 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
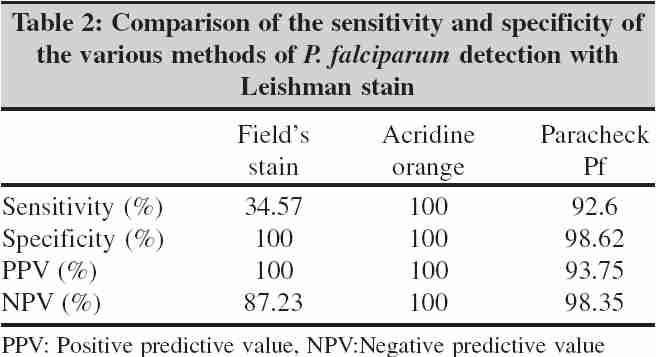
Indian Journal of Medical Microbiology, Vol. 24, No. 1, January-March, 2006, pp. 49-51 Brief Communications Evaluation of different methods for diagnosis of P. falciparum malaria Mendiratta DK, Bhutada K, Narang R, Narang P Department of Microbiology, Mahatma Gandhi Institute of Medical Sciences, Sevagram - 442 102, Maharashtra, India Correspondence Address: Department of Microbiology, Mahatma Gandhi Institute of Medical Sciences, Sevagram - 442 102, Maharashtra Code Number: mb06009 Abstract Rapid diagnosis is a prerequisite for institution of effective treatment and reducing the mortality and morbidity of falciparum malaria. This study was taken up to compare the efficacy of various rapid methods viz, acridine orange, Plasmodium falciparum histidine rich protein II antigen detection and Field's stain with traditional microscopy i.e., Leishman stain for diagnosing falciparum malaria. Thick and thin blood films of 443 consecutive patients with history of fever with chills and rigors were examined by Leishman and Field's method. Acridine orange stained wet mounts of blood were examined under fluorescence microscopy. All films were examined by two independent microbiologists. Plasmodium falciparum histidine rich protein II antigen was detected using commercially available kit, Paracheck Pf. Out of the 443 subjects examined for P.falciparum 18.28% were detected by Leishman stain, 6.32% by Field's stain, 18.28% by acridine orange and 18.1% by antigen based technique. Field's stain missed 53 (65.4%), while Paracheck Pf was negative in 6(7.4%) of the Leishman positive samples. All Field's stain and acridine orange positives were positive by Leishman, but five Paracheck Pf positives were negative. Leishman stain is cost effective but if facilities are available one should use acridine orange for screening. The antigen detection kits are rapid, simple and are useful but to rule out false negatives in clinically suspected cases, Leishman stain is reliable.Keywords: P. falciparum, rapid methods
Malaria causes 1.5 to 2.7 million deaths each year world wide.[1] It continues to be one of the major health problems in the developing world. The increasing incidence of falciparum malaria, the need to identify and treat the additional infective carriers (reservoirs) and to reduce the chances of transmission has given an impetus for development of simple and rapid methods for the diagnosis of falciparum malaria. Conventional Leishman, Giemsa or Romanowsky's stained peripheral blood smear examination remain the gold standard for diagnosis of malaria in malaria endemic countries. Conventional light microscopy has the advantages that it is sensitive, informative, relatively inexpensive, provides permanent record and can be shared with other disease control programmes. However, it suffers from disadvantages such as it is labour intensive and time consuming.[2] In recent years, numerous rapid techniques like acridine orange (AO) stain,[3] quantitative buffy coat (QBC)[4] and detection of soluble histidine rich protein II antigen (HRP II Ag) in whole blood have been evaluated in an attempt to diagnose falciparum malaria as early as possible. HRP II antigen is released by erythrocyte infected with Plasmodium falciparum and Orchid Biomedical Systems (Paracheck Pf) and Span Diagnostics Ltd (Parahit) have developed commercial kits to detect this antigen by immunochromatography. However , previous studies have compared the sensitivity of these techniques (AO, QBC and HRP II Ag) individually with Leishman stain. In the present study, we compared these and Field's stain with the gold standard Leishman stain to evaluate their sensitivity in detecting falciparum malaria parasite . Materials and Methods The study was conducted in the department of microbiology, Mahatma Gandhi Institute of Medical Sciences, Sevagram, between September 1, 2003 and June 30, 2004. One millilitre of blood in EDTA bulb was collected from 443 consecutive subjects who were clinically suspected to be suffering from malaria. The study was cleared by institutional ethics committee and written consent from the patients was taken prior to collection of blood. Antigen detection All samples were subjected to antigen detection using Paracheck Pf kit (Orchid Biomedicals Systems) as per kit instructions. The strip of this kit is coated with anti HRP II antibody and this detects the presence of the HRP II antigen by immuno-chromatography. All kit components were brought to room temperature. The anticoagulated blood sample was mixed by gentle swirling. The sample loop was dipped in the sample and the blood so collected was blotted on the sample pad just below the rows on to the dipstick (approximately 5 μL of the whole blood specimen). The dipstick (arrows facing downwards) was then placed in a test tube containing four drops (200μL) of the clearing buffer, ensuring that the buffer level is below the blood sample for the entire duration of the test. At the end of fifteen minutes results were read as: negative for P.falciparum if only one pink band appeared and positive for P.falciparum if two distinct bands appeared. The test was considered invalid if no bands appeared and results were not read after 15 minutes. Staining Leishman and Field's method Thick and thin blood films were prepared on four slides. Two slides each were stained by Leishman [4] and Field's stain.[4] Acridine orange[3] Seventy five μL of blood was mixed with 10μL of acridine orange stain on a glass slide and covered with a cover slip. The cover slip was pressed slightly and the preparation was examined under fluorescence microscope (exciter filter: LP 450 and barrier filter: LP 520). The ring stage, trophozoites and gametocytes appeared pale apple green under the fluorescence microscope. All stained slides (Leishman and fluorescence) were screened by two microbiologists independently. Results There was 100% correlation in the interpretation of slides, both with respect to positivity and negativity, between the two microbiologists. Of the 443 subjects, 18.28% (81) were positive for falciparum malaria by Leishman stain, 6.32% (28) by Field's stain, 18.28% (81) by AO and 18.1% (80) by Paracheck kit [Table - 1]. Field's stain failed to detect 65.4% (53) of the positives, while Paracheck method failed to detect 6(7.4%) cases [Table - 1]. All those positive with Field's stain and AO were also positive with Leishman stain, however Paracheck Pf detected five positives that were negative by Leishman stain [Table - 1]. The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of AO with respect to Leishman stain was 100% [Table - 2]. The sensitivity of Field's stain was low (34.57%) but its specificity was 100%. The sensitivity and specificity of Paracheck Pf was 92.6% and 98.6% respectively with respect to Leishman stain [Table - 2]. Discussion Rapid detection and effective treatment of falciparum malaria is a prerequisite in reducing the morbidity and mortality due to the disease. Leishman stained blood smear examination, which is the cornerstone in the laboratory diagnosis of malaria, has undergone little improvement since its inception. This is labour intensive and time taking and therefore delays diagnosis.[2] In the present study, while comparing the available different methods of rapid detection of parasites with gold standard Leishman stain, the sensitivity of Field's stain was found to be the lowest (34.57%), which may be because of the undefined ring stage of the parasite. Modified acridine orange stain correlated well with traditional Leishman stain (100% sensitivity and specificity, NPV and PPV). Hemvani et al [3] found acridine orange (AO) to be better than Leishman stain as they detected 248 cases by AO against 148 by the latter. Acridine orange has the advantage that screeing is much faster. However, it requires a fluorescence microscope which is expensive and the AO stained wet mounts cannot be preserved, unlike the Leishman stained smear. We also studied the usefulness of HRP II antigen detection kit Paracheck Pf for the rapid diagnosis of falciparum malaria. The sensitivity (92.6%) and specificity (98.65%) of this test kit observed in the present study was well comparable to that reported by many other authors (sensitivity 66-100% and specificity 98-100%).[5],[6],[7],[8],[9] However, Paracheck Pf was positive in five cases which were negative by Leishman staining. In retrospective case analysis of these five cases it was found that four of these never received any antimalarial treatment either for the present illness or in the past one month. Paracheck Pf was requested from them as routine to eliminate falciparum malaria infection, as they were suffering from fever. The fifth case (who responded to anti malarial treatment) probably had the parasite sequestered and this prevented its detection in peripheral blood smear by traditional method but HRP II could be detected by paracheck Pf.[10] One should bear in mind that HRP II has been shown to persist in blood for 7-14 days and up to 28 days[11] following antimalarial therapy, hence it is important to be familiar with the history of antimalarial treatment of the individual patient to rule out false positives. The six Paracheck Pf negative Leishman positive cases [Table - 1] were probably false negatives as ICT is unable to detect HRP II below 100 parasites/μL of blood.[12] The positivity of paracheck Pf depends on number of parasites per microlite of blood. Immunochromatography is unable to detect HRP II Ag when the number of parasites are less than 80 per μL of blood.[12] Christian et al[13] reported that if parasitaemia is more than 60 parasites/μL of blood, the dipsticks gave a sensitivity of 96.5 - 100% and this fell to 11 - 67% with 10 parasites/μL of blood. In the present study, six Paracheck Pf negative but Leishman positive cases [Table - 1] were in fact false negative by Paracheck Pf as the ICT kit was unable to detect HRP II Ag, the number of parasite per microlite of blood being low. We also tested 50 samples with another HRP II Ag detection test kit (Parahit-Span diagnostics) and found its results to be the same as that of Paracheck Pf, however, the positive results with Parahit appeared within four minutes as compared to nine minutes by Paracheck. In addition, cost per test was less with Parahit dipstick test. It is concluded that if facilities are available (equiptment and expertise) AO, should be used for screening. HRP II antigen detection kits are rapid, do not require expertise and can detect P. falciparum infection when the parasites are sequestered, hence, are useful in routine diagnosis (where cost is not a problem) and in emergency. However, there is need to confirm clinically suspected but HRP II negative, especially when level of parasitaemia is 60-80 parasites/ml or less. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06009t1.jpg] [mb06009t2.jpg] |
| |||||||||
{kind=link}
{kind=link}