 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 24, No. 1, January-March, 2006, pp. 25-29 Original Article Detection of biofilm formation among the clinical isolates of Staphylococci: An evaluation of three different screening methods Mathur *T, Singhal S, Khan S, Upadhyay DJ, Fatma T, Rattan A New Drug Discovery Research, Ranbaxy Research Laboratories, (TM, SS, SK, DJU, AR) Gurgaon-122 001, Haryana, India and Department of Biosciences (TF), Jamia Millia Islamia University, Jamia Nagar, New Delhi-110 025, India Correspondence Address: Mathur *T, E-mail:
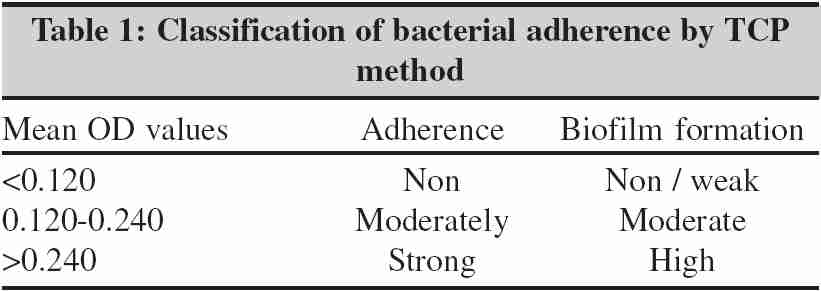
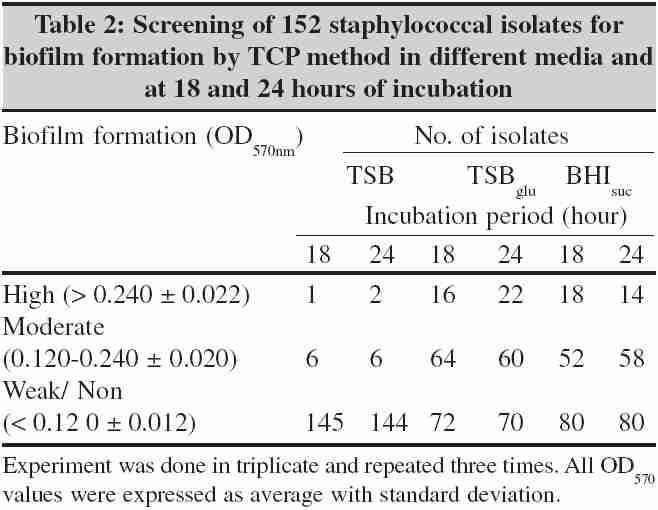
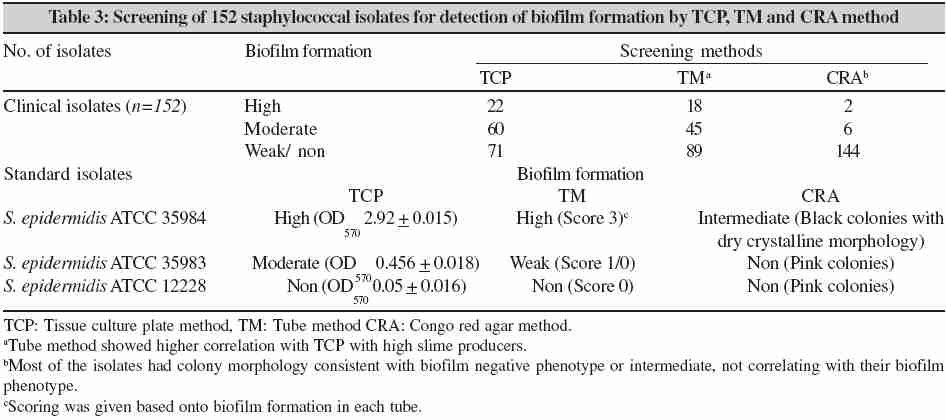
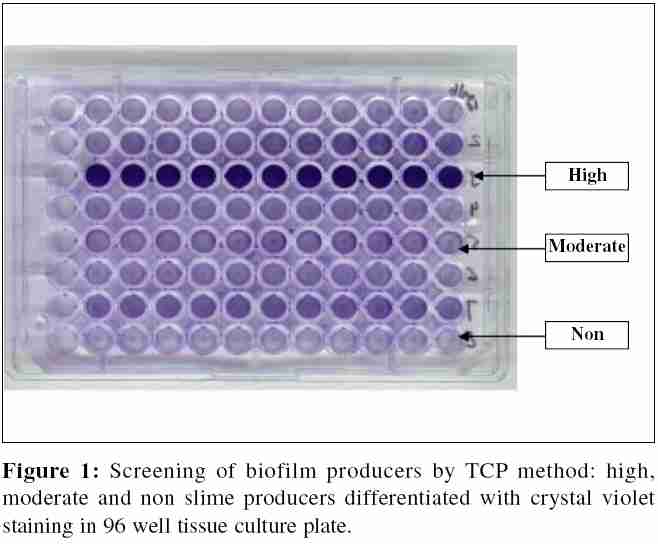
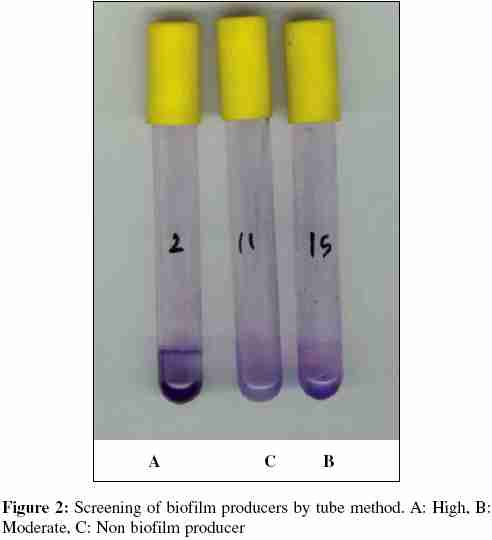
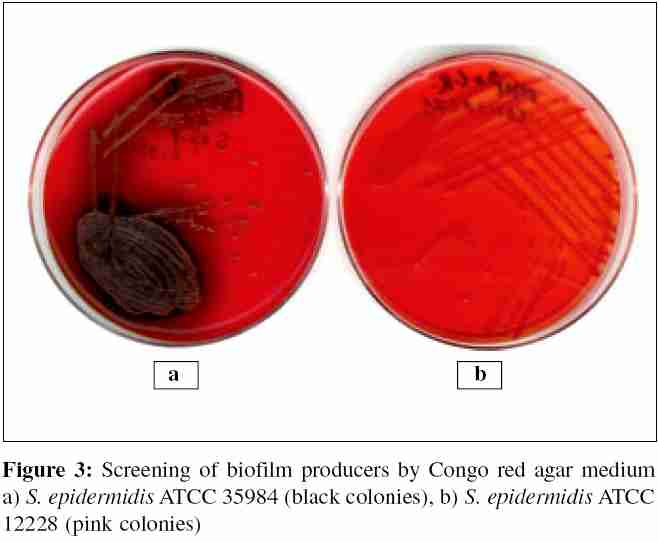
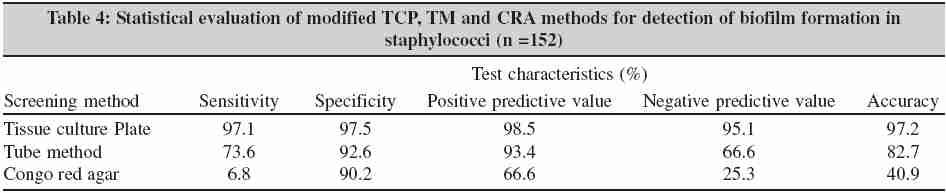
mathurtarun@ranbaxy.com Code Number: mb06004 Abstract Purpose: The purpose of this study was to evaluate three methods for detection of biofilm formation in staphylococci.Methods: For detection of biofilm formation, 152 clinical isolates of Staphylococcus spp. were screened by tissue culture plate (TCP), Tube method (TM) and Congo red agar (CRA) method. Results: Of the 152 Staphylococcus spp. 88(57.8%) displayed a biofilm-positive phenotype under the optimized conditions in the TCP method and strains were further classified as high 22 (14.47 %) and moderate 60 (39.4 %) while in 70 (46.0 %) isolates weak or no biofilm was detected. Though TM correlated well with the TCP test for 18 (11.8 %) strongly biofilm producing strains, weak producers were difficult to discriminate from biofilm negative isolates. Screening on CRA does not correlate well with either of the two methods for detecting biofilm formation in staphylococci. Conclusion: The TCP method was found to be most sensitive, accurate and reproducible screening method for detection of biofilm formation by staphylococci and has the advantage of being a quantitative model to study the adherence of staphylococci on biomedical devices. Keywords: Staphylococci, adherence, biofilm, tissue culture plate, Congo red agar Staphylococci are most often associated with chronic infections of implanted medical devices.[1],[2],[3] The use of indwelling medical devices is important in the treatment of critically and chronically ill patients, however bacterial colonization of implanted foreign material can cause major medical and economic sequel. The increased use of indwelling medical devices has had considerable impact on the role of staphylococci in clinical medicine. The predominant species isolated in these infections are Staphylococcus epidermidis and Staphylococcus aureus, their major pathogenic factor being ability to form biofilm on polymeric surfaces.[4] Biofilm consists of multilayered cell clusters embedded in a matrix of extracellular polysaccharide (slime), which facilitates the adherence of these microorganisms to biomedical surfaces and protect them from host immune system and antimicrobial therapy.[5] Biofilm formation is regulated by expression of polysaccharide intracellular adhesin (PIA), which mediates cell to cell adhesion and is the gene product of icaADBC .[6] Various reports attest to the presence of icaADBC gene in S. aureus and S. epidermidis isolated from infections associated with indwelling medical devices.[7],[8] It is now well documented that biofilms are notoriously difficult to eradicate and are often resistant to systemic antibiotic therapy and removal of infected device becomes necessary. [9],[10],[11] The differentiation of staphylococci with respect to its biofilm phenotype might help to elucidate the impact of staphylococci in diagnosis of infections related to biomedical devices and these observations may have utility in the prevention of device related infections.[12] A number of tests are available to detect slime production by staphylococci; methods include tissue culture plate (TCP), [13] tube method (TM),[14] Congo red agar (CRA),[15],[17] bioluminescent assay[18] and light or fluorescence microscopic examination.[19],20 These methods are often subject to severe analytical limitations and are unable to detect bacterial adherence accurately. In this study, we simultaneously screened 152 clinical isolates of Staphylococcus spp. by TCP (standard and modified), TM and CRA methods for determining their ability to form biofilm and also evaluated the reliability of these methods in order to determine most suitable screening method. Materials and Methods Bacterial strains A total of 152 non-repetitive, clinical isolates of Staphylococcus spp. isolated from blood, infected devices and skin surfaces received from different tertiary care centers in India were investigated. Isolates were initially identified by standard microbiological techniques including Gram stain, catalase test and coagulase test. All cultures were maintained on trypticase soy agar, Difco (TSA). Known additional reference strains of S. epidermidis ATCC 35984 (high slime producer) S. epidermidis ATCC 35983 (moderate slime producer) and S. epidermidis ATCC 12228 (non slime producer), obtained from American type culture collection (ATCC, Rockville, Md.), were also included in the study. Detection of biofilm formation Tissue culture plate method (TCP) The TCP assay described by Christensen et al [13] is most widely used and was considered as standard test for detection of biofilm formation. In present study, we screened all isolates for their ability to form biofilm by TCP method as described by Christensen et al [13] with a modification in duration of incubation which was extended to 24 hours. Previous reports have indicated the influence of media composition on biofilm production, therefore we had evaluated biofilm production in three different media, tryticase soy broth (TSB Difco), TSB with 1% glucose (TSBglu) and brain heart infusion (BHI, Difco) with 2% sucrose (BHISuc). Isolates from fresh agar plates were inoculated in respective media and incubated for 18 hour at 37oC in stationary condition and diluted 1in100 with fresh medium. Individual wells of sterile, polystyrene, 96 well-flat bottom tissue culture plates (Tarson, Kolkata, India) wells were filled with 0.2 ml aliquots of the diluted cultures and only broth served as control to check sterility and non-specific binding of media. The tissue culture plates were incubated for 18 hours and 24 hours at 37°C. After incubation content of each well was gently removed by tapping the plates. The wells were washed four times with 0.2 mL of phosphate buffer saline (PBS pH 7.2) to remove free-floating 'planktonic' bacteria. Biofilms formed by adherent 'sessile' organisms in plate were fixed with sodium acetate (2%) and stained with crystal violet (0.1% w/v). Excess stain was rinsed off by thorough washing with deionized water and plates were kept for drying. Adherent staphylococcal cells usually formed biofilm on all side wells and were uniformly stained with crystal violet. Optical density (OD) of stained adherent bacteria were determined with a micro ELISA auto reader (model 680, Bio rad ) at wavelength of 570 nm (OD 570 nm ). These OD values were considered as an index of bacteria adhering to surface and forming biofilms. Experiment was performed in triplicate and repeated three times, the data was then averaged and standard deviation was calculated. To compensate for background absorbence, OD readings from sterile medium, fixative and dye were averaged and subtracted from all test values. The mean OD value obtained from media control well was deducted from all the test OD values. Classification of bacterial adherence For the purpose of data calculation, we used classification [Table - 1] based on OD values obtained for individual strains of Staphylococcus spp. [13] Tube method (TM) A qualitative assessment of bifilm formation was determined as previously described by Christensen et al. [14] TSBglu (10mL) was inoculated with loopful of microorganism from overnight culture plates and incubated for 24 hours at 37°C. The tubes were decanted and washed with PBS (pH 7.3) and dried.dried tubes were stained with crystal violet (0.1%). Excess stain was removed and tubes were washed with deionized water. Tubes were than dried in inverted position and observed for biofilm formation. Biofilm formation was considered positive when a visible film lined the wall and bottom of the tube. Ring formation at the liquid interface was not indicative of biofilm formation. Tubes were examined and the amount of biofilm formation was scored as 0-absent, 1-weak, 2-moderate or 3-strong Experiments were performed in triplicate and repeated three times. Congo red Agar method (CRA) Freeman et al [15] had described an alternative method of screening biofilm formation by Staphylococcus isolates; which requires the use of a specially prepared solid medium -brain heart infusion broth (BHI) supplemented with 5% sucrose and Congo red. The medium was composed of BHI (37 gms/L), sucrose (50 gms/L), agar no.1 (10 gms/L) and congo red stain (0.8 gms/L). Congo red was prepared as concentrated aqueous solution and autoclaved at 121°C for 15 minutes, separately from other medium constituents and was then added when the agar had cooled to 55°C. Plates were inoculated and incubated aerobically for 24 to 48 hours at 37°C. Positive result was indicated by black colonies with a dry crystalline consistency. Weak slime producers usually remained pink, though occasional darkening at the centers of colonies was observed. A darkening of the colonies with the absence of a dry crystalline colonial morphology indicated an indeterminate result. The experiment was performed in triplicate and repeated three times. Statistical evaluation of TCP, TM and CRA method for detection of biofilm formation The comparitive statistical analysis for all methods by using 2x2 table given by Greenhalgh.[16] Data obtained from standard TCP method was considered as gold standard for this study was compared with data from modified TCP, TM and CRA methods. Parameters like sensitivity: a / (a + c), specificity: d / (b + d), negative predictive value (PV -): d / (c + d), positive predictive value (PV +): a / (a + b) and accuracy; (a + d) / (a + b + c + d): were determined, wherein a, b, c and d refer to number of determinants in which true positives (a) were biofilm producers by modified TCP, TM and CRA as well as positive by standard TCP method(gold standard), false positives (b) were biofilm producers by TCP, TM and CRA method but negative by TCP method, false negatives (c) were non biofilm producers by TCP, TM and CRA but biofilm producers by standard TCP, true negatives (d) were non biofilm producers by all the methods. Results In the standard TCP assay, only 7(4.6%) of 152 tested isolates displayed biofilm positive phenotype in TSB medium, whereas with addition of 1% glucose in TSB(TSBglu), number of biofilm forming isolates increased to 80 (52.6%) and 82 (53.9%) after incubation for 18 hour and 24 hours respectively. Similarly, by using BHIsuc medium 70 (46.0 %) biofilm forming isolates were detected [Table - 2]. In modified TCP method, from the total number of 152 isolates tested for biofilm formation, strong biofilm producers were 22 (14.4 %), 60 (39.4%) were moderate and 70 (46.0%) isolates were considered as non or weak biofilm producers [Table - 3], [Figure - 1]. The TM showed good correlation with the TCP assay for strongly biofilm forming isolates and total 18 (11.8%) isolates were picked up as strong and 45 (29.6%) were moderat biofilm producers. However, it was difficult to discriminate between moderate and weakly biofilm producing isolates [Figure - 2]. By CRA method we obtained very different results, most of the strains displayed red (pink to orange) colonies on medium typical for biofilm Staphylococcus isolates, 3 (1.97%) isolates showed black colonies, but no dry crystalline morphology was observed. Only 5 (3.2%) isolates displayed red colonies with dry crystalline morphology after 24-48 hours [Figure - 3]. With the exception of these 8 (5.2%) isolates showing black or red colonies with and without dry crystalline morphology, no correlation between colony morphology on CRA and TCP results was observed [Table - 3]. Using well-characterized 152 isolates data obtained from standard TCP method was used to evaluate TCP, TM, and CRA methods. The modified TCP method was most sensitive (96.2%) and specific (94.5%) with high accuracy (97.3%) in terms of discriminating between biofilm producers and non-producers. In TM, strong biofilm producers could be easily detected, where as it was difficult to differentiate between moderate and weak biofilm forming isolates, which affected its performance in terms of sensitivity (77.9 %), specificity (96.0%) and accuracy (86.8 %). CRA method showed very little correlation with corresponding methods and the parameters of sensitivity (7.6 %), specificity (97.2 %) and accuracy (51.3 %) were very low [Table - 4]. Discussion Slime production has been reported in strains of all Staphylococcus spp. associated with the infection of biomedical devices. [4],[5],[13] Investigations to understand the pathogenesis of these infections have focused upon the process of adherence of these microorganisms on these devices. Investigators have used various methods to quantify number of microorganisms adhering to surfaces. [13],[15],[16],[17],[18],[19],20 We tested 152 clinical isolates of staphylococci by three in vitro screening procedures for their ability to form biofilm. In the TCP assay with TSB medium, only 7 (4.6 %) of 152 tested S taphylococcus isolates displayed a biofilm positive phenotype. This was in agreement with observations of other investigators in which only few or no biofilm producing isolates could be detected using this medium. [17] On the other hand supplementation of TSB and BHI media with different sugars such as glucose and sucrose exhibited biofilm formation in 80 (52.6%) and 70 (46.0%) isolates respectively. In modified TCP method, extended incubation for 24 hour could lead to a better discrimination between moderate and non-biofilm producing staphylococci and biofilm formation was observed in 82 (53.9%) isolates. These observations suggested a strong dependence between growth condition and biofilm formation in staphylococci and that the use of various sugar supplementations is essential for biofilm formation. [17] The tube test correlates well with the TCP test for strongly biofilm producing isolates but it was difficult to discriminated between weak and biofilm negative isolates due to the variability in observed results by different observers. Consequently, high variability was observed and classification in biofilm positive and negative was difficult by tube method. In agreement with the previous reports, tube test cannot be recommended as general screening test to identify biofilm-producing isolate. [14] In CRA method, out of eight positive isolates, three (1.97%) displayed black colonies with no dry crystalline morphology, and five (3.2%) displayed dry crystalline morphology. In rest of the strains no correlation was observed with TCP and TM. These observations are entirely in disagreement with observations reported by the Freeman DJ et al. [15] Based on our results we are unable to recommend the CRA method for detection of biofilm formation by Staphylococcus isolates. Our data indicates that the TCP method is an accurate and reproducible method for screening and this technique can serve as a reliable quantitative tool for determining biofilm formation by clinical isolates of staphylococci. Acknowledgement We appreciate the help of Dr. MK Lalitha, CMC, Vellore; Dr. Archana Ayyagari, SGPGI, Lucknow and Dr. Sarman Singh, AIIMS, New Delhi, for providing the clinical isolates for this study.References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06004t1.jpg] [mb06004t2.jpg] [mb06004t3.jpg] [mb06004f2.jpg] [mb06004f3.jpg] [mb06004f1.jpg] [mb06004t4.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}