 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
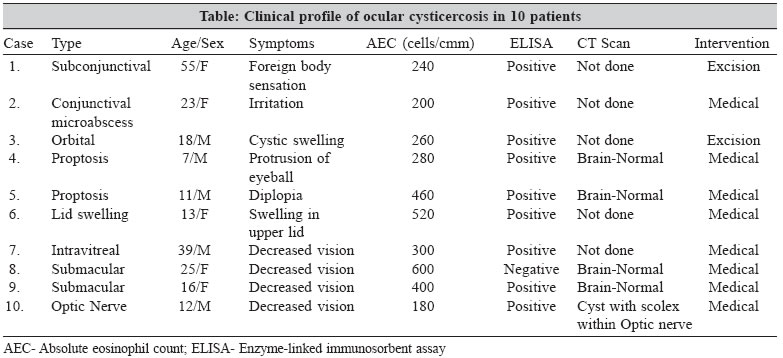
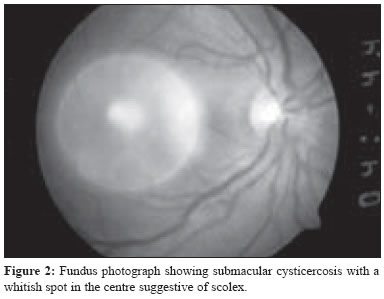
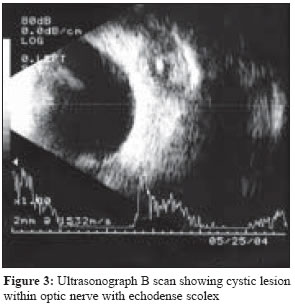
Indian Journal of Medical Microbiology, Vol. 23, No. 4, October-December, 2005, pp. 227-230 Original Article Cysticercosis of the eye in south India - A case series *Kaliaperumal S, Rao VA, Parija SC *Corresponding author (email: Code Number: mb05070 Abstract Purpose: To study the clinical presentation and treatment outcome of patients with ocular cysticercosis in southern India.Methods: This study included 10 patients who were diagnosed to have ocular or adnexal cysticercosis over a period of one year in Pondicherry, India. The clinical presentation, results of investigation and treatment outcome of the cases were analysed retrospectively. Results: Age of these patients ranged from 12 to 55 years. Four presented with loss of vision, two with a swelling in the eyelid, one with proptosis, one with diplopia and two with conjunctival involvement. ELISA for cysticercus antibodies in serum was positive in all cases. Albendazole and prednisolone were given for the treatment of these cases. Two patients responded well to treatment and were completely cured of the disease. There was partial improvement in 6 cases. Surgery in the form of excision was performed in two cases following a course of medical therapy. There was no significant change in visual acuity in eyes with intraocular cysticercosis following treatment. Conclusion: Ultrasonography B scan and ELISA for anticysticercal antibodies help to establish the diagnosis of ocular cysticercosis. A combination of oral albendazole and corticosteroids is found to be effective in confirmed cases. Intraocular cysticercosis is associated with a poor prognosis for vision. Keywords: Ocular cysticercosis, orbital, subconjunctival, ELISA, diagnosis Human cysticercosis is a parasitic infection caused by Cysticercus cellulosae , the larval form of the cestode, Taenia solium . Cysticercosis in humans is acquired by ingestion of faecally contaminated food, water or vegetables containing ova of T.solium . The condition is endemic in various parts of the world including Mexico, Africa, South East Asia, Eastern Europe, Central and South America and India. [1],[2],[3]Human cysticercosis predominantly affects the central nervous system causing neurocysticercosis and also the eye causing ocular cysticercosis.[4] In the present study, we report 10 cases of adnexal, orbital and intraocular cysticercosis seen in Pondicherry, India. The clinical manifestations, laboratory diagnosis and treatment of these cases were retrospectively reviewed with specific reference to the cases of ocular cysticercosis reported from other parts of India and abroad. Patients and methods A total of 10 patients who were diagnosed to have cysticercosis of the eye from April 2003 to March 2004 at JIPMER, Pondicherry, India, were included in the study.The age, gender and mode of presentation were recorded. Detailed ophthalmologic examinations including visual acuity, slit lamp biomicroscopy, direct and indirect ophthalmoscopy were performed for each eye. Hertel′s exopthalmometry and diplopia charting were done wherever required. Ultrasonography (A and B scan) was performed and clinical photographs were taken in all cases. A general physical examination was performed in all the cases to detect cysticercus if present in other parts of the body. A computerized tomography (CT) scan of the brain and orbit was carried out to rule out the possibility of neurocysticercosis and to supplement the diagnosis of ocular cysticercosis respectively. The serum from each patient was tested for cysticercus antibodies by enzyme linked immunosorbent assay (ELISA). The ELISA kit used was IgM ELISA, Novum Diagnostica. Other routine laboratory investigations included routine stool microscopy for intestinal parasites, ESR, total and differential leucocyte count, and absolute eosinophil count. A diagnosis of ocular cysticercosis was made based on ultrasonic or CT evidence of cyst with or without scolex and serum positivity for antibodies by ELISA. Medical management was initially given in all cases, which consisted of oral albendazole (15mg/kg/day) in two divided doses along with prednisolone (1.5mg/kg/day) in a single dose for four weeks. Oral prednisolone was tapered off over the subsequent four weeks. Surgical intervention was required in two cases. Results Of the 10 cases, five each were males and females. Age of these patients ranged from 12 to 55 years but majority (80%) were less than 25 years of age. Four patients presented with loss of vision, two with swelling of eyelid, one with proptosis, one with diplopia and two with irritation of eyes. Two cases with subconjunctival involvement had bilateral involvement of the eyes [Figure - 1] while the remaining cases had unilateral presentation [Table - 1]. CT scan of brain was normal in the five cases studied. Indirect ophthalmoscopy in one case (case 7) showed a free floating cyst in the vitreous cavity (5 disc diameters in size) while in two other patients (Case 8 and 9) a translucent cyst in the posterior pole with a intracystic whitish spot suggestive of scolex was demonstrated [Figure - 2]. One patient (Case 10) presented with no perception of light and mild prominence of left eye with optic neuritis like picture in that eye. Ultrasonography revealed cyst with scolex within optic nerve and a diagnosis of optic nerve cysticercosis was made [Figure - 3]. ELISA for serum antibodies was positive in all cases. Microscopy of stool did not reveal any Taenia eggs in any patient. Complete blood count was normal in all patients. Absolute eosinophil count ranged between 180 and 600 eosinophils per cubic millimeter. Medical treatment was fully effective in two cases while partial improvement was noted in the remaining. There was a dramatic response to medical treatment in one patient with optic nerve cysticercosis with patient regaining vision of 6/6 in one week. Another patient (Case 5) presenting with proptosis in right eye and diplopia in upgaze was treated elsewhere as a case of orbital pseudotumor on high dose steroids. With our treatment regimen, the proptosis decreased and diplopia improved [Table - 1]. Surgery in the form of excision was limited to two cases, one with orbital involvement and another with subconjunctival cysts following a course of medical therapy. Histopathological examination of the parasitic cyst in the excised cases revealed inflammatory reaction around the cyst wall composed of histiocytes, fibroblasts, neutrophils and eosinophils. There was no significant change in visual acuity in eyes with intraocular cysticercosis following treatment. Discussion Soemmering reported the first case of ocular cysticercosis in 1830. The larva was demonstrated and extracted by Schott in 1836.[5] Ocular or adnexal involvement occurs in 13-46% of infected patients. While the most common site of localisation reported in Western studies is the posterior, in the Indian literature the ocular adnexa is the most common site. [6],[7],[8]In a study reported by Kruger-Leite et al , 35% of the cysts were found in the subretinal space, 22% in the vitreous, 22% in the subconjunctival space, 5% in the anterior segment, and only 1% in the orbit.[9] In the present study of 10 cases of ocular cysticercosis, intraocular cysticercosis was the predominant form accounting for 40% of cases [Table - 1]. Of more than 500 cases collected in several series, about 4% occurred in the orbit or eyelids, 20% occurred in the subconjunctival area, 8% occurred in the anterior segment, 68% occurred in the posterior segment of which 41% either subretinally or intraretinally, while 27% occurred in the vitreous.[5] We found no predilection for either sex as in most other studies.[1],[7] The majority (80%)of our patients were less than 25 years of age. Reddy et al reported that 90% of their patients were less than 15 years of age;[8] Malik et al reported 68% in the age group of 10-30 years.[7] Cysticercosis in the eyelid is usually seen as a painless enlarging mass.[10] Subconjunctival lesions tend to present as hyperemic epibulbar masses that are sometimes fluctuant. Cysticerci may also be seen in the anterior chamber attached to the iris or on occasion to the anterior lens capsule. Cysticerci of the posterior segment are usually seen in the vitreous body[11] or in the subretinal space.[12],[13] The parasite is brought via the posterior ciliary arteries to the subretinal space usually in the region of the posterior pole. The subretinal cysts may vary in size from 3-6 disc diameters and have a single central scolex. Contraction and undulation of the cyst was seen periodically in two cases (Cases 6 & 7), which were accentuated by light. One patient (Case 7) had a full thickness macular hole; presumably this may be the entry site of the cyst into the vitreous cavity presenting as a translucent free floating cyst. The intravitreal cyst also had vitreous bands attached to it. Retinal pigment epithelial disturbances, retinal detachment, retinal oedema, intraretinal haemorrhage, and vascular sheathing are known to occur in intraocular cysticercosis.[14] The diagnosis of extraocular cysticercosis was largely speculative until the advent of advanced imaging modalities like ultrasonography and computed tomography. Intraocular cysticerci are easily diagnosed because of their visibility by ophthalmoscopy. High-resolution ultrasonography displays the characteristic picture of a sonolucent area with well defined anterior and posterior margins. The presence of a central echodense, curvilinear, highly reflective structure within the cyst suggestive of scolex, helps to narrow the differential diagnosis to cysticercosis as the aetiological cause.[15] Computerised Tomography scan not only confirms the diagnosis but helps to rule out neurocysticercosis. Though CT scan is advisable in all cases, it could not be done in five cases of our series due to economic constraints. Presence of a cystic lesion without a scolex with positive ELISA for anticysticercal antibodies is also diagnostic. Enzyme-linked immunosorbent assay (ELISA) to detect the antibody to cysticerci has been reported to be positive in 61% to 79% of cases of neurocysticercosis.[16] In our series, ELISA was positive in all 10 cases. Histopathological examination of eye lesions in cysticercosis shows an inflammatory reaction about the cyst wall composed of three distinct layers: the outermost zone formed by dense fibrovascular connective tissue, a middle layer showing large histiocytes intermingled with fibroblasts, and an inner layer containing neutrophils and eosinophils. The scolex with suckers and double row of hooklets is a prominent feature.[10] The differential diagnosis of ocular cysticercosis is hydatid cyst, which rarely affects the eye. Hydatid cysts of the eye are larger and mostly require surgical excision. The other important differential diagnosis especially with the presentation of painful inflammatory proptosis with restricted ocular motility is orbital pseudotumor or idiopathic myositis. Neurocysticercosis has been treated successfully with albendazole and with praziquantel.[17],[18] Sotelo et al have compared the two drugs and found albendazole to be more effective than praziquantel and also less expensive.[17] All the patients in the present study received a combination of oral albendazole and corticosteroids for 4-6 weeks. Oral steroids are recommended along with cysticidal drugs to control the inflammation elicited by the dying cyst. Surgery in orbital and intraocular cysticercosis is accompanied with complications and does not yield gratifying results in most cases. In orbital cysticercosis, the cyst may be attached to important orbital structures and surgical excision may cause postoperative fibrosis resulting in restrictive ocular motility.[19] The most devastating location is intraocular. Pars plana vitrectomy has been proved to be an ideal operative procedure for intravitreal cysticercosis. Though subretinal cysts can be removed by an intravitreal or transscleral approach, the results are not very good. In conclusion, a high index of suspicion is required for the diagnosis of ocular cysticercosis because of the endemic nature of this infestation in this geographic location. Ultrasonography B scan and ELISA for anti cysticercal antibodies help to establish the diagnosis. A combination of oral albendazole and corticosteroids is given in confirmed cases. Intraocular cysticercosis is associated with a poor prognosis for vision. References
Copyright 2005 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb05070t1.jpg] [mb05070f1.jpg] [mb05070f3.jpg] [mb05070f2.jpg] |
| |||||||||
![Figure - 1]](/showimage?mb/photo/mb05070f1.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}