
|
Indian Journal of Medical Microbiology
Medknow Publications on behalf of Indian Association of Medical Microbiology
ISSN: 0255-0857 EISSN: 1998-3646
Vol. 23, Num. 4, 2005, pp. 231-238
|
Indian Journal of Medical Microbiology, Vol. 23, No. 4, October-December, 2005, pp. 231-238
Original Article
Granulomatous inflammation in acanthamoeba keratitis: An immunohistochemical study of five cases and review of literature
*Vemuganti GK, Pasricha G, Sharma S, Garg P
*Corresponding author (email:)
Department of Ophthalmic Pathology Service(GKV), Jhaveri Microboogy Centre
(GP, SS) and Cornea Services (PG), L V Prasad Eye Institute, L V
Prasad Marg, Banjara Hills, Hyderabad- 500
034, India
Code Number: mb05071
Abstract
Purpose: Acanthamoeba keratitis usually presents as a necrotizing stromal inflammation. We report a rare presentation of granulomatous inflammation in Acanthamoeba keratitis
Methods: Retrospective clinico-pathologic case series.
Results: Five corneal tissues (3 corneal buttons, 2-eviscerated contents) from patients suffering from severe Acanthamoeba keratitis not responding to anti-Acanthamoeba treatment, revealed a florid granulomotous inflammation with multinucleated giant cells in the posterior stroma and around Descemet's membrane. Phagocytosed parasites were noted within the giant cells. Vascularization of the corneal stroma was noted in two cases. Immunophenotyping revealed a predominance of T lymphocytes and macrophages. Clinically, four of five cases had shown features of limbal and scleral involvement.
Conclusion: Granulomatous inflammation in the posterior corneal stroma, is not an uncommon finding in Acanthamoeba keratitis and could possibly be immune-mediated, contributing to persistence and progression of disease.
Clinical Relevance: Presence of granulomatous inflammation in Acanthamoeba
keratitis, in most cases is associated with limbal and scleral involvement
and therefore could be considered as one of the poor prognostic markers.
Further studies are required to ascertain the specific clinical features
and appropriate management strategies in these cases.
Keywords: Acanthamoeba keratitis, Granulomatous inflammation, sclertitis, immunophenotyping
Acanthamoeba keratitis is a rare infection of the cornea caused by free-living amoeba. [1],[2],[3]The infection is characterized by stromal keratitis, ring-shaped stromal infiltrates, severe pain and rarely involvement of episclera. [4],[5]Medical cure, if diagnosed early, is obtained by the use of one or more drugs which include propamidine isethionate, polyhexamethylene biguanide (PHMB), chlorhexidine, clotrimazole and a judicial use of corticosteroids. [6],[7],[8],[9],[10]However in severe cases, not responding to adequate medical treatment, surgical intervention in the form of penetrating keratoplasty or evisceration is undertaken. [11],[12]The histologic changes observed in Acanthamoeba keratitis include, epithelial ulceration, stromal inflammation and necrosis, presence of cysts and trophozoites of Acanthamoeba , [13],[14],[15]apoptosis of keratocytes[16] and rarely granulomatous inflammation of the corneal stroma.[17] We herein report clinical, histologic and immunohistochemical features in five cases of Acanthamoeba keratitis with granulomatous inflammation presenting clinically as severe, rapidly progressive disease involving the limbus and the sclera.
Materials and Methods
In this retrospective study of cases, the corneal buttons of microbiologically diagnosed cases of Acanthamoeba keratitis submitted to the Ophthalmic Pathology Service and showing features of granulomatous inflammation were reviewed and evaluated further as described below.
Clinical
The standard protocol of treatment for microbiologically diagnosed
cases of Acanthamoeba keratitis
at our Institute is as follows: 0.02% PHMB (Baquasil, ICI, USA) and 0.02% chlorhexidine
digluconate (Sigma, C-9394) instilled half hourly for 2-3 days (day and
night) and then one hourly for period of 7 days. Subsequently, according
to clinical response to treatment, the frequency of biguanides is reduced
to 3 to 4 hourly per day and then continued for 2-3 weeks after resolution
of inflammatory signs. The patients are observed daily or weekly for
few weeks. Decision for surgical intervention is taken if: 1) there is
large infiltrate at presentation, 2) progression of the disease despite
the initiation of anti- Acanthamoeba treatment for 2 weeks 3)
If there is involvement of limbal region, 4) impending perforation. We
evaluated medical and microbiology records of these cases, and noted
the clinical picture at the time of presentation, medical treatment and
its duration and the indication for surgical intervention.
Microbiology
Corneal scrapings from all patients had been subjected to smear
examination by three methods, viz., potassium hydroxide with calcofluor
white, Gram and Giemsa stains and culture on media for bacterial and
fungal growth along with nonnutrient agar with live Escherichia coli overlay
for growth of Acanthamoeba . Corneal buttons, whenever available
for microbiologic studies, were processed for bacteria, fungi and Acanthamoeba by
culture of tissue homogenate on blood agar, chocolate agar, brain heart
infusion broth, Sabouraud dextrose agar and nonnutrient agar with E.coli.
Paraffin sections of corneal buttons and evisceration materials
were used for extraction of DNA by a procedure described earlier[18] and
were tested for presence of herpes simplex virus DNA by polymerase chain
reaction,[19] using primers
specific for glycoprotein D gene of herpes simplex virus. Results of
microbiological investigations for all cases is shown in [Table
- 1].
Histopathology
Keratectomy/eviscerated material was fixed in 10% buffered formalin. Multiple sections of 5µ thickness were cut from paraffin embedded tissues. Sections were deparaffinized by placing the slides in the oven at 51°C for 1 hour, followed by immersion in xylene and hydration in decreasing ethanol concentration. Hematoxylin - eosin staining, periodic acid Schiffs and Gomori′s
methenamine silver staining were performed on these tissue sections.
Immunophenotyping
Immunohistochemistry was performed using monoclonal mouse anti-human
antibodies (Dako, Denmark) against, T cell CD 3, Macrophage CD 68 and
B cell CD 20 antigen. After deparaffinizing the sections, the endogenous
peroxidase acitivity was neutralized using 100% methanol and 0.4% H2O2.
Antigenic epitopes of the corneal section were retrieved by incubating
the sections with prewarmed citrate buffer for 15 minutes in hot air
oven maintained at 100°C. Non-immunologic binding of antibodies was blocked by incubation with bovine serum albumin. Incubation with all the primary antibodies was carried out in a moist chamber at 4°C overnight. On the following day after thorough washing with phosphate buffer saline, secondary biotinylated goat anti-mouse antibody (Dako, Denmark) was added and incubated at room temperature in moist chamber for 30 minutes. This was followed by incubating the sections with avidin-biotin complex wherein the biotin was conjugated with horseradish peroxidase enzyme (Dako, Denmark) for 45 minutes. The peroxidase activity was visualized by incubation with freshly prepared 3 3′ Diaminobenzidine tetrahydrochloride (DAB) containing 0.0015% H2O2.
The slides were counterstained with hematoxylin, dehydrated and cleaned
in xylene and mounted. Corneal button section, without the incubation
with primary antibody was used as negative control, while tonsil section
served as positive control. The phenotype of the inflammatory cells was
assessed in the region of the granulomatous inflammation, surrounding
stroma and limbus.
Results
Clinical profile
Of the 172 cases of Acanthamoeba keratitis diagnosed in our
institute from 1995 till May 2003, 18 (10.4%) underwent surgical intervention in the form of penetrating keratoplasty or evisceration. Five of these eighteen keratectomy specimens (27.7%)
displayed granulomatous cell reaction. Five patients included 3 males and
2 females and their age at the time of surgery ranged from 20 - 65 years
(median 45 years). Two patients underwent evisceration while the other
three had penetrating keratoplasty done.
Case 1
A 30-year-old male patient presented with complaints of pain, redness,
watering and decreased vision of two months duration following an injury
to the eye while working in the fields. He was diagnosed as a case of ring
corneal ulcer and treated with antibiotic eye drops for two months before
being referred to our institute. At presentation, he had a vision of hand
movements at 2 meters with inaccurate projection of light. The conjunctiva
was congested. Cornea showed a ring ulcer [Figure
- 1] involving
the limbus at the entire periphery. Fundus could not be visualized. B scan
revealed choroidal thickening with no gross vitreous opacities. Corneal
scrapings revealed 0-4 cysts of Acanthamoeba per high power field.
Patient was diagnosed as Acanthamoeba keratitis and treated with
chlorhexidine and PHMB for a period of one month. There was progression
of the ulcer, marked thinning and ectasia of cornea with impending perforation.
Prognosis of the condition was explained to the patient and was advised
for evisceration. The excised contents were subjected to histologic examination.
Case 2
A 65-year-old female who underwent uncomplicated penetrating keratoplasty
with extracapsular cataract extraction and posterior chamber lens implantation
in her right eye for granular dystrophy presented to her ophthalmologist
three months post-operatively complaining of pain, photophobia, and decreased
vision. The ophthalmologist diagnosed her condition as graft rejection
based on the presence of a raised concentric epithelial line on the donor
cornea, diffuse stromal edema and multiple keratic precipitates on the
endothelium. She was treated with hourly topical prednisolone acetate.
After three days of therapy the epithelial line increased in size and developed
areas of epithelial defect. The surgeon suspected recurrent HSV keratitis,
therefore reduced the frequency of prednisolone acetate and started topical
acyclovir (5%) 5 times a day. When there was no improvement in the patient′s
condition, he referred the case to us. At initial examination at our institute
her visual acuity was hand movements in the right eye and 20/125 in the
left eye. The conjunctiva was injected. Cornea showed two circumferential
epithelial defects, about 2 mm inside the graft host junction, associated
with granular infiltrate [Figure - 2].
Rest of the graft showed diffuse stromal haze associated with multiple
keratic precipitates. The host cornea demonstrated minimal superficial
vascularization and all interrupted sutures were intact. Anterior chamber
was deep and the intraocular pressure appeared normal on digital tonometry.
Microscopic examination and culture of the corneal scrapings were positive
for Acanthamoeba .
A review of the patient′s medical and social history revealed she was using pond water for washing face and taking bath. The patient was treated with half hourly topical PHMB 0.02% and chlorhexidine 0.02% and
oral itraconazole 100mg twice daily. When the clinical picture did not
improve a therapeutic penetrating keratoplasty was done after 2 weeks;
the excised corneal button was subjected to histopathology examination.
On the first post operative day, there were exudates in the anterior chamber.
There was evidence of suture abscess, epithelial defect and endothelial
pigments on the 7th post-operative which progressed to scleral abscess
at the end of 5 weeks [Figure - 3].
The final visual acuity at the end of 6 weeks was perception of light.
Case 3
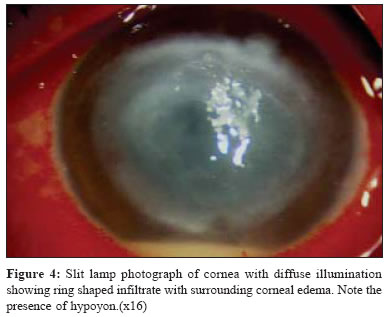
A 45- year- old man presented with severe pain, redness, watering,
pricking sensation and reduced vision of 10 days duration. He gave a history
of sand particles falling into his eye while digging pits in the farm.
He consulted a local ophthalmologist who diagnosed as hypopyon corneal
ulcer [Figure - 4] and
referred to our institute for further treatment. On examination, he had
edema of lids with pseudoptosis. Conjunctiva was congested and chemosed.
Cornea showed an epithelial defect 2 x 2.5mm associated with underlying
stromal infiltrates of 8mm. Anterior chamber was deep with 1mm hypopyon.
Initial corneal scrapings did not reveal any organisms on microscopic examination
of smear while a repeat scraping revealed cysts of Acanthamoeba .
The patient was treated for five weeks with PHMB and chlorhexidine eye
drops along with oral itraconazole. There was no response to the above
medication. On the contrary, the ulcer expanded to involve the limbus and
the sclera with increase in intraocular pressure. In view of advanced disease,
not responding to medical treatment, an evisceration was performed after
obtaining consent from the patient.
Case 4
A 20-year-old female presented to us with the complaints of pain,
redness, watering, photophobia and diminished vision in her left eye of
two and half months duration. She gave history of unknown particles falling
into her eyes while washing clothes. At the time of presentation, the visual
acuity in her affected eye was light perception and accurate projection
of rays in all quadrants. Intraocular pressure was normal on digital tonometry.
On examination the left eye showed a ring shaped corneal infiltrate 1mm
inside the limbus. The corneal stroma within the ring showed a granular
infiltrate. Surrounding cornea was edematous with deep vascularization
in two quadrants. Anterior chamber was deep. Posterior segment appeared
normal on B-scan ultrasonography.
Corneal scrapings revealed Acanthamoeba cysts on microscopic
examination. The patient was treated with topical 0.02% PHMB and 0.02% chlorhexidine instilled half hourly, atropine sulphate 1% instilled thrice daily and oral ketoconazole 200 mg twice daily. Over the next 10 days the infiltrate increased in density and showed progressive vascularization. We added prednisolone acetate 1% every
three hourly. With this therapy the central infiltrated area showed progressive
thinning. Therefore, we advised penetrating keratoplasty. The
corneal tissue removed during keratoplasty was divided in to two halves;
one submitted in saline for microbiology work-up and the other half in
formalin for histopathology examination. At the end of 6 weeks, the graft
was clear with a visual acuity of 20/50 in the left eye.
Case 5
A 58-year male patient presented to us with the complaints of pain,
redness, watering, and reduced vision in his left eye on 1month duration.
He gave a history of dust/wooden particles falling into his eyes while
cutting wood. He was treated with 3-hourly instillation of fluconazole
(0.3%), natamycin 5%, ciprofloxacin HCl (0.3%) before presenting to us. At the time of presentation visual acuity was counting fingers close to face in the affected eye. The cornea showed a central 8.1 mm x 5.1mm epithelial defect with a ring infiltrate measuring 6 x 5mm and surrounding cellular reaction. The stroma within the ring showed 50% thinning.
Anterior chamber was deep with 2mm hypopyon. B-scan ultrasonography showed
an echo-free vitreous cavity with attached retina. Initial corneal scraping
did not reveal any organisms on microscopy or on culture. However, the Acanthamoeba cysts
were seen on microscopic examination and cultured on repeat scrapings.
The patient was treated with 0.02% chlorhexidine and PHMB for 11
days. Despite treatment, the infiltrate finally progressed and extended
to involve the limbus between 10 to 2 clock hours. Therefore, penetrating
keratoplasty was performed. The corneal button was subjected for microbiology
and histopathology evaluation. Four weeks post operatively the vision in
the left eye was 20/60 with a clear graft.
Microbiology
The results of smear and culture of clinical samples from all five
cases are shown in [Table - 1].
Histopathology
The histopathologic features of the five cases are given in [Table
- 2].
There was epithelial ulceration with destruction of Bowman′s layer
in all the cases. The stroma showed inflammatory infiltrates consisting
of neutrophils in the anterior two-thirds of stroma [Figure
- 5].
Vascularization of stroma was noted in mid and deep peripheral stroma in
two cases. Viable and degenerated cysts of Acanthamoeba were seen
in the stroma [Figure - 6].
In addition, the deeper stroma and the region around Descemets membrane
showed a few aggregates of epitheloid cells, lymphocytes and multinucleated
giant cells [Figure - 7].
Some of the giant cells and occasional keratocytes showed cysts of Acanthamoeba in
the cytoplasm [Figure - 8],
suggesting the phagocytosed parasites. Limbal tissue, when identified in
the sections, showed dense lymphoplasmacytic infiltrates admixed with few
eosinophils.
Immunophenotyping
The inflammatory cells in the corneal stroma were found to be of
T cell population. In the granulomatous regions, the cells were positive
for T cells [Figure - 9],
CD 68 [Figure - 10] and
negative for B-cell marker, suggesting a predominance of T lymphocytes
with macrophages. The detailed results are depicted in [Table
- 2].
Discussion
Acanthamoeba keratitis is a vision-threatening infection caused
by pathogenic species of the genus Acanthamoeba . The amoebae are
often introduced in the eye by an individual′s use of contaminated
contact-lens cleaning solutions, trauma or by swimming in contaminated
water.[21] Acanthamoeba keratitis
usually results from direct invasion of ocular tissue by the amoeba through
minor breaks in the corneal epithelium, caused by trauma, previous episodes
of herpes simplex or by abrasion from hard or soft contact lenses.[2] The
pathogenesis of Acanthamoeba keratitis involves parasite-mediated
cytolysis and phagocytosis of corneal epithelial cells,[22] invasion
of the extracellular matrix, keratocyte depletion, recruitment of inflammatory
infiltrates and dissolution of the corneal stromal matrix.[13]
Histologically, the corneal tissues in Acanthamoeba keratitis show evidence of epithelial ulceration, polymorphonuclear infiltrates, stromal necrosis along with the presence of trophozoites and/or cysts in the corneal stroma.[13] Despite the prolonged clinical course of the disease, a few unique observations have been made in Acanthamoeba keratitis which include: absence of vascularization,[14] scarcity of lymphocytes,[13] keratocyte loss through apoptosis, and the presence of cysts in the deep stroma, unaccompanied by inflammatory cells.[16] Though acanthamoebic infections of brain usually evoke granulomatous inflammation,[23] this is rarely reported in Acanthamoeba keratitis. We herein report five cases of Acanthamoeba keratitis presenting with granulomatous inflammation in the posterior corneal stroma, four of which presented with rapidly progressing Acanthamoeba keratitis involving limbus and sclera. To understand the significance of these findings we performed the immunophenotyping of the inflammatory cells and attempted a clinicopathological correlation.
Clinically, Acanthamoeba keratitis is characterized by severe
pain with an early superficial keratitis, followed by radial perineural
infiltration, ring infiltration and rarely limbitis and scleritis.[4] Sclerokeratitis
in Acanthamoeba keratitis is often associated with severe inflammtion
and is a therapeutic challenge to the ophthalmologist. The limbal and
scleral inflammation has been reported to increase on initial intensive
topical antiamoebic therapy and this has been related to immune mediated
response to dead or dying amoebae within the cornea. Fortunately limbal
and scleral extension of Acanthamoeba keratitis remains a rare
complication. None of the patients in our earlier reported series of
39 patietns had developed this complication.[5] Three
of five cases reported in this series had a severe clinical course that
progressed despite adequate doses of supervised medical treatment, necessitating
surgical intervention. One case presented with total corneal ulcer, while
the other presented as a graft infiltrate, clinically mimicking a rejection
phenomenon. The median duration of medical treatment was 2 weeks (1-
8 weeeks). History of trauma was elicited in 4 cases. Though prolonged
medical treatment is usually advised for Acanthamoeba keratitis,
penetrating keratoplasty has been advocated in cases which threaten the
integrity of the eye.[11] At
our institute, 10.4% (18 of 172) of cases underwent surgical intervention in the form of keratoplasty in 72% (13 of 18) and evisceration in 28% (5
of 18).
Histologically, the tissues showed epithelial ulceration and destruction
of Bowman′s layer. The stroma showed dense inflammatory infiltrates
predominantly consisting of polymorphonuclear infiltrates in all cases,
as was reported in most studies. [13],[14],[15] The
deeper stroma showed lymphocytes, macrophages, epitheloid granulomas and
giant cells. Though polymorphonuclear cells are believed to be the first
line of defense in all infections, including Acanthamoeba keratitis,
recent evidence however points towards the role of macrophages.[24] Van
Klink et al performed conjunctival macrophage depletion in chinese
hamsters to determine the importance of macrophages in Acanthamoeba keratitis.
They selectively eliminated macrophages using macrophagicidal drug dichloromethylene
diphosphate. They found profound exacerbation of Acanthamoeba keratitis
in hamster treated with this drug, strongly suggesting that macrophages
play an important role in the corneal infection with Acanthamoeba ,
probably by acting as a first line of defense and eliminating significant
numbers of Acanthamoeba trophozoites.[24]
Two of the five cases showed evidence of vascularization in our series.
This is different from the observations made by Kremer et al[14] who
noted the conspicuous absence of vascularization in 10 cases reported by
them. In general, it is believed that lymphocytic infiltration in the cornea
is closely associated with vasculatization.[25] When
vascularization is present, lymphocytic and plasmacytic infiltrates are
usually observed mainly in the immediate vicinity of blood vessels in the
corneal stroma or in the vascular pannus. An immune response to chronic
inflammation can be expected to further involve macrophages, lymphocytes
and macrophage derived epitheloid cells.[25]
Garner interpreted that absence of lymphoid cell may be due to absence
of stromal vascularization and consequent barrier to invasion by relatively
immotile cells.[13] In all
our cases, lymphomononuclear cells were noted in the deep stroma accompanied
by macrophages, epitheloid cells and multinucleated giant cells. Though
Auran et al in their review article of 35 cases interpreted the
presence of granulomatous inflammation in 5 cases,[23] best
illustration of this finding was reported by Meitz et al in 1997.[17] Granulomatous
inflammation extending to sclera has been reported by Doughtery et al . [26] In
the two eviscerated tissues, there was no evidence of granulomatous inflammation
in the sclera or other layers.
The frequency of granulomatous inflammation in corneal tissues varies
from 2% to 25% depending on the type of tissues included in the
study. [27],[28],[29] It
was reported in 2% (6 of 314) of all keratoplasty specimens,[27] 9% (28/298)
in infectious keratitis of all causes,[28] and
25% (53 of 215) of keratectomy specimens from patients with a clinical
diagnosis of herpes stromal keratitis.[29] We
reported granulomatous inflammation in 13.8%(23 of 167) of fungal
keratitis[30] and now report
27.7 % (5 of 18) in Acanthamoeba keratitis. Though it can
be seen in various other infectious and non-infectious corneal diseases,
there is enough evidence that it is most commonly associated with disciform
herpes simplex keratitis.[29] In
this study, the DNA isolated from the paraffin sections of the corneal
tissue were negative for herpes simples virus DNA, thereby ruling out any
associated or pre-existing herpes virus keratitis.
Granulomatous inflammation is a type of chronic inflammation characterized
by the collection of modified macrophages, namely the epitheloid cells
with or without associated multinucleated giant cells and lymphocytes.
Though definite pathogenesis of the granulomatous reaction in general
remains unknown, the process may have a non-immune or immune aetiology.[27] The
non-immune response is the well known foreign body granuloma. There is
an influx of macrophages due to chemotaxis and these cells persist in
the area if the foreign material is poorly soluble.[31] The
immune pathway is the result of sensitized T cells releasing lymphokines
and causing the accumulation of macrphages.[32] The
presence of T lymphocytes as found in this study suggests that granulomatous
inflammation in cornea appears to be an immune-mediated process. These
T cells could either be sensitized to microbial antigens, altered cellular
and/or basement membrane structures from the host, or both. Holbach et al[29] support
the role of viral antigens while Weiner et al suggest a non-viral
antigen in the etiopathogenesis of this type of inflammation.[27] Though
the clinical implications of this type of inflammation is not clearly
documented, it has been suggested that granulomatous inflammation around
Descemets
membrane can be identified clinically and should be considered as an
indication for penetrating keratoplasty in herpes stromal keratitis.
We speculate
that it may be the same for Acanthamoeba keratitis. What is important
to note is that all four of five cases had a rapid clinical worsening
with extension of the inflammation to the limbus, with involvement of
sclera
in four cases, necessitating an early surgical intervention, suggesting
the possibility that it could be a poor prognostic maker. However, whether
the granulomatous inflammation is the cause or the effect of the advanced
disease cannot be commented upon by these five cases but it is likely
that the two are related.
To summarize, granulomatous inflammation, is not an uncommon finding
and could be seen in rapidly progressing form of Acanthamoeba keratitis,
not responding to medical treatment. Further studies are warranted
to understand the varied presentation of this disease and its clinical
implication.
References
| 1. | Visvesvara GS, Stehr-Green JK. Epidemiology of free-living ameba infections. J Protozool 1990; 37 :25S-33S. Back to cited text no. 1 |
| 2. | Stehr-Green JK, Bailey TM, Visvesvara GS. The epidemiology of Acanthamoeba keratitis in the United States. Am J Ophthalmol 1989; 107 :331-6. Back to cited text no. 2 |
| 3. | Radford CF, Lehmann OJ, Dart JKG. Acanthamoeba keratitis: Multicentre survey in England 1992-1996. Br J Ophthalmol 1998; 82 :1387-92. Back to cited text no. 3 |
| 4. | Bacon AS, Frazer DG, Dart JKG, Matheson M, Ficker LA, Wright P. A review of 72 consecutive cases of Acanthamoeba keratitis, 1984-1992. Eye 1993;7:719-25. Back to cited text no. 4 |
| 5. | Sharma S, Garg P, Rao GN. Patient characteristics, diagnosis and treatment of non-contact lens related Acanthamoeba keratitis. Br J Ophthalmol 2000; 84 :1103-8. Back to cited text no. 5 |
| 6. | Illingworth CD, Cook SD. Acanthamoeba keratitis. Surv Opthalmol 1998; 42 :493-508. Back to cited text no. 6 |
| 7. | D'Aversa G, Stern G, Driebe WT. Diagnosis and medical treatment of Acanthamoeba keratitis. Arch Ophthalmol 1995; 113 :1120-3. Back to cited text no. 7 |
| 8. | Lindquist TD. Treatment of Acanthamoeba keratitis. Cornea 1998;17:11-6. Back to cited text no. 8 |
| 9. | Park DH, Palay DA, Daya SM, Stulting RD, Krachmer JH, Holland EJ. The role of topical corticosteroids in the management of Acanthamoeba keratitis. Cornea 1997; 16 :277-83. Back to cited text no. 9 |
| 10. | McClellan K, Howard K, Niederkorn JY, Alizadeh H. Effect of steroids on Acanthamoeba keratitis. Invest Opthalmol Vis Sci 2001; 42 :2885-93. Back to cited text no. 10 |
| 11. | Cohen EJ, Parlato CJ, Arentsen JJ, Genrert, Eagle Jr RC, Wieland MR, et al . Medical and surgical treatment of Acanthamoeba keratitis. Am J Ophthalmol 1987; 103 :615-25. Back to cited text no. 11 |
| 12. | Illingworth CD, Cook SP, Karabatsas CH, Easty DL. Acanthamoeba keratitis: risk factors and outcome. Br J Ophthalmol 1995; 79 :1078-82. Back to cited text no. 12 |
| 13. | Garner A. Pathogenesis of Acanthamoeba keratitis: hypothesis based on a histological Analysis of 30 cases. Br J Opthalmol 1993; 77 :366-70. Back to cited text no. 13 |
| 14. | Kremer I, Cohen EJ, Eagle RC Jr, Udell I, Laibson PR. Histopathologic evaluation of stromal inflammation in Acanthamoeba keratitis. CLAO J 1994; 20 :45-8. Back to cited text no. 14 |
| 15. | Yang YF, Matheson M, Dart JK, Cree IA. Persistence of Acanthamoeba antigen following Acanthamoeba keratitis. Br J Ophthalmol 2001;85:277-80. Back to cited text no. 15 |
| 16. | Vemuganti GK, Sharma S, Athmanathan S, Garg P. Keratocyte loss in Acanthamoeba keratitis: Phagocytosis, necrosis or apoptosis? Indian J Ophthalmol 2000; 48 :291-4. Back to cited text no. 16 |
| 17. | Mietz H, Font RL. Acanthamoeba keratitis with granulomatous reaction involving the stroma and anterior chamber. Arch Ophthalmol 1997; 115 :259-63. Back to cited text no. 17 |
| 18. | Chomczynsky P, Mackey K, Drews R, Wilfinger W. DNAzol: A reagent for the rapid isolation of genomic DNA. Biotechniques 1997; 22 :550-3. Back to cited text no. 18 |
| 19. | Farhatullah S, Kaza S, Athmanathan S, Garg P. Diagnosis of Herpes simplex virus-1 keratitis using Giemsa stain, Immunofluorescence assay, and Polymerase chain reaction assay on corneal scrapings. Br J Ophthalmol 2003. (In press) Back to cited text no. 19 |
| 20. | Schaumberg DA, Snow KK, Dana MR. The epidemic of Acanthamoeba keratitis: where do we stand? Cornea 1998; 17 :3-10. Back to cited text no. 20 |
| 21. | Niederkorn JY, Alizadeh H, Leher H, McCulley JP. The pathogenesis of Acanthamoeba keratitis; Review. Microbes Infect 1999; 1 :437-42. Back to cited text no. 21 |
| 22. | Auran JD, Starr MB, Jakobiec FA. Acanthamoeba keratitis: A review of literature. Cornea 1987; 6 :2-26. Back to cited text no. 22 |
| 23. | Lee GA, Gray TB, Dart JKG, Pavesio CE, Ficker LA, Larkin DFP, et al . Acanthamoeba sclerokeratitis: Treatment with systemic immunosuppression. Ophthalmology 2002; 109 :1178-82. Back to cited text no. 23 |
| 24. | Van Klink F, Taylor W M, Alizadeh H, Jager M J, van Rooigen N, Niederkorn J Y. The role of macrophages in Acanthamoeba keratitis. Invest Ophthalmol. Vis Sci 1996; 37 :1271-81. Back to cited text no. 24 |
| 25. | Mathers W, Steven G Jr, Rodrigues M, Chan CC, Gold J, Vissvesvara GS, et al . Immunopathology and electron microscopy of Acanthamoeba keratitis. Am J Ophthalmol 1987; 103 :626-35. Back to cited text no. 25 |
| 26. | Dougherty PJ, Binder PS, Mondino BJ, Glasgow BJ. Am J Opthalmol 1994;117:475-9. Back to cited text no. 26 |
| 27. | Weiner JM, Carroll N, Robertson IF. The granulomatous reaction in herpetic stromal keratitis: Immunohistochemical and ultrastructural findings. Aus NZ J Ophthalmol 1985; 13 :365-72. Back to cited text no. 27 |
| 28. | Green WR, Zimmerman LE. Granulomatous reaction to Descemet's membrane. Am J Ophthalmol 1967; 64 :555-8. Back to cited text no. 28 |
| 29. | Holbach LM, font RL, Naumann GOH. Herpes simplex stromal and endothelial keratitis: Granulomatous cell reaction at the level of Descemet's membrane, the stroma and Bowman's layer. Ophthalmol 1990; 97 :722-8. Back to cited text no. 29 |
| 30. | Vemuganti GK, Garg P, Gopinathan U, Naduvilath TJ, John RK, Buddi R, et al . Evaluation of agent and host factors in progression of mycotic keratitis: A histologic and microbiologic study of 167 corneal button. Ophthalmol 2002; 109 :1538-46. Back to cited text no. 30 |
| 31. | Williams GT, William WJ. Granulomatous inflammation - a review. J Clin Pathol 1983; 36 :723-33. Back to cited text no. 31 |
| 32. | Taussing MJ, editor. Processess in pathology and microbiology. 2nd edn. Oxford: Blackwell Scientific Publications; 1984. p. 164. Back to cited text no. 32 |
Copyright 2005 - Indian Journal of Medical Microbiology
The following images related to this document are available:
Photo images
[mb05071f6.jpg]
[mb05071f5.jpg]
[mb05071f8.jpg]
[mb05071t2.jpg]
[mb05071f10.jpg]
[mb05071f3.jpg]
[mb05071f1.jpg]
[mb05071t1.jpg]
[mb05071f2.jpg]
[mb05071f9.jpg]
[mb05071f4.jpg]
[mb05071f7.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}