 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
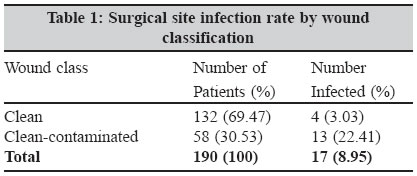
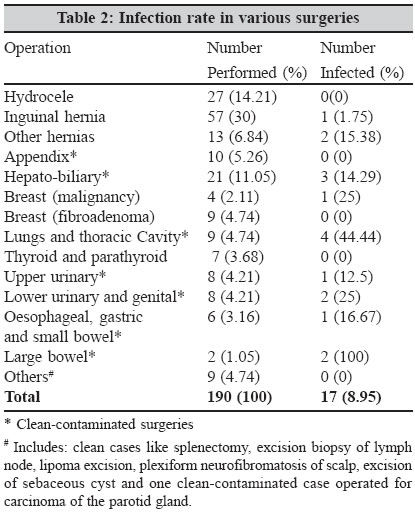
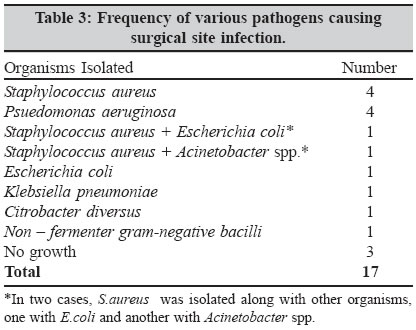
Indian Journal of Medical Microbiology, Vol. 23, No. 4, October-December, 2005, pp. 249-252 Brief Communications Surgical site infection in clean and clean-contaminated cases *Lilani SP, Jangale N, Chowdhary A, Daver GB *Corresponding author (email: Code Number: mb05074 Abstract The rate of surgical site infections and the frequency of various pathogens causing surgical site infection with their antibiotic resistance pattern in general surgery units were studied. In the period from May 2001 to July 2002, 190 patients admitted for surgery (clean and clean-contaminated elective cases) were assessed preoperatively, intraoperatively and postoperatively. Normal microbial flora was studied within 24 to 48 hours of admission and patients were followed up to 30 days postoperatively. Infected wounds were studied bacteriologically and clinically. The overall infection rate was 8.95%. Surgical site infection rate was 3.03% in clean surgeries and 22.41% in clean-contaminated surgeries. Significant increase was seen in surgical site infection rate with an increase in preoperative stay. The increase in duration of surgery was associated with a significant rise in the rate of surgical site infection. Surgical site infection rate was much higher (22.41%) in cases where a drain was used than in non-drained wounds (3.03%). The most common isolate was Staphylococcus aureus followed by Pseudomonas aeruginosa .Keywords: Surgical site infection, Clean and clean-contaminated surgeries, Staphylococcus aureus, Pseudomonas aeruginosa Surgical site infections are the third most commonly reported nosocomial infection and they account for approximately a quarter of all nosocomial infections.[1] They have been responsible for the increasing cost, morbidity and mortality related to surgical operations and continue to be a major problem even in hospitals with most modern facilities and standard protocols of preoperative preparation and antibiotic prophylaxis.[2] Surgical site infection rate has varied from a low of 2.5% to a high of 41.9%.[3],[4],[5],[6],[7],[8],[9],[10]Objective of this study was to know the rate of surgical site infection and to determine the frequencies of various pathogens causing surgical site infection with their antibiotic resistance pattern in general surgery. Materials and Methods The present study was conducted on patients admitted for surgery in general surgery units of Grant Medical College and Sir JJ Group of Hospitals, Mumbai. A total of 190 clean and clean-contaminated elective surgeries in two general surgery units from May 2001 to July 2002 were included in the study. The patients were assessed preoperatively, intraoperatively and postoperatively. Normal microbial flora of all patients was studied within a period of 24 to 48 hours of the admission to the general surgical ward. The sites included nose, throat, axilla, skin (the site of operation), perineum, and rectum as recommended earlier.[11],[12] Details that were recorded include the type of surgery by wound class (CDC, 1999), clean surgeries (Class I-operative wound) / clean-contaminated surgeries (Class II-operative wound), type and duration of operation, antimicrobial prophylaxis, drain used, preoperative hospital stay and total stay. Each patient was followed up from the time of admission till discharge from the hospital and also for 30 days postoperatively. Surgical wound was inspected at the time of first dressing and weekly thereafter for 30 days. Wound infection was diagnosed if any one of the following criteria were fulfilled: serous or non-purulent discharge from the wound, pus discharge from the wound, serous or non-purulent discharge from the wound with signs of inflammation (oedema, redness, warmth, raised local temperature, fever > 38°C, tenderness, induration) and wound deliberately opened up by the surgeon due to localized collection (serous/purulent). Stitch abscesses were excluded from this study. Swabs obtained from infected wounds were processed aerobically and anaerobically by standard methods.[13] Staphylococcus aureus strains isolated from infected surgical wounds were tested for β -lactamase production and also for methicillin resistance. Staphylococcus aureus strains were sent for phage typing to National Reference Centre for Staphylococcal Phage Typing, Department of Microbiology, Maulana Azad Medical College, New Delhi. Data were evaluated by chi square (X2 statistical test. P < 0.05 was considered to be significant. Results Out of total 190 patients, majority (57) were operated for inguinal hernia followed by operations for hydrocele (27), 132 (69.47%) were clean surgeries and 58 (30.53%) were clean-contaminated surgeries. Of the total 190 patients included in this study, 17 developed surgical site infection with the overall infection rate of 8.95%. Surgical site infection rate was 3.03% in clean surgeries and 22.41% in clean-contaminated surgeries [Table - 1]. The difference was found to be statistically significant (P = 0.0012). In clean surgeries, maximum infection rate was seen in mastectomies (25%) for breast malignancy, while patients with surgeries for hydrocele, fibroadenoma breast, thyroid and parathyroid had no surgical site infection [Table - 2]. In clean-contaminated surgeries, infection rate doubled in patients with surgeries for lower urinary tract and genital tract (25%) as compared to those with upper urinary tract surgeries (12.5%). In addition, surgical site infection rate was very high in cases of thoracotomies (44.44%). Two patients who underwent large bowel surgery, developed postoperative wound infection [Table - 2]. None of the patients who were operated within the first two days of admission to the ward had surgical site infection. The incidence of surgical site infection increased with increase in the duration of preoperative stay, and the difference was found to be statistically significant (P = 0.0034). There was no infection in surgeries lasting for less than 30 minutes. Infection rate was low (1.47%) for operations lasting for 30 minutes to less than an hour, while surgical site infection rate was high (38.46%) for operations that lasted for 120 minutes or more. The increase in the rate was statistically significant (P = 0.0021). Wound infection rate was much higher (22.41%) in cases where drain was used than in non-drained wounds (3.03%). The difference in infection rates was found to be statistically significant (P = 0.00016). Three of 17 infected wounds were culture negative. From the remaining 14 infected wounds, total 16 isolates were recovered [Table - 3]. Staphylococcus aureus was the commonest isolate followed by Pseudomonas aeruginosa . All the six S.aureus strains were resistant to penicillin. Five out of six stains were positive for β -lactamase and two were methicillin resistant (MRSA) S.aureus was isolated from six infected wounds [Table - 3]. In one patient, two S.aureus strains were isolated, one from the infected wound postoperatively and other from the axilla during preoperative normal flora surveillance. These two were having same antibiogram and belonged to the same phage type (type 80). In remaining five patients with S.aureus wound infection, S.aureus was not found at any of the normal flora sites during preoperative surveillance. Similarly, Escherichia coli isolated from one of the patients infected wound postoperatively, and also from his perineum and rectum preoperatively as a normal flora, revealed similar antibiograms. Pseudomonas aeruginosa exhibited 100% resistance to gentamicin. Other gram negative bacilli were found to be most resistant (100%) to tetracycline followed by ampicillin and cephalothin (83.33% each). The mean postoperative stay, in patients who did not develop any surgical site infection, was 6.19 days, whereas the mean postoperative stay increased four times (24.82 days) in 17 patients, who developed surgical site infection. Discussion The surgical site infection rate reports by different workers have differed considerably. The overall infection rate in the present study was 8.95% and compares favourably with other reported rates ranging from 2.5 to 41.9 %.[3],[4],[5],[6],[7],[8],[9],[10] Number of studies carried out in India indicate an overall infection rate of 4.04 to 30% for clean surgeries and 10.06 to 45% for clean-contaminated surgeries.[5],[7],[10] Findings in the present study show that there is significant rise in infection rate with increased degree of operative contamination; rate of infection for clean surgeries was 3.03% while in clean-contaminated surgeries it was 22.41%. A prolonged preoperative stay with exposure to hospital environment and its ubiquitous diagnostic procedures, therapies and microflora have been shown to increase the rate of surgical site infection.[14] Kowli et al found an infection rate of 17.4% when preoperative stay was 0-7 days and an infection rate of 71.4% with a preoperative stay of more than 21 days.[8] Anvikar et al (1999), in their study demonstrated an infection rate of 1.76% when preoperative stay was upto one day, which increased to 5.0% when the preoperative stay was more than one week.[10] In the present study, correlation was seen between duration of preoperative hospitalization and the development of surgical site infection. Significant increase in rate of surgical site infection was found in patients who had prolonged stay in hospital before the surgery. It has been observed that wound infection rate is influenced by duration of operation.[3], [5],[6],[7],[8],[10] The findings of the present study are in agreement with the reported literature. With increase in duration of surgery, the rate of infection increased in direct proportion. The results were found to be statistically significant. Higher surgical site infection rates have been noted for drained wounds as compared to non-drained wounds as was observed in this study.[3],[7] Many studies have reported Staphylococcus aureus as the commonest isolate from the postoperative wound infection.[1],[9],[15] In the present study, predominance of Staphylococcus aureus in surgical site infection is consistent with reports from other studies. Among gram negative bacilli, Pseudomonas aeruginosa was the commonest isolate in the present study. Based on the type of surgical procedure, the pathogens that are isolated from surgical site infection vary. It is found that in clean surgical procedures, Staphylococcus aureus from the exogenous environment or the patient′s skin flora is the usual pathogen, whereas, in other categories of surgical procedures, including clean-contaminated, contaminated and dirty, the polymicrobial flora closely resembling the normal endogenous microflora of the surgically resected organ are the most frequently isolated pathogens.[16] In the present study gram negative bacilli were predominantly isolated from clean-contaminated surgeries, while none of the infected wounds in clean class yielded gram negative bacilli. Number of studies in the literature indicate gradual increase in the emergence of antibiotic resistant microorganisms in surgical patients.[4],[5],[8],[10] Special interest in Staphylococcus aureus surgical site infection is mainly due to its predominant role in hospital cross infection and emergence of virulent antibiotic resistant strains. In the present study, all Staphylococcus aureus strains from the infected wound were resistant to penicillin. Ineffectiveness of penicillin in Staphylococcus aureus has been reported in other studies also.[4],[5],[10] Two out of six (33.33%) strains of Staphylococcus aureus were methicillin-resistant but none of the strains was resistant to vancomycin. All strains of Pseudomonas aeruginosa were resistant to gentamicin, which was one of the antibiotics used for antimicrobial prophylaxis. Prolonged postoperative hospitalization, which is a major concern of most of the hospitals, has been evident in patients developing surgical site infection.[6] In the present study, mean postoperative stay in patients who developed infection was almost four times (24.82 days) as compared to patients who did not develop surgical site infection where the mean postoperative stay was 6.19 days. Though the exact increase in patient-care cost due to prolonged postoperative hospital stay could not be calculated, it is a cause of concern for any hospital. Surveillance of surgical site infection with feedback of appropriate data to surgeons would be desirable to reduce the surgical site infection rate. References
Copyright 2005 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb05074t3.jpg] [mb05074t1.jpg] [mb05074t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}