 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
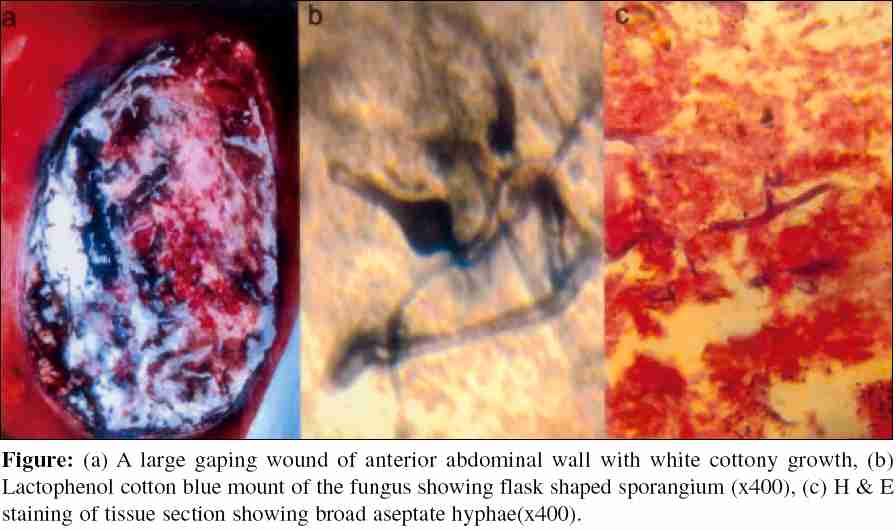
Indian Journal of Medical Microbiology, Vol. 24, No. 1, January-March, 2006, pp. 58-60 Case Report Cutaneous zygomycosis - Necrotising fascitis due to Saksenaea vasiformis Padmaja *IJ, Ramani TV, Kalyani S Department of Microbiology, Andhra Medical College, Visakhapatnam - 530 002, Andhra Pradesh, India Correspondence Address: Padmaja *IJ, E-mail: j_indugula@yahoo.co.in Code Number: mb06012 Abstract Saksenaea vasiformis is an emerging human pathogen, most often associated with cutaneous or subcutaneous lesions following trauma. This is the report of a case of subcutaneous zygomycosis from which Saksenaea vasiformis was isolated on culture. As the patient developed acute interstitial nephritis, amphotericin B could not be administered in full dose. Surgical debridement was carried out, but the patient deteriorated gradually and died. To the best of our knowledge, this is the first reported case of Zygomycosis due to Saksenaea vasiformis from Visakhapatnam.Keywords: Saksenaea vasiformis, zygomycosis, lactophenol cotton blue, Sabouraud dextrose agar, potassium hydroxide.
Among the zygomycetes there are two orders that contain genera and species of medical importance - the Mucorales and Entomophthorales. In general, fungi in the order Mucorales, cause more severe forms of disease.[1] Most of the species known to cause human or animal infections belong to a few genera within the family Mucoraceae . Members of several other genera belonging to other families such as Cunninghamellaceae, Mortierellaceae and Saksenaeceae are also occasionally reported. Since the 1980s, nosocomial zygomycosis manifesting as primary skin and wound infections caused by Rhizopus spp , Absidia, Cunninghamella , Saksenaea vasiformis and Apophysomyces elegans are often being reported. Zygomycosis may manifest as rhinocerebral, pulmonary, abdominal, pelvic, cutaneous and disseminated forms. The monotypic genus Saksenaea was described by Saksenaea in 1953 based on isolates from soil in India.[2] It has been isolated in soil samples from other geographic areas. Vasiformis is the only species. The first human infection with Saksenaea vasiformis was described by Ajello et al in 1976. The key features of Saksenaea vasiformis are the formation of flask shaped sporangia and failure to sporulate on primary isolation media. Sporulation may be induced by the use of nutrient deficient media or Czapek Dox agar or by using agar block method described by Ellis and Ajello. Colonies are fast growing, white with no pigment on the reverse, Hyphae are broad, aseptate and the sporangia are typically flask shaped with a distinct spherical center and long neck arising singly or in pairs from dichotomously branched darkly pigmented rhizoids. Columellae are dome shaped and sporangiospores are small, oblong 1-2 x 3-4 mm in size and are discharged thorough the neck after the dissolution of an apical mucilaginous plug. Saksenaea vasiformis is most often associated with cutaneous or subcutaneous lesions after trauma. It has also been associated with rhinocerebral infection, cranial infection, osteomyelitis, necrotising cellulitis and disseminated type of infection. Case Report A male patient aged 35 years, working as a constable in a tribal area of Visakhapatnam district was brought to the emergency service of King George Hospital with complaints of pain abdomen, vomitings and fever of one day duration. A history of similar complaint in the past was present and a provisional diagnosis of acute appendicitis was made. The patient was admitted to surgical unit and an emergency appendisectomy was done under spinal anaesthesia. A gangrenous appendix with minimal periappendicular collection was noticed, he was under an antibiotic coverage of i.v metrogyl and ciprofloxacin pre and post operatively. The postoperative period was uneventful till the fourth postoperative day except for a mild soiling of the dressing at the drain site on the fifth post operative day. Induration and oedema were noticed at the incision site and the patient complained of pain. Sutures were removed on the seventh postoperative day and the incision site showed induration and oedema extending for about 7cms around the incision. There was blistering of the skin, the skin edges were becoming gangrenous and a gaping wound with white cottony growth was observed [Figure - 1] a. By the tenth postoperative day a rapid spread involving skin and subcutaneous tissue and areas of necrosis were noticed. The patient was afebrile, there was complaint of pain and burning sensation at the wound site. An emergency slough excision was done and bits of excised skin and subcutaneous tissue were sent for bacteriological and fungal culture and for histopathological examination. The material was processed by potassium hydroxide (KOH) mount, lactophenol cotton blue (LPCB) mount, Gram stain and culture for bacteria and fungus. KOH and LPCB preparations showed broad, aseptate fungal hyphae and fat globules. Grams stain revealed aseptate, broad hyphae and no bacteria were seen. Bacterial culture yielded no growth. There was no growth on Sabouraud dextrose agar (SDA) with actidione, however, SDA without actidione at 22o C showed growth after 48 hours. The fungal colony was cottony and white. A LPCB mount from this growth showed only broad aseptate hyphae. No sporulation could be observed. Subculture on cornmeal agar and fresh SDA also failed to accomplish sporulation. Saksenaea / Apophysomyces were considered as a possibility and subculture was made on to 1% saline agar and 1% water agar. Agar block technique was adopted to achieve sporulation by floating the agar block containing subculture in distilled water. Mycelial growth could be observed extending from the agar block into distilled water in 72 hours. LPCB mount from agar block showed broad aseptate ribbon like hyphae characteristic of Zygomycetes and typical flask shaped sporangium with columella short sporangiophore and darkly pigmented rhizoids [Figure - 1] b. Depending on the typical morphology the fungus was identified as Saksenaea vasiformis . Haematoxylene and eosin staining of tissue section also showed broad aseptate ribbon like hyphae and areas of necrosis [Figure - 1] c. The patient remained afebrile throughout. The infection extended from the McBurneys incision to infraclavicular region. His blood sugar and blood counts were within normal limits. His serum tested nonreactive for antibodies to HIV. Serum creatinine was 4 gms and there was persistant hypertension. He was referred to nephrology where he was diagnosed as having acute interstitial nephritis and was put on 50% dose of amphotericin B. Emergency debridement was planned, but the patient was not willing for high risk and left the hospital against medical advice. He was later admitted to a private hospital where he passed away. Discussion Cutaneous infections account for 16% of all forms of zygomycosis, with an associated mortality of 16%, compared to 67% for rhinocerebral, 83% for pulmonary and 100% for disseminated infection. Saksenaea vasiformis and Apophysomyces elegans differ from other pathogenic zygomycetes species by their failure to sporulate on media routinely used in mycology laboratory like SDA, potato dextrose agar and corn meal agar. Czapek dox agar and agar block culture have been used for their identification.[3] Most of the reported infections caused by Saksenaea vasiformis are subcutaneous, with only two being disseminated and one rhinocerebral infection reported. [4] Cutaneous lesions may be primary or secondary, representing haematogenous dissemination from some other primary site. In the primary disease, the infection may occur at the site of a barrier break such as in surgery or an indwelling catheter. In an immunosuppressed patient infection may become rapidly disseminated and require much more aggressive management. Fatal disseminated infection with Saksenaea vasiformis in an immunocompromised woman has been reported by Torell J et al[5] and in a immunocompetent child by Hay RJ et al[6]. Subcutaneous infections have been reported in a three month old infant and an eleven year old thalassemic child, who were successfully treated. Cases of tissue invasion with Saksenaea vasiformis following traumatic injury have been reported by several workers.[7] The first case of subcutaneous zygomycosis caused by Saksenaea vasiformis in India was reported by Padhye et al[8] in a rice mill worker in 1988. The infection involved the foot with multiple sinuses. Amputation of the fore-part of the foot followed by a split thickness graft and treatment with potassium iodide cured the infection. Primary cutaneous zygomycosis due to Saksenaea vasiformis has subsequently been reported from Chandigarh in 1997.[9] In an immunocompetent patient infection usually remains localized around the site of initial trauma and responds well to local debridement and antifungal therapy. The present case has been an acute infection with lesions appearing and progressing rapidly. There was no systemic illness which might have predisposed to the present condition and there was no evidence of immunosupression. Sporulation was induced by the agar block method. Though an early diagnosis was made and debridement carried out amphotericin B could not be administred in full dose because of the acute interstitial nephritis and the patient was lost. Disseminated infection due to Saksenaea vasiformis in an immunocompetent adult which was fatal has been reported by Solano et al in 2000.[10] Saksenaea vasiformis is increasingly being reported as a cause of subcutaneous zygomycosis. Cutaneous zygomycosis generally has a favourable outcome, zygomycosis due to Saksenaea vasiformis has also been reported to have a favourable outcome after treatment in most of the cases, though at times it can cause a fatal infection, as in the present case. Hence when a zygomycetes species which fails to sporulate on routine media is isolated, the isolate should be cultured on nutritionally deficient media to induce sporulation so as to enable quick identification and to start treatment properly. In an immunocompetent individual with localized cutaneous lesions, surgical debridement alone is often sufficient, but aggressive debridement and i.v amphotericin B are definitely indicated in severe cases. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06012f1.jpg] |
| |||||||||
{kind=link}