 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 24, No. 1, January-March, 2006, pp. 34-38 Original Article Prevalence and antimicrobial susceptibility pattern of methicillin resistant Staphylococcus aureus: A multicentre study. Rajaduraipandi *K, Mani KR, Panneerselvam K, Mani M, Bhaskar M, Manikandan P Department of Microbiology, Dr. GR Damodaran College of science, Coimbatore- 641 014, Tamilnadu, Pasteur Institute of India (KRM), Coonoor, Tamilnadu, Microbiological Laboratory (MM), Coimbatore, Tamilnadu, Department of Microbiology (MB),Coimbatore Medical College, Coimbatore, Tamilnadu, and Department of Microbiology (PM), Aravind Eye Care System, Aravind Eye Hospital and Post Graduate Institute of Ophthalmology, Coimbatore-641 014, Tamilnadu, India Correspondence Address: Rajaduraipandi *K, E-mail: rajaduaripandi2003@yahoo.com Code Number: mb06006 Abstract Purpose: Methicillin resistant Staphylococcus aureus (MRSA) is an important nosocomial pathogen. We report the prevalence and antibiotic susceptibility pattern of MRSA in major southern districts of Tamilnadu. Keywords: MRSA, prevalence, multidrug resistance, Staphylococcus aureus, antibiotic
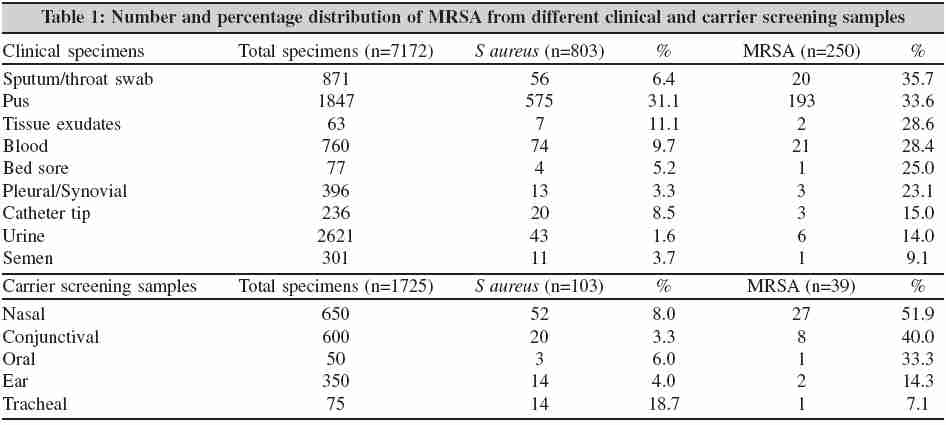
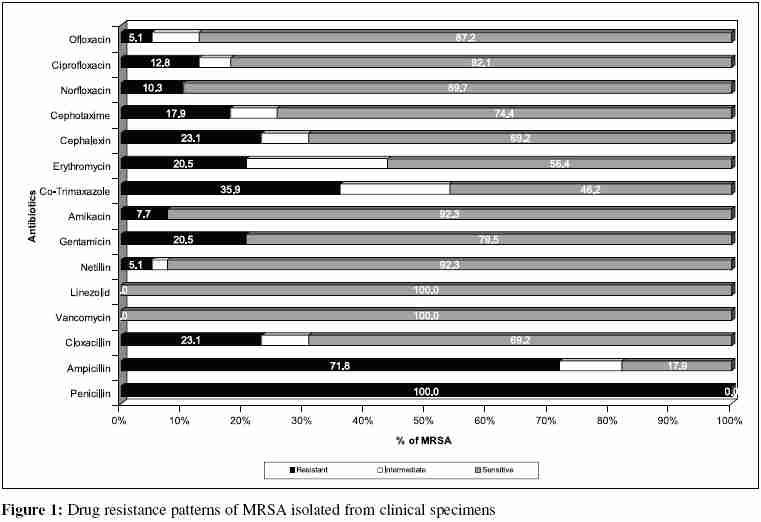
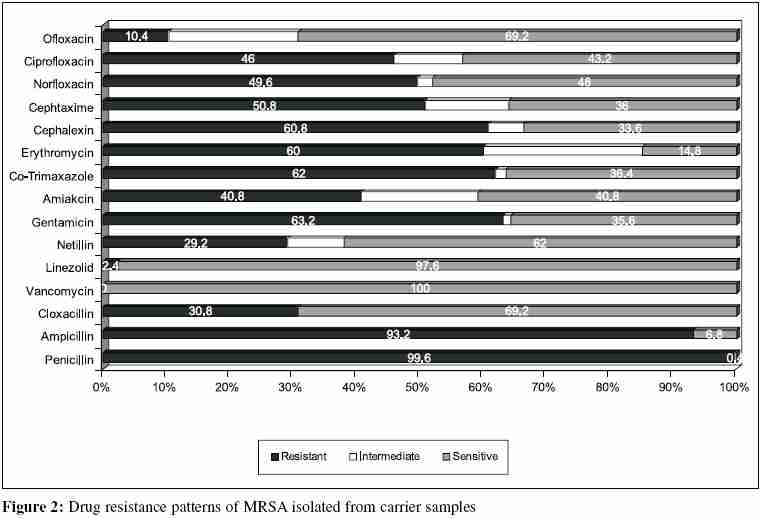
The genus Staphylococcus includes pathogenic organisms in which Staphylococcus aureus is most important. It has overcome most of the therapeutic agents that have been developed in the recent years and hence the antimicrobial chemotherapy for this species has always been empirical.[1] The most notable example of this phenomenon was the emergence of methicillin resistant S taphylococcus aureus (MRSA), which was reported just one year after the launch of methicillin.[2] Many of these MRSA isolates are becoming multidrug resistant and are susceptible only to glycopeptide antibiotics such as vancomycin.[3] Low level resistance even to vancomycin is emerging at present.[4] The prolonged hospital stay, indiscriminate use of antibiotics, lack of awareness, receipt of antibiotics before coming to the hospital etc. are the possible predisposing factors of MRSA emergence.[5] Serious endemic and epidemic MRSA infections occur globally as infected and colonized patients in hospitals mediate the dissemination of these isolates and hospital staff assists further transmission. [6] The development of resistance to multiple antibiotics and control of disease transmission by MRSA isolates in hospitals/communities have been recognized as the major challenges as the bacterial population that expresses the resistance phenotype varies according to the environmental conditions.[2] Therefore, the knowledge of prevalence of MRSA and their current antimicrobial profile become necessary in the selection of appropriate empirical treatment of these infections. We determined the prevalence of MRSA from different clinical and carrier screening samples and their in vitro susceptibility pattern to various antimicrobial agents to record the current status of MRSA response to commonly used anti Staphylococcus antibiotics in major southern districts of Tamilnadu. Materials and Methods A total of 8897 clinical specimens and carrier screening samples such as urine, pus, sputum/throat swab, blood, pleural and synovial fluid, semen, catheter tip, bedsore, tissue exudates, conjunctival, ear, nasal, tracheal swabs and oral scraping were collected for Staphylococcus aureus screening The clinical samples (7172) were obtained from various private hospitals and Microbiological Laboratory Pvt. Ltd (Micro-lab), Coimbatore and from the subcenters of the microbiology laboratories scattered in Salem, Coonoor, Erode, Karur, Trichirappalli, and Palayamkottai of Tamilnadu from July 2000 to June 2002. The remaining 1725 carrier screening samples were obtained from either sex who accompanied patients to the clinical centers/hospitals and volunteers working in these centers and were subjected to S. aureus isolation so as to compare these isolates with the isolates of clinical specimens. All the samples were aseptically handled and processed. The morphotypes were done for all the samples based on the Gram staining method to determine the likely organism present. Subsequently, the clinical specimens and carrier screening samples were inoculated on to blood agar plates (aerobic with 5% CO 2 ), MacConkey agar and RCM (Robertson cooked meat medium) for further subculturing and incubated at 37°C for 24 hours. The colonies of Gram-positive cocci in clusters were further confirmed using API-Staph biochemical strip (bioMerieux, France). All strains were further tested for the production of free coagulase enzyme using tube coagulase test based on standard methods.[7] Staphylococcus aureus ATTC-25923 of known coagulase production was included as control strain. All the confirmed S. aureus strains were subsequently tested for methicillin resistance based on Kirby-Bauer disk diffusion method using oxacillin discs (1ìg) obtained from Hi-Media Laboratories Pvt. Ltd. The isolates were considered methicillin resistant if the zone of inhibition was 10 mm or less. Further, the antibiotic susceptibility pattern of methicillin resistant S. aureus strains was determined on the day of their isolation by the modified Kirby Bauer disc diffusion method on Muller Hinton agar using the criteria of standard zone sizes of inhibition to define sensitivity or resistance to different antimicrobials. The antibiotics used were penicillin-G (10 unit); ampicillin (10 µg); cloxacillin (30µg); cephalexin (30µg); cephotaxime (30µg); erythromycin (15µg); gentamycin (10µg); amikacin (30µg); netillin (30µg); ciprofloxacin (5µg); ofloxacin (5µg); norfloxacin (10µg); co-trimoxazole (25µg); vancomycin (30µg); linezolid (30µg). Finally, the data were recorded and analyzed at the completion of the study as per recommendations of the NCCLS.[8] S. aureus ATCC 29213 was used as reference strain for the standardization of antibiotic susceptibility testing. Results A total number of 906 Staphylococcus aureus was isolated, of which 803 and 103 were from clinical specimens and carrier screening samples respectively [Table - 1]. The reports on the methicillin resistance by these isolates confirmed the presence of 289 MRSA (250 from clinical specimens and 39 from carrier screening samples) and the remaining strains were considered as methicillin sensitive S. aureus (MSSA). The prevalence of MRSA was significantly different among various clinical specimens ( p < 0.001) and was found that 35.7% of these isolates were from throat swabs, followed by pus (33.6%) and 9.1% from semen. Similarly, the number of MRSA isolates was significantly different between various carrier screening samples (chi square-13.36; p -0.001), in which from nasal swab alone 51.9% of MRSA were obtained, followed by conjunctival (40.0%) and the lowest 7.1% from tracheal. The prevalence rate of S. aureus and MRSA in these two categories of samples is shown in [Table - 2]. The drug resistance patterns of MRSA isolated from clinical specimens and carrier screening samples were found to be highly variable. Almost all the 250 MRSA strains (99.6%) screened from clinical specimens were resistant to penicillin, 93.2% to ampicillin, 63.2% to co-trimoxazole, 62% to gentamicin, 60.8% to cephalexin and 60.0% to erythromycin. However, all (100%) MRSA strains recorded sensitivity to vancomycin, which was followed by 97.6% to linezolid. In general, all MRSA strains were resistant to 8.0 ± 0.3 drugs, in which 63.6% isolates proved multidrug resistance. Higher percentage of intermediate resistance was noted against antibiotics such as erythromycin, Ofloxacin, amikacin, cephotaxime and ciprofloxacin. In contrast to these observations all the 39 MRSA strains (100%) of carrier samples had resistance to penicillin antibiotic. Against ampicillin and co-trimoxazole 71.8% and 35.9% MRSA strains showed resistance respectively. However, 100% sensitivity was observed to both vancomycin and linezolid followed by 92.3% to netillin and cloxacillin, 89.7% to amikacin and 87.2% to ofloxacin. To 4.5±0.4 drugs all carrier screening samples derived MRSA strains had resistance and only 23% isolates exhibited multipledrug resistance. The different drug resistance patterns of MRSA obtained from clinical specimens and carrier screening samples are shown in [Figure - 1][Figure - 2] respectively. Discussion MRSA is a major nosocomial pathogen causing significant morbidity and mortality.[9] The important reservoirs of MRSA in hospitals/institutions are infected or colonized patients and transient hand carriage on the hands of health care workers is the predominant mode for patient-to-patient transmission.[6] In India, the significance of MRSA had been recognized relatively late and it emerged as a problem in the 80s and in the 90s. Epidemic strains of these MRSA are usually also resistant to several other antibiotics. During the past 15 years, the appearance and world-wide spread of many such clones have caused major therapeutic problems in many hospitals, as well as diversion of considerable resources to attempts at controlling their spread.[10] In this study, the prevalence and antibiotic susceptibility patterns of various MRSA isolates obtained from different clinical and carrier subjects were determined. We isolated 250 and 39 MRSA strains from 803 clinical specimens and 103 carrier screening samples respectively. As high as 35.7% of MRSA strains were obtained from throat swabs and 33.6% of strains were obtained from pus among clinical isolates. Similar observation was made by Mehta, who in his study on control of MRSA in a tertiary care center, had reported an isolation rate of 33% from pus and wound swabs.[3] However, Qureshi from Pakistan reported a high isolation rate of up to 83% MRSA from pus.[2] Another significant observation in this study was the increased isolation of MRSA from carrier screening samples. No precise reason could be attributed to this apparent increase in carrier rate. This is an alarming observation despite the fact that carrier screening samples are less compared to clinical samples. Contemporary literature shows highly variable carrier rate ranging from 0% to 29%.[3],[9],[11] But nasal carriage (57.9%) was the commonest presentation followed by conjuntival carriage (40%) among carriers. In this study all the strains showed susceptibility to vancomycin and most of them were susceptible to linezolid. As expected, all the strains were resistant to penicillin and most of them were resistant to ampicillin. But the significant and clinical relevant observation of this study is the moderate resistance shown by MRSA to other conventional antibiotics. The other contemporary reports state higher resistance rates for aminoglycosides and fluoroquinolones. In one study on spectrum of antimicrobial resistance among MRSA, ciprofloxacin resistance was as high as 90% and Qureshi had reported the same as 98.9%. [2],[11] In contrast we have 46% of the strains resistant to ciprofloxacin and a further lower resistant rate to ofloxacin (10.4%). However, Pulimood had observed only 8% resistance of MRSA to gentamicin[2] as against 63.6% in our study. Gentamicin resistance is on the rise since 1996. An increase of gentamicin resistance from 0% before 1996 to 80% after 1996 has been reported.[12] Qureshi had reported a gentamicin resistance of 97.8%,[2] which is higher compared to our study. Although MRSA from clinical specimens showed higher susceptibility to individual antibiotics when compared with others, we obtained high percentage of multidrug resistant MRSA from these specimens. Majumder from Assam had reported 23.2% of the MRSA isolated from clinical specimens to be multidrug resistant.[13] Anupurba from Uttarpradesh had reported a higher percentage of multidrug resistant MRSA. [4] Vidhani from Delhi reported even a higher percentage of multidrug MRSA but from high risk patients admitted in burns and orthopedic units.[14] All the carrier strains were resistant to penicillin and most of them were resistant to ampicillin. This is in contrast to other studies where higher susceptibility rate was observed among the strains obtained from carrier screening samples. [15] Nevertheless, we have observed low percentage (23%) of multidrug resistant MRSA from carrier samples. In conclusion, the degree of resistance or sensitivity of MRSA towards commonly used antibiotics is recognized to be diverse from region to region and vancomycin was the only antibiotic found to give uniform sensitivity (100%). When antimicrobials including vancomycin are considered for treatment, choice inevitably requires the need for in vitro susceptibility testing of every isolate of MRSA in the clinical laboratories. Our study is a preamble to enable epidemiologists to understand the nature of MRSA isolates in this part of India. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06006f1.jpg] [mb06006t2.jpg] [mb06006t1.jpg] [mb06006f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}