 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
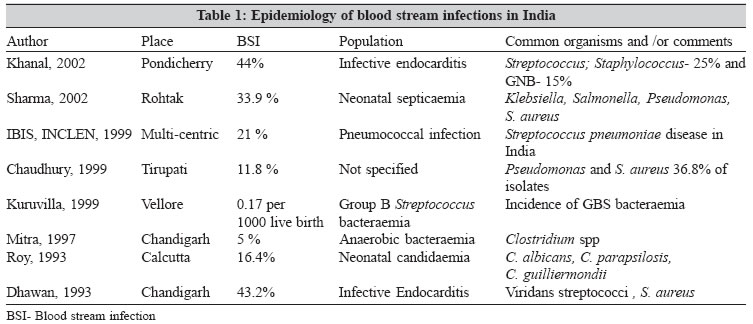
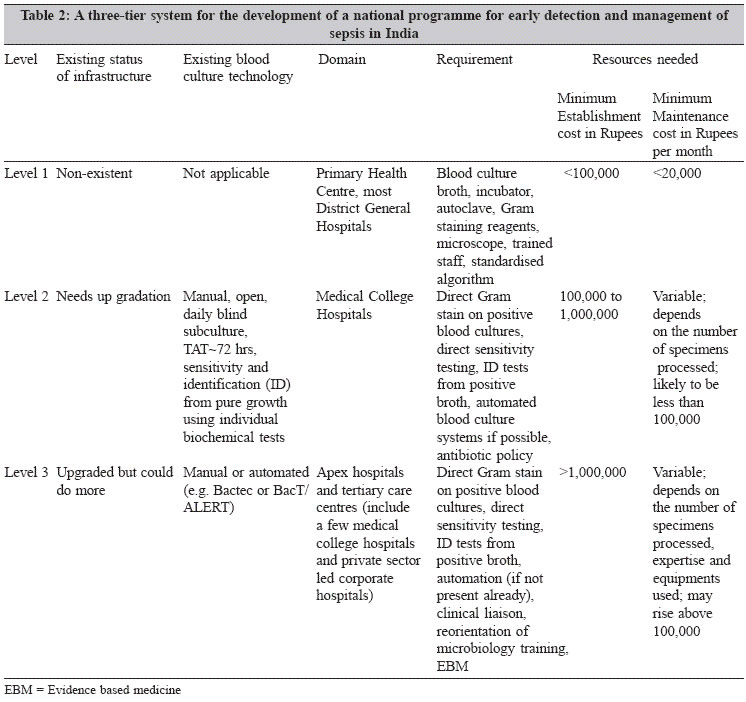
Indian Journal of Medical Microbiology, Vol. 23, No. 4, October-December, 2005, pp. 220-226 Special Article Blood culture in India: A proposal for a national programme for early detection of sepsis Bhattacharya S *Corresponding author (email: Code Number: mb05069 Abstract Septicaemia is a major contributor of mortality. Blood culture is the essential investigation for the management of sepsis. Due to lack of resources blood culture is an irregularly used investigation in India. A three-tier level of development is being proposed to develop the blood culture based national programme for early detection of sepsis. The plan envisages the establishment of manual blood culture based elementary system in the health centre and district hospital level (Level 1), direct Gram stain and direct antibiotic sensitivity testing from the "positive" blood culture broths at the medical college hospital level (Level 2) and development of automated methods, enhancement of quality control and safety measures, clinical liaison and re-orientation of microbiology training at the tertiary care centre level (Level 3).Keywords: Blood culture, India, direct susceptibility testing, turn around time, health economics Enhanced detection of blood stream infections needs to be a national priority. Early diagnosis and appropriate treatment of blood stream infections can make the difference between life and death. It would reduce mortality from septicaemia, reduce turnaround time and improve patient management. The challenges are to make this development sustainable- logistically, technically and financially. Considering India′s burden of mortality resulting from blood stream infections combined with financial resources, technical expertise and scientific know-how, a three-tier approach based on existing infrastructure, potential for development and future need looks both desirable and as well as realistically feasible. India has 187 medical colleges, 440 district hospitals, 2289 upgraded PHCs (primary health centres), 21,009 PHCs, 131,470 subcentres and 27,403 dispensaries. The hospitals and health centres in India harbour 870,161 public and private beds (Ministry of Health and Family Welfare, 2004).[1] In order to ensure an equitable, long-term and sustainable development it is important to think nationally and globally. Epidemiology of blood stream infections in India: morbidity and mortality A pre-requisite for the development of any meaningful programme to combat the problem of blood stream infection in India is to have an understanding of the magnitude of the problem afflicting us. If we look at the data published in the last 15 years from various centres in India [Table - 1] it becomes abundantly clear that the blood stream infection is a significant contributor of morbidity and mortality. Sharma et al from Rohtak in 2002 reported the incidence of bacteraemia to be 33.9% in neonates. Gram negative organisms (88.8%) like Klebsiella, Salmonella and Pseudomonas were most common followed by Staphylococcus aureus among the gram positives.[2] Chaudhury et al reported from Tirupati that the ratio of gram positive to gram negative bacteraemia was 1:1. S. aureus and P. aeruginosa taken together comprised 36.8% of their isolates.[3] Kuruvilla et al reported from Vellore that the incidence of Group B Streptococcal bacteraemia over a 10 year period was 0.17 per 1000 live births.[4] In the IBIS Group-INCLEN multi-centric study it was reported that 21% of the pneumococcal disease resulted in septicaemia. Intermediate resistance to penicillin was noted in 1.3% of the isolates; however, resistance to co-trimoxazole and chloramphenicol which are common antimicrobial agents used were common and seen 56% and 17% isolates respectively.[5] The microbiology of infective endocarditis in India has been documented in several studies. These include the one by Dhawan et al in Chandigarh in 1993 where 43.2% of the blood cultures were positive and as expected Streptococcus ′viridans′and Staphylococcus aureus where the commonest pathogens.[6] Khanal et al reported from Pondicherry that the incidence of gram negative bacillary (15%) and staphylococcal (25%) endocarditis was increasing. The appearance of MRSA and high-level gentamicin resistance associated endocarditis was found to complicate the management of endocarditis.[7] Not many studies have focussed on the epidemiology of anaerobic blood stream infections. The one by Mitra et al from Chandigarh describes that 5% of the symptomatic babies had infection with Clostridium spp.[8] Roy et al from Calcutta reported in 1993 an outbreak of neonatal candidaemia where 16.4% of the sick neonates had Candida blood stream infections (BSI).[9] Chakrabarti et al in 1992 reported from Chandigarh that the incidence of candidaemia increased eleven-fold during a study spanning 10 years.[10] Kumar et al in 1989 found 16.4% of the maternal deaths was due to puerperal sepsis in a rural community in northern India.[11] In another study from northern India spread over 16 years, sepsis was found to be responsible for 35.3% of the maternal deaths.[12] The leading causes of maternal death was sepsis (41.9%) in a study from Pondicherry by Rajaram et al in 1995.[13] Nosocomial sepsis was diagnosed in 21 out of a cohort of 134 (15.7%) newborn babies in hospitals in northern India. Multi-drug resistant Klebsiella species was the infectious agent in 68% of cases.[14] Making sense of the blood stream infection data in India A closer and holistic examination of all these epidemiological figures reveal certain interesting trends which could be made use of in designing diagnostic, clinical and infection control programmes. Infections, which can rapidly develop into life threatening sepsis and early death like septicaemia due to Enterobacteriaceae and Pseudomonas, are significant in the list of organisms causing sepsis. Staphylococcus aureus, which is notable for its ability to cause profound morbidity requiring long term, expensive management like in endocarditis, osteomyelitis, septic arthritis, deep seated abscesses and prosthetic device related infections is also among the most common organisms seen. This means that the early detection of these Gram negative organisms and their antibiotic susceptibility profiles can make a substantial difference in mortality rates and alter significantly neonatal, infant, childhood and maternal and other adult mortality and morbidity statistics. Similarly an early detection of Staphylococcal infections and MRSA would imply more appropriate use of antibiotics and prevention of life threatening complications of staphylococcal bacteraemia. This requires a new approach in diagnostic technology and standard operating procedures (SOPs)in India.[15] Most laboratories in India use blood culture SOPs in which the turn around time is not less than 72 hours and in some cases as long as five days. This makes the blood culture microbiology report a matter of academic interest in most cases and not a vital tool to save lives and diminish morbidity. The use of automated blood culture equipment, direct sensitivity[16] and identification testing from positive blood culture broths and urgent clinical liaison between the microbiology department and clinical team are essential if we want to make a difference in the struggle between life and death. Three-tier system in the diagnosis of blood stream infections: ground realities and future prospects Despite the enormous number of lives lost from sepsis, blood culture is an infrequent investigation done in most health care settings in India. This is because the culture of blood for the isolation, identification of microorganisms remains a technically challenging, financially demanding and man power intensive enterprise. Not many health centres in India possess the required infrastructure, manpower and money to support a diagnostic microbiology service. To overcome this problem various surrogate markers from haematology and biochemistry like total leukocyte count, C-reactive protein (CRP) level, erythrocyte sedimentation rate (ESR), presence of left shift or toxic granules in polymorphs have been used as markers of sepsis. The advantage of the surrogate markers is that they are sensitive indicators of sepsis, less expensive, rapid, and less labour intensive. However, the surrogate markers never tell us anything about the aetiology of sepsis, whether the sepsis in unimicrobial or polymicrobial, the antibiotic susceptibility, and they lack specificity in the setting of non-infective inflammatory processes such as trauma, ischaemia, collagen vascular disorders. Unless we go for the aetiologic diagnosis of infections our morbidity and mortality rates are unlikely to make a significant decline. It is true that sensitivity remains an important problem in blood culture. In a country like India, where antibiotics are available over the counter (OTC) without prescription, self-medication or injudicious medication is common. In these circumstances the probability of detecting bacteria in cases of sepsis is around 10% in most cases and 30% at the best. However, these figures can be improved by investing on training and practices, which favour early and pre-antibiotic sampling of blood cultures. Devices which facilitate growth of bacteria in blood cultures through the use of charcoal or ion-exchange resins (an inherent component of some automated blood culture monitoring system like Bactec) can improve the detection even further. Setting up of a microbiology laboratory with blood culture facility is a challenge in the rural health care setting. The options before us are to develop low cost, less labour intensive, rapid, low tech strategies. This is the rationale of the three-tier approach [Table - 2] where development is based on ground realities, existing infrastructure, potential for development and immediate needs. Level 1 Level 2 The objective of this paper is to bring about a change in diagnostic SOPs at this level so that the TAT is reduced by at least 24-48 hours and the first results start becoming available within 24 hours of the sample "signalling" positive. This can be made possible by direct Gram staining of all "positive" broths, performance of identification tests and antibiotic susceptibility testing (AST) directly from the positive broths without waiting for the isolation of pure colonies by sub-culture.[16] At the same time all efforts need to be made to make sure that clinically significant microbiology results like Gram stain findings from positive broths and presumptive identification and AST results are brought to the urgent and immediate attention of the responsible clinician either by telephonic communication, direct ward visit and entry in to patient′s clinical notes, or face to face discussion with clinical team members. Institutions and laboratories at this level should also make the necessary administrative, management, financial, training and technical decisions to see that equipment necessary for automated methods of blood culture (Bactec 9120/9240 or BacT/ALERT) are acquired at some point of time. Antibiotic policy for the empirical therapy for suspected sepsis needs to be developed for all medical colleges and nodal centres. Medical staffs (doctors) working in microbiology would require training in clinical microbiology (antibiotic advice, hospital infection control, appropriate methods of sampling and transportation of microbiology specimens). A standardised SOP (developed by the IAMM) may form the backbone of all departmental diagnostic microbiology services. Internal quality control must be an integral part of such SOPs and participation in External Quality Assurance has to become mandatory. The eventual target would be to bring all microbiology laboratories in the country under mandatory laboratory accreditation scheme. Non-compliance, non-performance should not be an option. Level 3 Unanswered questions It is obvious that provision of safe and efficient health care facility which includes the essential diagnostic services like blood culture in a vast country like India would require a colossal enterprise. It is a challenge as well as an opportunity. There are and would be several difficult questions to answer before we can make this ambitious enterprise a reality. Maintaining continuous resources- material, monetary and human- in the remote corners of the country may prove to be a logistical nightmare. Expert advice may be sought from institutions dealing with logistical support in difficult areas like the Indian Army to make this organisationally possible.[17] Lessons may have to be learnt from private sector initiative like the one by SRL - Ranbaxy which performs about 4 million tests a year (2002 data), supports a diagnostic laboratory network across 362 towns in India and wishes to increase the number of collection centres from 500 to over 2000. The SRL is now working on the prospect of business process outsourcing (BPO) of diagnostic tests.[18] Secondly, there is the problem of communication particularly in rural areas. Since, sepsis is a rapidly evolving life threatening condition, speed is the key to success, and this can only be achieved by the means of electronic communication. Currently, in India there are 51.9 fixed lines and mobile telephones per 1000 people (compared to 668/1000 in the USA, 580/1000 in the UK and 105/1000 in China), and only 7.2 personal computers per 1000 people and 6.7 internet users/1000 people (compared to 570/1000 in the USA and the UK, 35.5/1000 in China).[3],[19] Development of a national antibiotic policy, although highly desirable, is a very complex issue in itself. In most industrialised countries antibiotics are controlled drugs and are not available over the counter (OTC). It is desirable that all antibiotic prescriptions come from a physician and this will no doubt diminish the prevalence of antibiotic resistance. This is a sensible approach in a society where access to some form of health care is unrestricted. But there are large parts of India where locating a shop which sells medicine is easier than visiting a qualified doctor. Denying these individuals the right to buy antibiotics (a potentially life saving drug) over the counter, is basically denying them their right to life. This can raise serious moral and ethical dilemma. What is clear from these figures and facts is the reality that provision of health care infrastructure in a developing country is part of an over all social and economic development. The basic technology needed to provide this service is within our grasp. What we need is carefully calibrated organisational, administrative and political decisions so that the national priorities become focussed on health. It is not being recommended that blood cultures be taken in all ill patients. Instead it is emphasised that it should be taken where the surrogate markers and/or clinical judgement indicate to the possibility of sepsis. This will at least ensure that patients who need antibiotics get the most appropriate one. A crucial component of making any sector a national mission is to make it commercially viable and financially profitable. Purchase, lease and reagent rental are some of the commercial approaches used to acquire equipment and technologies. Implementing Blood culture services in India: an economic assessment India accounts for 16% of the world′s population and 21% of the world′s global burden of disease. Article 21 of the Constitution requires the State to ensure the health and nutritional well being of all people. The Central and State governments spend 0.9 % of the GDP on health. Three-quarters of the total health spending in the country is out of pocket (MOHFW, 2000).[20],[21] Therefore, the question is from where do we get the money to implement the changes that are being proposed in this paper in the scenario of differing priorities and low health expenditure on the part of the government. We need to impress upon the government that the present level of health expenditure is unacceptably low both in terms of internal resource allocation and in comparison to international standards. This policy must change in favour of health if we are to become a developed country. WHO′s Commission on Macroeconomics and Health, set up in 2000, concluded that development would not automatically occur in the developing world without increased investment in health. In response to this report in 2003 India had announced the formation of its own national commission on macroeconomics and health. The commission is co-chaired by India′s health and finance ministers.[22] This is just an acknowledgement of the problem but it has not been reflected in budgetary allocations in health. The WHO has laid out certain criteria for identifying the priority areas for work. These include a) Potential for significant change in burden of disease with existing cost-effective interventions, b) Health problems with major impact on socioeconomic development and a disproportionate impact on the lives of the poor, c) Urgent need for new technologies, d) Opportunities to reduce health inequalities within and between countries.[20] It is interesting that although the management of sepsis which contributes for the vast proportion of maternal and infant deaths fulfills most of these criteria, not much attention has been given to it in the WHO list of priority areas for India (Country Cooperation Strategy, India: WHO, 2000).[20] In spite of these imbalances there is some recent good news for the departments which specialise for laboratory services. The World Bank funded Integrated Disease Surveillance Project was approved on 8th July 2004 (the closing date is 31st March 2010). One of the four main objectives of this project is to improve laboratory support, upgrading laboratories at the state level, to improve laboratory surveillance activities. Support includes diagnosis, monitoring drug resistance, and changes in disease agents. In addition, a quality assurance system for assessing, and improving the quality of laboratory data will be introduced. The total cost for this project is $ 88.64 million in which the IDA (The International Development Association, World Bank Group) commitment is $ 68 million.[23] It is for India′s microbiological community now to make sure that this opportunity is not lost. Conclusions The MOHFW states that the National Health Programme (NHP) 2002 will endeavour to achieve certain time bound goals. One of them is to reduce IMR to 30/1000 live births and MMR to 100/100,000 live births by 2010. It is difficult to imagine how these targets would be achieved without tackling the problem of sepsis, which as discussed previously is the commonest contributor of infant and maternal deaths. The NHP-2002 also states that it endeavours to achieve certain other time bound goals. These include a) Increase health investment by Government as a % of GDP from the existing 0.9 % to 2.0% by 2010, b) increase central grants to constitute at least 25% of total health spending by 2010, c) increase state sector health spending from 5.5% to 7% of the budget by 2005 and to 8% by 2010. The departments of microbiology, infectious diseases and also all clinical departments who have a stake in the management of infections need to take a close and careful look at all such government declared targets. Economics is the study of choice and decision-making in a world with limited resources. It is up to the leaders in microbiology in India to ensure that economic decisions related to health care are made in their favour so that vital equipment, infrastructure, manpower are made available References
Copyright 2005 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb05069t2.jpg] [mb05069t1.jpg] |
| |||||||||
{kind=link}
{kind=link}