 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 24, No. 1, January-March, 2006, pp. 45-48 Brief Communications Changing trends in the antibiograms of Salmonella isolates at a tertiary care hospital in Hyderabad Lakshmi *V, Ashok R, Susmita J, Shailaja VV Department of Microbiology, Nizam's Institute of Medical Sciences, Hyderabad-500 082, Andhra Pradesh, India Correspondence Address:Lakshmi *V, E-mail:
lgorthi@hotmail.com Code Number: mb06008 Abstract The present study was undertaken to compare the changing trends of antibiograms of Salmonella enterica serovar Typhi and Salmonella enterica serovar Paratyphi A isolates. A total of 80 isolates of salmonella obtained from blood cultures between 2001-2004 were included in the study. Identification and antibiotic sensitivities of the isolates were performed by using mini API (bio Merieux, France). Sixty isolates were identified as Salmonella enterica serovar Typhi and 20 were identified as Salmonella enterica serovar Paratyphi A. More than 67% of S.typhi and 80% of S.paratyphi A isolates were sensitive to chloramphenicol. Sensitivity of S.typhi isolates to cephalosporins was found to have increased from 2001-2004 while that of S.paratyphi A showed a decline. With increasing resistance to ciprofloxacin and the possibility of re-emergence of sensitivity to chloramphenicol, the policy of empirical treatment of enteric fever needs to be rationalized.Keywords: Ciprofloxacin, chloramphenicol, ceftriaxone, nalidixic acid
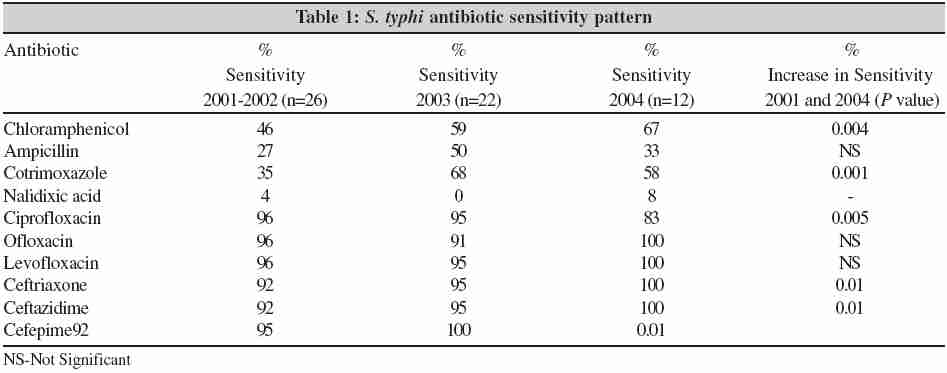
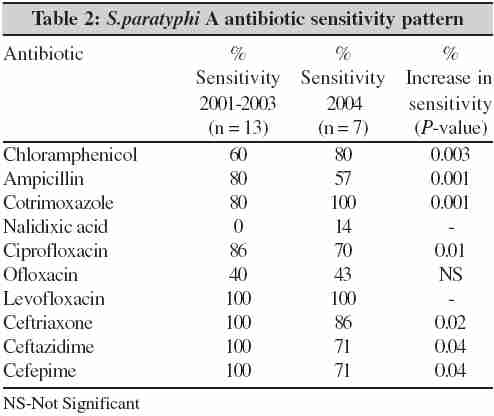
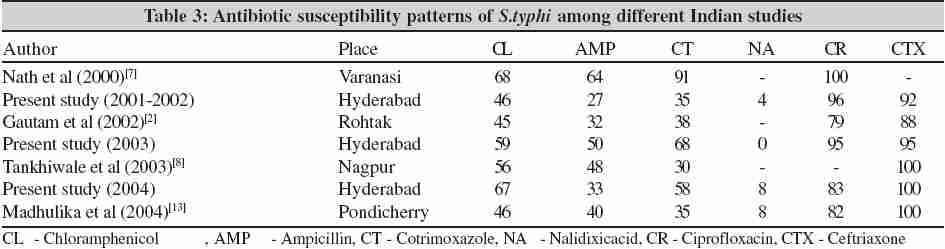
Typhoid fever continues to be a global health problem with an estimated 12 to 33 million cases occurring worldwide each year. The disease is endemic in many developing countries particularly the Indian subcontinent, South and Central America.[1] In India, Salmonella enterica serovar Typhi drug resistance has been reported since 1960 following the first outbreak of multidrug resistant Salmonella enterica serovar Typhi in Calicut. Since then multi drug resistant Salmonella enterica serovar typhi (MDRST) have appeared throughout the world, especially in South America, the Indian sub continent, Africa and South East Asia.[2] Chloramphenicol resistant Salmonella enterica serovar Typhi causing an outbreak has earlier been reported from Chandigarh.[3] Drug resistance in Salmonella is of considerable importance to both clinicians and microbiologists and poses a major problem for public health authorities. Resistance to commonly used antibiotics such as chloramphenicol, ampicillin and cotrimoxazole has been reported from different parts of India.[2] The present study was undertaken to compare the changing trends of antibiograms of Salmonella enterica serovar Typhi and Salmonella enterica serovar Paratyphi A isolates from blood culture between 2001-2004 at our Institute, a tertiary care hospital. Materials and Methods Eighty Salmonella isolates obtained from blood cultures of clinically suspected cases of enteric fever admitted to the Nizam's Institute of Medical Sciences, Hyderabad, Andhra Pradesh, between 2001- 2004, were included in the study. All the 80 isolates were identified and their antibiograms were determined using the mini API ID32E strips and the rapid ATBE antibiotic sensitivity strips for Enterobacteriaceae . The results were analyzed using the mini API (bioMerieux, France).Results Out of 80 Salmonella isolates, 60 were identified as Salmonella enterica serovar Typhi and 20 were identified as Salmonella enterica serovar Paratyphi A. The sensitivity pattern of S. typhi is shown in the [Table - 1] and for S.paratyphi A in [Table - 2].Discussion Enteric fever is a major public health problem in our country. Proper sanitation, public health education and vaccination are long-term preventive measures that would improve this situation. The emergence of antibiotic resistant strains of bacteria is closely linked to the irrational use of antibiotics in treating human infections, especially ciprofloxacin.[2] Since its introduction in 1948, chloramphenicol has been the treatment of choice for typhoid fever and remained the standard against which newer antimicrobials must be compared. Treatment with chloramphenicol reduces mortality due to typhoid fever from approximately 20% to 1% and duration of fever from 14-28 days to 3-5 days.[4] However chloramphenicol therapy has been associated with the emergence of resistance, a high relapse rate, a high rate of continued and chronic carriage, bone marrow toxicity and high mortality rates in some recent series reported from the developing world.[1],[4] Widespread plasmid mediated chloramphenicol resistance emerged in S.typhi in the early 1970s with outbreaks in Mexico, South India, Vietnam, Korea and Thailand.[5] Ampicillin and co-trimoxazole were found to be effective alternative drugs.[6] In the present study S.typhi isolates showed significant increase in sensitivity to chloramphenicol, ampicillin, and cotrimoxazole over the four year study period. Similar findings were reported by Nath et al Tankhiwale et al and Sheorey et al from Varanasi, Nagpur and Mumbai respectively. [7],[8],[9] Probably these drugs could once again be used in the future for enteric fever. [4],[10] However, with the recent threat for emergence of multidrug resistant strains of S.typhi, which show resistance to ampicillin and trimethoprim as well, the efficacy of these drugs is also diminishing.[6] In the recent past, cephalosporins have gained importance for the treatment of enteric infections.[2] Parenterally administered third generation cephalosporins are effective in the treatment of typhoid fever. Ceftriaxone, administered either intravenously or intramuscularly for 10-14 days is equivalent to oral or intravenous chloramphenicol administered for treatment of susceptible S.typhi strains. It is now considered to be the first drug of choice for the treatment of enteric fever unless the in vitro susceptibility tests prove otherwise. First and second generation cephalosporins are ineffective and should not be used to treat typhoid fever. [2] In the present study, the S. typhi isolates showed an increased sensitivity to third and fourth generation cephalosporins, from 92 to 100% (P - 0.01), as was also observed by Nath et al from Varanasi and Gautum et al from Haryana.[2],[7] Ceftriaxone and cefixime are both effective in typhoid fever, including nalidixic acid resistant infections. However, the resolution of fever and symptoms is slow and short course chemotherapy has not proven satisfactory. The high cost and need for parenteral administration are further disadvantages of cephalosporin therapy.[11] Also, some authors reported treatment failure with these cephalosporins in the recent years.[4] Quinolones are highly effective against salmonellae in vitro . Ciprofloxacin was considered the drug of choice for the treatment of multidrug resistant typhoid, replacing chloramphenicol.[4] Hemalatha et al from Hyderabad, India, reported a sensitivity of 95% to ciprofloxacin in 1999.[12] This was similar to studies from other parts of India. All these reports were about the time when the drug was introduced into the market, i.e., during the early part of 1990s. Consequent to the widespread use of ciprofloxacin especially in the community, resistance and treatment failures were being increasingly observed and reported. The minimum inhibitory concentration (MIC) to the drug was reported to steadily increase from 0.025 to 0.5 µgm/mL.[4],[11] Gautum et al from Haryana reported a decrease in sensitivity pattern of S. typhi to ciprofloxacin from 89% to 81% (1997 to 2001).[2] The present study also documents similar findings, from 96% in 2001 the sensitivity to ciprofloxacin dropped significantly to 83% by 2004 (P- 0.005). Nalidixic acid resistance is a marker for predicting low-level resistance to ciprofloxacin among S.typhi a nd also an indicator of treatment failure to ciprofloxacin.[4],[10] Hence, it is suggested that all S.typhi isolates should be screened for nalidixic acid resistance along with ciprofloxacin.[4] Any isolate that shows resistance to nalidixic acid should be reported as intermediately susceptible to ciprofloxacin. The clinician should be advised to change the antibiotic.[13] Such strains have been found to be endemic in different parts of the world including India.[4] All patients with nalidixic acid resistant strains should be treated with higher doses of ciprofloxacin or ofloxacin. Rodrigues et al reported 82 - 88% resistance to nalidixic acid among their isolates with an associated increase in MIC to ciprofloxacin from 0.125 to 1.5 µgm/mL.[10] In our study, 92 - 96% isolates were resistant to nalidixic acid. However, the mini API system that we used for interpreting the susceptibility results, follows the NCCLS guidelines and does not incorporate the analysis with reference to the relation between nalidixic acid and ciprofloxacin resistances in its expert system. Hence, in [Table - 1], ciprofloxacin sensitivity is shown to be high (83 - 96%) inspite of very high resistance to nalidixic acid among the S.typhi isolates. Madhulika et al who also found a high resistance to nalidixic acid (92%), documented high MICs (>0.5 µgm/mL) to ciprofloxacin in majority of their isolates.[13] Probably we have to further determine the exact MICs of all our S.typhi isolates to ciprofloxacin to document the true susceptibility to ciprofloxacin, which would be of clinical relevance. Like the S.typhi isolates, the S.paratyphi A isolates also showed a significant increase in the sensitivity pattern to chloramphenicol from 60 to 80% (P-0.003), similar to the findings from Mumbai.[9] Though the latter reported a decreased sensitivity of S.paratyphi A to cotrimoxazole, an increased sensitivity to cotrimoxazole from 80 to 100% was observed among our isolates. Sensitivity of S.paratyphi A to Ampicillin was also decreased in the present study (80 to 57%). Gautum et al from Haryana reported a decrease in the sensitivity pattern of S.paratyphi A to Ciprofloxacin from 93% to 83%.[2] Similar findings were observed in the present study also, with the sensitivity reducing from 86% to 70% (P-0.01). A decreased sensitivity of the S.paratyphi A isolates to cephalosporins (third and fourth generation) was also observed. Gautum et al reported similar findings from Haryana to third generation cephalosporins.[2] A comparison of reports on the sensitivity patterns of S.typhi documented from other regions of India between 2002 and 2004 were attempted [Table - 3]. All the studies indicate that there is a definite change in the antibiogram of S.typhi isolates through out the country. With increasing resistance to fluoroquinolones (ciprofloxacin) and the possibility of re-emergence of sensitivity to chloramphenicol among Salmonellae , the policy of empirical treatment of enteric fever needs to be rationalized. The changing trends in the antibiograms of S.typhi and S.paratyphi A , probably demands reconsideration for the use of chloramphenicol in typhoid fever, instead of ciprofloxacin or third and fourth generation cephalosporins to prevent the emergence of multidrug resistance. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06008t2.jpg] [mb06008t1.jpg] [mb06008t3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}