 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
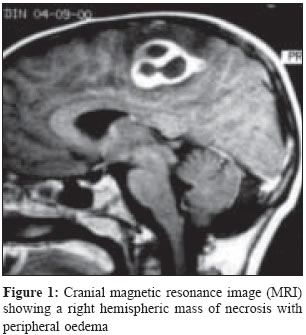
Indian Journal of Medical Microbiology, Vol. 23, No. 4, October-December, 2005, pp. 259-261 Case Reports Haemophilus aphrophilus brain abscess in the first decade *Bayraktar M, Onal C, Durmaz B, Yakinci C, Sonmezgoz E *Corresponding author (email: Code Number: mb05077 Abstract This report presents a case of brain abscess due to Haemophilus aphrophilus in a six-year old boy. He was admitted to our hospital suffering from left-sided weakness. The initial radiological diagnosis was an intracranial abscess. Purulent material was obtained by puncturing the subcortical lesion and the sample was cultured on conventional media. H. aphrophilus was isolated in pure culture, identified according to conventional methods and confirmed by Becton Dickinson Laboratory (BBL) crystal system. After surgical drainage and eight weeks of antibiotic therapy, the neurological findings improved. The presented case is an example of H. aphriphilus causing brain abscess in the first decade without cardiac predisposition and with good outcome. Keywords: Haemophilus aphrophilus, brain abscess, child Haemophilus aphrophilus is a fastidious gram negative bacillus belonging to the HACEK group.[1] It was so named because it needs high carbon dioxide atmosphere for its growth and the word ′′aphrophilus′′ means ′′foam loving.′′ It is usually present as a normal commensal in oral cavity and upper respiratory tract of human beings and animals like dogs.[1] It was first reported by Khairat et al in 1940 from a fatal case of endocarditis.[2] In addition to endocarditis, it has been implicated in other serious infections (brain abscess, spinal epidural abscesses, meningitis, osteomyelitis, arthritis, lymphadenitis and soft tissue infections) following trauma (teeth manipulation, lacerations, bites and postoperative wounds) particularly in absence of antibiotic prophylaxis. [1],[2],[3],[4],[5],[6],[7],[8],[9],[10] It causes human infections particularly in middle-aged and old people but not in pediatrics population. Involvement of brain by this specific organism in pediatric population without cardiac predisposition is very rare. Case Report A six-year old boy was referred to Turgut Ozal Medical Center with major complaint of left lower limb weakness. On neurological examination, hemiparesis, brisk deep tendon reflexes and positive plantar reflexes were observed on the left side. Otorhinolaryngological examination was within normal limits. Physical examination revealed an axillar temperature of 38 0 C, pulse of 138 /minutes and a respiratory rate of 36 minutes. His white blood cell count was 10,700/mm 3 with 59% polymorphonuclear cells. Echocardiogram was normal. Cranial magnetic resonance imaging (MRI) disclosed a right subcortical multilocular mass of 30 x 30 x 20 mm. in dimensions with peripheral oedema and rim enhancement [Figure - 1]. Cranial computerized tomography (CT) showed a round spherical mass and oedema in right hemisphere [Figure - 2]. By CT-guidance, the subcortical mass was punctured under local anesthesia with the initial diagnosis of intracranial abscess. Adequate antibiotic therapy was initiated. H. aphrophilus was isolated on the culture. Culture results demonstrated the effectiveness of ampicillin. Two recurrent punctures with two weeks intervals were performed by aspirating 30 mL and 20 mL pus respectively. Control CT scans showed diminished lesion with no peripheral oedema. After six weeks of parenteral antibiotic therapy, hemiparesis and other neurological manifestations disappeared over six weeks period. Gram staining of purulent material revealed many polymorphonuclear leukocytes and gram negative bacilli. Primary culture was made on trypticase soy agar supplemented with 5% sheep blood, chocolate agar and eosin methylene blue agar (EMB). After 48 hours incubation at 35o C in 5% CO 2 atmosphere, pure growth of small non hemolytic colonies was seen on trypticase soy agar and chocolate agar. EMB yielded very tiny colorless colonies. The organism did not grow anaerobically. Gram stain of colonies showed gram negative coccobacilli. No difference in culture yield was observed when the organism was incubated in atmosphere with and without CO 2 . It did not require X and V factors. In trypticase soy broth culture, it produced microcolonies some of which adhered to sidewalls of tubes. Yellowish pigment was seen on rubbing of cotton swabs on the surface of colonies. The organism was late oxidase positive. Catalase, urease and indole tests were negative. Acid but no gas was produced from glucose and lactose on triple sugar iron agar. The organism was identified and confirmed as H. aphrophilus by performing BBL Crystal Haemophilus 10-System BBL.[1] The organism was not isolated after treatment. Discussion The first case of brain abscess due to H. aphrophilus was reported by Fager in 1964.[3] Since then, many cases of brain abscesses have been documented and a number of patients have been reported to have a history of respiratory infection, human or animal bites and dental disease. [4],[5],[6]However, H. aphrophilus infection should be suspected in individuals with history of recent dental manipulation, bite or in those with close contact with pets such as dogs but without antibiotic cover. [2],[3],[4],[5],[6],[7]The patient had no signs and symptoms of respiratory infections such as sinusitis, otitis media, and chronic bronchitis or other infections. Therefore, the source of infection in current case was probably teeth decay with history of recent teeth manipulation within the last month. H. aphrophilus infection has been most commonly observed in young adults and elderly[9] and very rarely in paediatric population. There is no case described in the available literature where this microorganism has caused brain abscess in children without cardiac predisposition. In an extensive review by Bieger et al , which consisted of 42 cases, only two cases were in the first decade and only one of them had a brain abscess.[10] Previous studies showed that central nervous system abscesses were sterile in 9-63% pus samples,[4] however, improvement in culture methods, prompt inoculation and prompt incubation for 48 hours or over were required for successful isolation of H. aphrophilus.[2] Prompt antibiotic therapy and adequate drainage of brain abscess via minimally invasive surgery are essential since these infections are serious and have high mortality rates.[2] It has been mentioned that therapy with ciprofloxacin or ceftriaxon had led to full recovery and an initial antimicrobial therapy with these drugs is recommended.[11] Nevertheless, good response was obtained in our case following therapy with ampicillin. Pus was removed by draining the brain abscess and the patient improved after surgical procedure. Hence, to achieve optimal therapy, surgical intervention is necessary in addition to antimicrobial treatment. Prophylactic measure is indispensable after dental manipulation. Finally, this report presents a patient within the first decade of life having an intracranial abscess due to H. aphrophilus with no cardiac pathology. The combination of neurosurgical intervention and postoperative antibiotic therapy provided a good prognosis. All brain abscess specimens should be processed rapidly and cultured for a prolonged period to ensure recovery of fastidious organisms which may determine antibiotic therapy. References
Copyright 2005 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb05077f1.jpg] [mb05077f2.jpg] |
| |||||||||
{kind=link}
{kind=link}