[36],[37],[38] [Table
- 1]. Furthermore, these colonized patients contaminate themselves as well as environment, thereby having potential for transfer of VRE from environment to patients.[8],[9] As VRE survives for long periods of time on dry surfaces[38] it is a successful environment contaminant causing some outbreaks.[25]
Screening methods for detection of VRE
In the face of increasing rate of colonization with VRE and in the light
of increasing concerns about the possible effect of this organism on
patients with high risk of infections screening methods have been introduced
for detection of VRE. The reliable and recommended agar screen method
includes using brain heart infusion (BHI) agar with 6 μgm of vancomycin
per mL.[17] Inoculum of
105 - 106 cfu is spotted and plate incubated at
35°
C for 24 hours. Growth indicates resistance and no growth indicates susceptibility.[6] Two Enterococcus selective
broths for isolation of VRE from colonized patients are also available.
These are enterococcal broth with bile esculin azide and sodium azide with
6 μgm vancomycin (EBVA) and M- Enterococcus broth with sodium
azide and triphenyl tetrazolium with 6 μgm vancomycin (M-EVA).[39] Similarly,
antibiotic gradient method (E test) is also able to detect VRE.[9],[10] Once
suspected, based on a screening method, vancomycin resistance should be
confirmed by using a different method.
Antibiotic synergism
Enhanced killing, called synergism is defined for enterococci as > 100
fold increase in killing by the drug combination over the killing accomplished
by most active of the two drugs when tested separately and resistance
to synergy is < 100 fold increase in killing.[30] The
use of an aminoglycoside and penicillin in combination for severe enterococcal
infections is standard for management. By mechanism of synergy, penicillin
facilitates the entry of aminoglycoside into the bacterial cell but
does not cause an irreversible defect by itself. Synergistic effect
depends on subsequent susceptibility of bacteria to aminoglycoside.
Therefore, the enzyme that inactivates aminoglycoside also makes the
organism resistant to synergism.[10]
Two most common methods used for determining synergy are the checkerboard
technique and time kill test.[10] These
are, however, too cumbersome, time consuming and labor intensive for
routine use in many laboratories. As in enterococci synergy resistance
is most frequently mediated by HLAR,[40] alternative
method used to accurately differentiate between isolates that are resistant
or susceptible to synergy is using high content aminoglycoside disc
(120 μgm of gentamicin disc and 300 μgm of streptomycin disc). It is
a convenient technique for laboratories to screen clinically E. faecalis strains
for synergy resistance. Because of greater resistance of E.faecium to
both b-lactam and aminoglycoside antibiotics, the disc agar diffusion
results can be applied only to E. faecalis isolates and not
to E. faecium strains.[30]
Therapeutic options for multiply resistant enterococci
Enterococci have a vast potential for acquiring and disseminating resistant genes.[6] As
a result of this, they are currently causing significant therapeutic
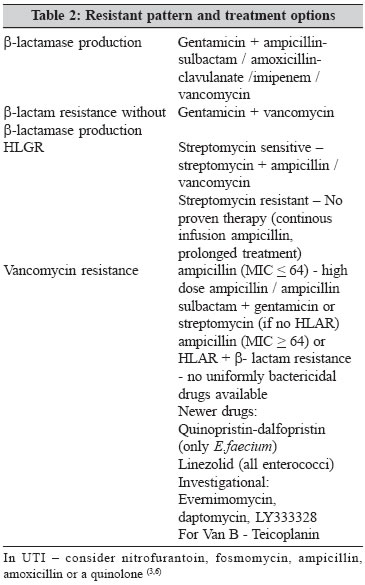
difficulties. Strains resistant to penicillin by β -lactamase production respond to gentamicin plus ampicillin-sulbactam or ampicillin - clavulanate or vancomycin. β -lactam resistance without β -lactamase
production responds to vancomycin plus gentamicin.[41] Management of clinical HLAR enterococcal infection is quite limited. The common regimen include monotherapy with vancomycin, ampicillin, penicillin, mezlocillin or piperacillin. However, relapse or primary failure occurs as penicillin or ampicillin or vancomycin alone produces a bacteriostatic rather than bactericidal effect. Currently, there is no ideal therapy which yields bactericidal activity for serious infections caused by VRE. Above all, assessing the efficacy of therapy remains difficult because VRE is often associated with severe underlying illnesses and can be a part of polymicrobial infection. Fortunately, most VRE, particularly E.faecalis are moderately susceptible to ampicillin. If the MIC for ampicillin is < 64 μgm /mL recommended therapy is high dose ampicillin or ampicillin-sulbactam combined with gentamicin or streptomycin (unless there is HLR). If VRE is highly resistant to ampicillin (MIC > 64 μgm / mL) or both to gentamicin and streptomycin, then no drug regimen will be uniformly useful.[3] Some of these strains remain susceptible to tetracycline, erythromycin, chloramphenicol, fluoroquinolones, novobiocin or rifampicin and used as monotherapy or usually combining 2 or 3 antibiotics.[2],[4] Even when a single agent or a combination of agents show in vitro activity
against a particular VRE strain, overall therapeutic efficacy may be < 70 %.[9] Teicoplanin can be used in patients exhibiting the Van B phenotype preferably in combination with streptomycin or gentamicin (if not resistant).[2] Two newer agents with activity against VRE are quinopristin-dalfopristin and linezolid which are approved. Quinopristin-dalfopristin is streptogramin combination with in vitro bacteriostatic activity against E.faecium but not against E.faecalis or other enterococcal species.[3],[9],[41] Favourable clinical responses have been obtained in approximately three quarters of patients treated with these agents.[2],[41] Limited clinical experiments suggest that linezolid (member of oxazolidinone class) is atleast as efficacious as quinopristin-dalfopristin.[41] Experimental agents with in vitro activity against VRE include glycopeptide (LY 333328), clinafloxacin, minocycline, ketolides, glycylcyclines, evernimomycin and daptomycin [Table
- 2].[2],[3],[9]
The choice of antibiotics should not only depend on antimicrobial quantitative microbiological susceptibility data, but also on the type of infection being treated (endocarditis versus urinary tract infection), the severity of this infection and clinical response to the regimen chosen.
Control efforts
Due to lack of uniformly effective antimicrobial therapy for patients infected with multiply resistant enterococci, limiting the dissemination of these organisms is of paramount significance. Primarily, the use of those antimicrobial agents that select for their isolations (cephalosporins,[42] antianaerobic drugs[37] must be limited. Recommendation to reduce cross contamination by multiply resistant enterococci include surveillance for colonization, identification of colonized and infected patients, isolation of colonized patients, the use of gowns and gloves by health care worker (barrier method), hand washing with an antiseptic after gloves removal and avoid contact with environmental surfaces after gloves removal. Medical equipments (stethoscopes,blood pressure cuffs etc.) must be dedicated to HLR patients. Environmental decontamination is also required with effective disinfectants (isopropyl alcohol, sodium hypochlorite, phenolic and quarternary ammonium compounds). [3],[4],[5],[9]
Thus, multifactorial control efforts can effect a decrease or atleast prevent an increase in the number of patients colonized or infected by these organism.
Conclusions
During past two decades, enterococci resistant to multiple antimicrobial
agents have been recognized, including strains resistant to vancomycin, β -lactams
and aminoglycosides, making it a formidable nosocomial pathogen. Such strains
pose therapeutic dilemmas for clinicians. Thus, it is crucial for laboratories
to provide accurate antimicrobial resistance patterns for enterococci so
that effective therapy and infection control measures can be initiated
References
| 1. | Murray BE. The life and times of the Enterococcus. Clin Microbiol Rev 1990; 3 :46-65. Available at http://www.pubmedcentral.nih.gov/articlerender. fcgi? tool= pubmed & pubmedid = 2404568. 2005. Back to cited text no. 1 |
| 2. | Clinical updates in infectious diseases. April 1998. Available at http://www.nfid.org/publications/clinicalupdates/id/enterococcal.html. 2005. Back to cited text no. 2 |
| 3. | Murray BE. Vancomycin-resistant enterococcal infections. N Eng J Med 2000; 342 :710-21. Available at http://jcm.asm.org/cgi/content/full/40/4/1160. 2005. Back to cited text no. 3 |
| 4. | Murray BE. Vancomycin resistant enterococci. Am J Med 1997; 101 :284-93. Back to cited text no. 4 |
| 5. | Rice LB. Emergence of vancomycin resistant enterococci. 2001. Available at http://www.cdc.gov/ncidod/eid/vol7no2/rice.htm 2005. Back to cited text no. 5 |
| 6. | In : Forbes BA, Sahm DF, Weissfeld AS, editors. Laboratory methods for detection of antibacterial resistance, Chapter 18. In Bailey and Scott's Diagnostic Microbiology. 10th ed. London: Mosby; 1998. p. 250-72. Back to cited text no. 6 |
| 7. | The gram positive cocci Part II: Streptococci, Enterococci, and the " Streptococcus -like" bacteria, Chapter 12. In : Koneman EW, Allen SD, Janda WM, Schreckenberger PC, Winn WC, editors. Color Atlas and Textbook of Diagnostic Microbiology . 5th edn. New York: JB Lipincott; 1997. p. 577-649. Back to cited text no. 7 |
| 8. | Morris JG Jr., Shay DK, Hebden JN, McCarter RJ Jr., Perdue BE, Jarvis W, et al . Enterococci resistant to multiple antimicrobial agents, including vancomycin. Ann Intern Med 1995; 23 :250-9. Back to cited text no. 8 |
| 9. | Delisle S, Perl TM. Vancomycin resistant enterococci. A road map on how to prevent the emergence and transmission of antimicrobial resistance . Chest 2003; 123 :504S-18S. Available at http://www.chestjournal.org/cgi/content/abstract/123/5_suppl/504S 2005. Back to cited text no. 9 |
| 10. | Antimicrobial susceptibility testing. In : Koneman EW, Allen SD, Janda WM, Schreckenberger PC, Winn WC,editors. Color Atlas and Textbook of Diagnostic Microbiology , 5th edn. New York: JB Lipincott; 1997. p. 785-856. Back to cited text no. 10 |
| 11. | Patterson JE, Masecar BL and Zervos MJ. Characterisation and comparison of two penicillinase producing strains of Streptococcus (Enterococcus) faecalis [published erratum appears in Antimicrob Agents Chemother 1989; 33 :20-25]. Antimicrob Agents Chemother 1988;32:122-124. Available at http://www.pubmedcentral.nih.gov/articlerender.fcgi? tool = pubmed & pubmedid = 3126703. 2005. Back to cited text no. 11 |
| 12. | Rhinehart E, Smith NE, Wennersten C, Gorss E, Freeman J, Eliopoulos GM, et al . Rapid dissemination of b-lactamase producing, aminoglycoside-resistant Enterococcus faecalis among patients and staff on an infant-toddler surgical ward. N Eng J Med 1990; 323: 1814-8. Back to cited text no. 12 |
| 13. | Rice LB, Eliopoulos GM, Wennersten C, Goldmann D, Jacoby GA, Moellering RC Jr. Chromosomally mediated b-lactamase production and gentamicin resistance in Enterococcus faecalis . Antimicrob Agents Chemother 1991; 35 :272-6. Available at http://www.pubmedcentral.nih.gov/articlerender.fcgi? tool = pubmed & pubmedid = 1902647. 2005. Back to cited text no. 13 |
| 14. | Wells VD, Wong ES, Murray BE, Coudron PE, Williams DS, Markowitz SM. Infection due to Beta-lactamase producing, high level gentamicin resistant Enterococcus faecalis . Ann Intern Med 1992; 116: 285-92. Back to cited text no. 14 |
| 15. | Jesudason MV, Pratima VL, Pandian R, Abigail S. Characterisation of penicillin resistant enterococci. Indian J Med Microbiol 1998; 16 :16-8. Back to cited text no. 15 |
| 16. | Agarwal VA, Jain YI, Pathak AA. Concomitant high level resistance to penicillin and aminoglycoside in enterococci at Nagpur, Central India. Indian J Med Microbiol 1999; 17 :85-7. Back to cited text no. 16 |
| 17. | National Committee for Clinical Laboratory Standards: Performance standards for antimicrobial disk susceptibility test, 6th edn., Villanova, PA: NCCLS 1997;document M2-A6. Back to cited text no. 17 |
| 18. | Miles RS, Amyes SGB. Laboratory control of antimicrobial therapy, Chapter 8. In : Collee JG, Fraser AG, Marmion BP, Simmons A, editors. Mackie and McCartney Practical Medical Microbiology, 14th ed. London: Churchill Livingstone; 1996. p. 151-78. Back to cited text no. 18 |
| 19. | Lin RVTP, Tan AL. Enterococcus faecium with high level resistance to gentamycin. Lancet 1991; 338 :260-1. Back to cited text no. 19 |
| 20. | Havard CWH, Garrod LP, Waterworth PM. Deaf or Dead? A case of subacute bacterial endocarditis treated with penicillin and neomycin. BMJ 1959. Available at http://www.ncbi.nlm.nih.gov/entrez/query.fcgi? cmd = Retrieve & db = PubMed & list_uids = 13629091 & dopt = Abstract. 2005. Back to cited text no. 20 |
| 21. | Tompsett R, Pizette M. Enterococcal endocarditis: Lack of correlation between therapeutic results and antibiotic sensitivity tests. Arch Intern Med 1962; 109 :146-50. Back to cited text no. 21 |
| 22. | Krogstad DJ, Korfhagan TR, Moellering RC Jr., Wennersten C, Swarz MN, Perynski S, et al . Aminoglycoside-inactivating enzymes in clinical isolates of Streptococcus faecalis. An explanation for resistance to antibiotic synergism. J Clin Invest 1978; 62 :480-6. Available at http://www.pubmedcentral.nih.gov/articlerender.fcgi? tool = pubmed & pubmedid = 97312. 2005 Back to cited text no. 22 |
| 23. | Zimmermann RA, Moellering RC Jr., Weinberg AN. Mechanism of resistance to antibiotic synergism in enterococci. J Bacteriol 1971;105:873-9. Back to cited text no. 23 |
| 24. | Weinstein AJ, Moellering RC Jr. Penicillin and gentamicin therapy for enterococcal infections. JAMA 1973; 223 :1030-2. Back to cited text no. 24 |
| 25. | Livornese LL, Dias S, Samel C, Romanowski B, Taylor S, May P, et al . Hospital-acquired infection with vancomycin resistant Enterococcus faecium transmitted by electronic thermometers. Ann Intern Med 1992; 117 :112-6. Back to cited text no. 25 |
| 26. | Bhat KG, Paul C, Bhat MG. High level aminoglycoside resistance in enterococci isolated from hospitalized patients. Indian J Med Res 1997; 105 :198-9. Back to cited text no. 26 |
| 27. | Mohanty S, Kapil A, Das BK. Enterococcal bacteraemia in a tertiary care hospital of North India. JIMA 2005; 103 :31-7. Back to cited text no. 27 |
| 28. | Pfaller MA, Niles AC, Murray PR. Evaluation of Kirby-Bauer disc diffusion test as a screening test for high level aminoglycoside resistance in enterococci. Am J Clin Pathol 1984; 82 :458-60. Back to cited text no. 28 |
| 29. | Sahm DF, Torres C. Effects of medium and inoculum variations on screening for high level aminoglycoside resistance in Enterococcus faecalis. J Clin Microbiol 1988; 26 :250-6. Available at http://www.pubmedcentral.nih.gov/articlerender. fcgi? tool = pubmed & pubmedid = 3125217, 2005. Back to cited text no. 29 |
| 30. | Sahm DF, Torres C. High content aminoglycoside disks for determining aminoglycoside-penicillin synergy against Enterococcus faecalis. J Clin Microbiol 1988; 26 :257-60. Available at http://www.pubmedcentral.nih.gov/articlerender. fcgi? tool = pubmed & pubmedid = 3125218. 2005. Back to cited text no. 30 |
| 31. | Zervos MJ, Patterson JE, Edberg S, Pierson C, Kauffman CA, Mikesell TS, et al . Single concentration broth dilution test for detection of high level aminoglycoside resistance in enterococci. J Clin Microbiol 1987; 25 :2443-4. Available at http://www.pubmedcentral.gov/articlerender.fcgi? tool = pmcentrez & artid = 269516. 2005. Back to cited text no. 31 |
| 32. | Uttley AH, Collins CH, Naidoo J, George RC. Vancomycin resistant enterococci. Lancet 1988; 1 :57-8. Back to cited text no. 32 |
| 33. | Leclercq R, Derlot E, Duval J, Courvalin P. Plasmid mediated resistance to vancomycin and teicoplanin in Enterococcus faecium. N Eng J Med 1988; 319 :157-61. Back to cited text no. 33 |
| 34. | Montecalvo MA, Shay DK, Patel P, Tacsa L, Maleney SA, Jarvis WR, Wormser GP. Bloodstream infections with vancomycin resistant enterococci. Arch Intern Med 1996; 156 :1458-62. Back to cited text no. 34 |
| 35. | Purva M, Rama C, Benu D, Nidhi S, Lalit K. Vancomycin resistant Enterococcus bacteraemia in a lymphoma patient:Case report from India. Indian J Med Microbiol 1999; 17 :194-5. Back to cited text no. 35 |
| 36. | Bonten MJM, Slaughter S, Ambergen AW, Hayden MK, Voorhis JV, Nathan C, et al . The role of " Colonization pressure "in the spread of vancomycin resistant enterococci. Arch Intern Med 1998; 158 :1127-32. Available at http://archinte.ama-assn.org/cgi/content/abstract/158/10/1127? ijke = ef3ca5c9af3faf089637. 2005. Back to cited text no. 36 |
| 37. | Donskey CJ, Chowdhry TK, Hecker MT, Hoyen CK, Hanrahan JA, Hujer AM, et al . Effect of antibiotic therapy on the density of vancomycin resistant enterococci in the stool of colonized patients. N Eng J Med 2000; 343 :1925-32. Available at http://content.nejm.org/cgi/content/abstrac/343/26/1925? ijke = 5f3f77b722fe88a993ac0ec. 2005. Back to cited text no. 37 |
| 38. | Noskin GA, Stosor V, Cooper I, Peterson LR. Recovery of vancomycin resistant enterococci on fingertips and environmental surfaces. Infect Control Hosp Epidemiol 1995; 16 :577-81. Available at http://www.ncbi.nlm.nih.gov/entrez/query.fcgi? cmd = retrieve & db = pubmed & list_uids = 856. 2005. Back to cited text no. 38 |
| 39. | VanHorn KG, Gedris CA, Rodney KM. Selective isolation of vancomycin resistant enterococci. J Clin Microbiol 1996; 34 :924-7. Back to cited text no. 39 |
| 40. | Standiford HD, deMaine JB, Kirby WMM. Antibiotic synergism of enterococci. Arch Intern Med 1970; 126 :255-9. Back to cited text no. 40 |
| 41. | Wessels MR. Streptococcol and Enterococcal infections, Chapter 121. In : Kasper DL, Braunwald E, Fauci AS, Hauser SL, Longo DL, Jameson JL, editors. Harrison's Principles of Internal Medicine. 16th ed. New York: McGraw-Hill; 2005. p. 823-31. Back to cited text no. 41 |
| 42. | Bradley SJ, Wilson ALT, Allen MC, Sher HA, Goldstone AH, Scott GM. The control of hyperendemic glycopeptide resistant Enterococcus spp. on a haematology unit by changing antibiotic usuage. J Antimicrob Chemother 1999; 43 :261-6. Available at http://jac.oupjournals.org/cgi/content/abstract/43/2/261? ijkey = 549082fdb733b240e853ed8. 2005 Back to cited text no. 42 |
Copyright 2005 - Indian Journal of Medical Microbiology
The following images related to this document are available:
Photo images
[mb05068t1.jpg]
[mb05068t2.jpg]
|

{kind=link}
{kind=link}