 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
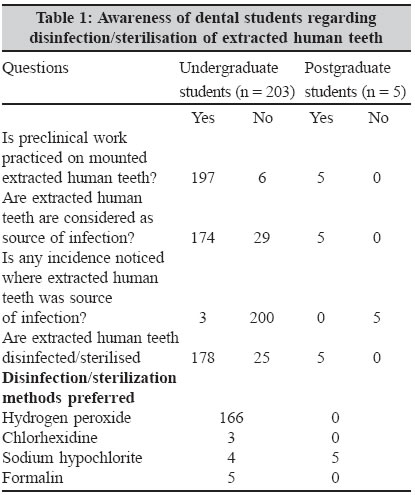
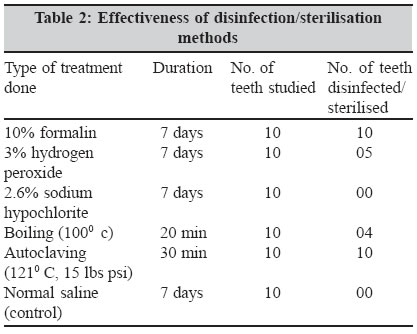
Indian Journal of Medical Microbiology, Vol. 23, No. 4, October-December, 2005, pp. 256-258 Brief Communications Sterilisation of extracted human teeth for educational use Kumar M, Sequeira PS, Peter S, *Bhat GK *Corresponding author (email: Code Number: mb05076 Abstract Sixty intact, non-carious and unrestored teeth extracted due to periodontal disease were used to determine the most effective method of sterilisation. The teeth were divided into six groups, each containing 10 teeth. Group 1 teeth were immersed in 10% formalin for seven days, group 2 teeth were immersed in 3% hydrogen peroxide for seven days, group 3 teeth were immersed in 2.6% sodium hypochlorite for seven days, group 4 teeth were boiled in water at 100°C for 20 minutes, group 5 teeth were autoclaved at 121°C at 15 lbs psi for 30 minutes, and group 6 teeth were immersed in normal saline for seven days. After the treatment, the teeth were individually inoculated into trypticase soy broth and incubated for 48 hours. A questionnaire survey was also conducted to determine the awareness of dental students regarding infection due to extracted human teeth and the common disinfection/sterilisation methods used. Autoclaving at 121°C, 15 lbs psi for 30 minutes and immersion in 10% formalin for seven days were effective in disinfecting/sterilising extracted human teeth. Chemicals such as 2.6% sodium hypochlorite, 3% hydrogen peroxide and boiling in water were not effective. The results indicate that autoclaving for 30 minutes or immersion in 10% formalin for seven days could be effectively used for disinfection/sterilisation of extracted human teeth. Keywords: Extracted human teeth, disinfection, sterilisation, chemicals, autoclaving, boiling Extracted human teeth are used routinely by dental students to learn technical and preclinical skills before they enter the clinical environment and deliver care to patients. Some endodontic procedures can be taught conceptually using manufactured instructional materials such as artificial plastic blocks and teeth on mannikins and models. However, there are instances where there is no substitute for extracted teeth for examination, preparation, or research.[1] Extracted human teeth are also used for in vitro laboratory dentin bonding research, before clinical trials ultimately decide their clinical effectiveness. In vitro tests such as bond strength measurements, microleakage evaluation and marginal gap measurements are indispensable as screening tests to predict the clinical behavior of new dentin bonding systems.[2] In recent years, infection control guidelines in dental institutions have been revised due to the possibility of cross-contamination from extracted teeth.[2] Directives by the American Dental Association (ADA) and the Centre for Disease Control (CDC) call for thorough removal of any organism capable of transmitting disease from nondisposable items used in patient care. By implication, these directives include those materials used in simulated care that may have come in contact with blood or saliva. Both of these body fluids are associated with extracted human teeth that are routinely used in dentistry to develop techniques and clinical skills.[3] Difficulties exist in the use of extracted human teeth because they are grossly contaminated, difficult to sterilize because of their structure, and may be damaged or altered by the sterilisation procedures.[3] It is apparent that many bloodborne pathogens, including hepatitis B virus, human immunodeficiency virus and bacterial pathogens, may be present in pulp, radicular and periradicular tissue of extracted human teeth.[4] Furthermore, since tooth preparation in technique laboratories is generally done without a liquid coolant, there is greater probability of exposure to pathogenic organism in the laboratory area. Certainly then, the risk exists for the spread of contagion, both, through aerosol and the accidental puncture wounds that might occur with dental instruments during handling.[3] The Centres for Disease Control (CDC), USA recommends storing extracted teeth in 1:10 household bleach.[3] However, one study [4] showed household bleach to be a poor disinfectant for this purpose. Ethylene oxide sterilisation has been found to have 20-36% efficacy on Bacillus subtilis spores in extracted teeth.[5] The efficacy of autoclaving in sterilising teeth depends on temperature and exposure time.[3] Gamma radiation could be used for sterilisation of teeth.[6] However, such a set-up is not present in many institutions. Several chemicals have been tried for disinfection/sterilisation of extracted human teeth with varying success.[1],[3],[4] At present, there is no specific recommendation for sterilisation of extracted human teeth used in dental technique course. The purpose of this study was to determine the efficacy of some commonly used chemicals and heat for disinfection/sterilisation of extracted human teeth. Method and Materials The present study was conducted in three phases. First phase consisted of a questionnaire-based survey to determine the awareness of dental students regarding infection due to extracted human teeth and the common disinfection/sterilisation methods used by them. In the second phase, the efficacy of some commonly used methods for disinfection/sterilisation of extracted human teeth were assessed. The third phase of the study was designed to determine whether the disinfection/sterilisation methods caused any alteration in the "feel" and cutting characteristics of the teeth. Questionnaire survey Evaluation of efficacy of chemical and physical disinfection/sterilisation methods The teeth were randomly divided into one of the following 6 groups (10 teeth per group). Teeth in group 1 were immersed in 10% formalin (Merck Limited, Mumbai, India), at 250 C for seven days, group 2 teeth were immersed in 3% hydrogen peroxide (Wilson Medicine Company, Mumbai, India), at 250 C for seven days, and group 3 teeth were immersed in 2.6% sodium hypochlorite (Novo Dental Products, Mumbai, India) at 250 C for seven days. All teeth were immersed in separate test tubes containing 20 mL of the disinfectant. Teeth in group 4 were boiled in water at 1000 C for 20 min and group 5 teeth were autoclaved at 1210 C at 15 lbs psi for 30 min. Group 6 consisted of a control, in which teeth were immersed in normal saline for seven days at 250 C. Following the assigned treatment procedures, teeth from each group were placed individually in separate test tubes containing 10 mL of tryptic soy broth (HiMedia, Mumbai, India) at 370 C for 48 hours. Evidence of growth was observed after two days. No visible growth in the broth after 48 hours was considered effective disinfection/sterilisation. Data were collected and statistical analysis was performed using Chi-square test. Assessment of cutting characteristics of disinfected/sterilised teeth Results [Table - 1] shows the awareness of dental students to questions regarding infection due to extracted human teeth and the common disinfection/sterilisation methods used by them. Hydrogen peroxide was the most common disinfectant used by the undergraduate students, while all postgraduate students preferred to use sodium hypochlorite. This difference was statistically significant (p < 0.05). Among the methods used, treatment with 10% formalin for seven days and autoclaving at 1210 C for 30 minutes were able to sterilise all the teeth [Table - 2]. Sodium hypochlorite (2.6%) was ineffective in disinfection of extracted human teeth, while 3% hydrogen peroxide and boiling in water for 20 min at 1000 C were effective in 5/10 and 4/10 of the samples respectively. All the 10 teeth immersed in normal saline showed bacterial growth. Chi-square analysis of the data showed a statistically significant difference in the outcomes when comparing the different methods of disinfection/ sterilisation methods. None of the disinfection/sterilisation methods altered the "feel" and cutting characteristics of the treated teeth. Discussion Since extracted human teeth may harbour potential pathogens, disinfection/sterilization of extracted human teeth in the teaching laboratory is important for educators and students. Further, bacteria can remain viable within the root canal of tooth for extended period of time.[3] The results of the present study showed that immersion in 10% formalin for seven days and autoclaving at 1210 C, 15 lbs psi for 30 minutes were effective in disinfecting/sterilising the extracted human teeth. Our results are consistent with observations made by previous workers.[1],[3],[4] Both these procedures did not seem to affect the "feel" and cutting characteristics of the teeth. Other chemical and physical methods used in the present study were significantly less effective than formalin and autoclaving. The difference in the effectiveness of the methods could be due to poor penetration of the agents into the pulp space or inactivation of the disinfectants by the organic substances present in the teeth. Although formalin is the most effective chemical, it is hazardous, irritant and a potential carcinogen.[7] With regards to autoclaving, there is concern about its use for sterilization of extracted teeth with amalgam restorations as it may release mercury vapors in the air through autoclave exhaust and residual mercury contamination of the autoclave.[1] Both formalin treatment and autoclaving treatment are simple, cheap and suitable for routine use in preclinical courses, exercises and research purposes. They do not alter the "feel" and cutting characteristics of the teeth. This observation is supported by earlier studies on functional characteristics of sterilised human teeth.[8],[9] Further, both autoclaving and formalin treatments can effectively destroy all kinds of microorganisms, including viruses. Based on our results, we recommend that all non-amalgam containing teeth to be autoclaved and amalgam containing teeth to be disinfected using formalin. References
Copyright 2005 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb05076t1.jpg] [mb05076t2.jpg] |
| |||||||||
{kind=link}
{kind=link}